
Nutrition Guideline
Page 1
Revised January 2024
© 2024 Alberta Health Services, Nutrition Services.
This copyright work is licensed under the Creative Commons Attribution-Non-Commercial-No Derivatives 4.0 International License
except where otherwise indicated. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/ You are free to copy and distribute
the work including in other media and formats for non-commercial purposes, as long as you attribute the work to Alberta Health Services, do not adapt the
work, and abide by the other licence terms. The licence does not apply to AHS trademarks, logos or content for which Alberta Health Services is not the
copyright owner.
This material is intended for general information only and is provided on an "as is", "where is" basis. Although reasonable efforts were made to confirm the
accuracy of the information, Alberta Health Services does not make any representation or warranty, express, implied, or statutory, as to the accuracy,
reliability, completeness, applicability or fitness for a particular purpose of such information. This material is not a substitute for the advice of a qualified health
professional. Alberta Health Services expressly disclaims all liability for the use of these materials, and for any claims, actions, demands or suits arising from
such use.
Introduction
The purpose of this Nutrition Guideline (NG) is to provide care providers with an overview of
the evidence-based nutrition recommendations for individuals who are pregnant and provide
answers to commonly asked questions (See Key Questions List).
In North America, it is estimated that approximately half of pregnancies are unplanned.
1
It is
recommended that all people who could become pregnant maintain good nutrition.
Pregnancy is a critical period in a person’s life that can influence the short and long-term
health of both the parent and infant.
The health benefits of good nutrition intake during pregnancy include reducing the risk of:
• neural tube defects
2
• low-birth-weight infants, small for gestational age infants, and preterm births
2
• chronic health problems in both the parent and child
3
The NG was developed by the Nutrition Services Public Health Provincial Target Population
Reproductive Health Working Group and is based on scientific evidence and best practice. It
was reviewed by health professionals across the province. If you have questions about this
NG, please contact publichealth.nutrition@ahs.ca
.
This information is intended as a general resource only and is not meant to replace the
medical counsel of a physician or individual consultation with a registered dietitian (RD). It is
the responsibility of care providers to evaluate the situation of each client in their care and
apply the NG appropriately. Individuals who are at high risk of malnutrition or who have a
medical condition that is impacted by nutrition should be referred to an RD.
Pregnancy

Nutrition Guideline
Revised January 2024
Page 2
Pregnancy
Scope of this Guideline
The scope of this guideline covers the following:
• individuals who could become pregnant
• individuals pregnant with singletons
• all ages of people who are pregnant, including adolescents
Additional information for the following specific populations may be found here:
• Nutrition Guideline: Diabetes in Pregnancy
• Nutrition Guideline: Pregnancy: Multiples
Referral to a Registered Dietitian
For more information on referral to an RD and RD services available in Alberta Health
Services (AHS), visit Referring Clients for Nutrition Services
Note: For purposes of this Nutrition Guideline, the single term client will be used to refer to
clients, patients, and residents.
Inclusive Language
Some expectant parents may not identify as women or as female but as male, non-binary, or
gender diverse. In all circumstances, care providers shall utilize client and family-centred
care to be responsive to the individual context, self-identified gender, pronouns, and
preferred terminology of the families they support.
The language used within this NG is based on the Academy of Breastfeeding Medicine
Position Statement
4
and AHS Best Practices.
5
A variety of terms are used for accuracy and
clarity.
• non-gendered terms (e.g., person, individual) are used, when possible, to be inclusive.
• gendered terms (e.g., female, woman) used in the source being cited, are noted
throughout by “α”, and replaced with inclusive language, where appropriate, and align
with the greater body of scientific evidence.

Nutrition Guideline
Revised January 2024
Page 3
Pregnancy
Recommendations
• Individuals who could become pregnant are encouraged to:
o eat a variety of food every day and make healthy eating and physical activity part of
everyday life.
o take a multivitamin supplement that contains 0.4 mg (400 mcg) folic acid every day.
It is recommended to start supplementation at a minimum of three months before
conception.
o maintain a healthy body weight before and between pregnancies.
• During pregnancy, individuals are advised to:
o eat a variety of foods and follow Canada’s food guide.
o include additional foods every day in the second and third trimesters of pregnancy
in amounts appropriate to meet healthy pregnancy weight gain recommendations
for their pre-gravid body mass index (BMI) category.
o take a multivitamin. Health Canada recommends taking a multivitamin with folic
acid (0.4 mg), iron (16–20 mg), vitamin D (400 International Units [IU]) and vitamin B
12
every day. These exact amounts can be hard to find. When assisting an individual
who is pregnant in choosing a multivitamin, look for this information on the label as
these levels are safe:
Iron: between 16–27 mg
Vitamin D: at least 400 IU (10 mcg)
Folic acid (folate): between 0.4–1 mg (400–1000 mcg)
Vitamin B
12
: 2.6 mcg
o follow safe food handling practices and avoid foods that increase the chances of
getting a food-borne illness during pregnancy.
o limit caffeine intake to 300 mg/day.
o drink 10 cups (2.5 L) fluid each day. Water is recommended as the main fluid.
• Care providers are advised to offer individuals who are pregnant nutrition information
that will help them make informed choices about:
o healthy pregnancy weight gain.
o nutrients of special concern during pregnancy (e.g. folic acid, iron, calcium).
o nutrient supplements.
o beverage and fluid choices.
o general food safety and food items to limit or avoid during pregnancy.
o managing common discomforts of pregnancy (e.g. nausea and vomiting of
pregnancy).

Nutrition Guideline
Revised January 2024
Page 4
Pregnancy
Referral for nutrition assessment/counselling by an RD is appropriate for people who:
• are adolescents.
• are pregnant with twins, triplets, or higher-order multiples.
• previously had a low-birth-weight infant.
• had a low pre-pregnancy BMI.
• have a poor weight gain in the second or third trimester.
• have a nutrition-related health condition, such as inflammatory bowel disease (IBD),
post-bariatric surgery, celiac disease, gestational diabetes, and pre-eclampsia.
Definitions
Congenital anomalies: Anomalies, either structural or functional (e.g. metabolic disorders)
that occur during gestation. Also known as birth defects, congenital disorders, or congenital
malformations.
6
Cultural competence: The ability of health care systems and practitioners to provide high-
quality, safe, client-centred care to clients with a wide range of unique values, beliefs and
behaviours.
7
Fortified: Fortification refers to “the addition of one or more vitamins or minerals to a food
product”.
8
Gestational hypertension: First onset of hypertension after 20 weeks gestation (diastolic
blood pressure greater than 90 mm Hg or systolic blood pressure greater than 140 mm Hg).
9–11
Herbal teas: These are beverages made with fresh or dried flowers, leaves, seeds, or roots
from different kinds of plants. Climate, growing conditions, storage conditions, and
processing (e.g. extraction and drying) can influence the content and concentration.
12
Intrauterine growth restriction (IUGR): Fetus with an estimated fetal weight less than the
10
th
percentile on ultrasound, that, because of a pathological process, has not attained its
biologically determined growth potential.
13
Large for gestational age (LGA): Weight above the 90
th
percentile for gestational age.
14
Low birth weight (LBW): A baby that weighs less than 2500 g at birth. A baby may weigh less
than 2500 g at birth because it is born too soon or because it is small for its gestational age.
15
Miscarriage: Loss of a pregnancy before fetal viability.
16
Fetuses that die in utero before
20 weeks gestation are categorized as miscarriages.
17
Multivitamin supplement: Terminology used to describe a supplement containing multiple
vitamins and minerals. The terminology ‘prenatal multivitamin’ is not used due to the wide
variation in supplements available for people who are pregnant.

Nutrition Guideline
Revised January 2024
Page 5
Pregnancy
Natural product number (NPN): An 8-digit numerical code assigned to each natural health
product approved to be marketed under the Natural Health Products Regulations.
18
Neonatal death: Infant death within the first 27 days of life.
19
Nutrient-dense: Relatively rich in nutrients for the number of calories the food contains.
Perinatal: The perinatal period commences at 22 completed weeks (154 days) of gestation
and ends 7 completed days after birth.
15
Phytates: Antioxidant compounds found in whole grains, legumes, nuts, and seeds. Phytates
can bind to dietary minerals iron, zinc, manganese and, to a lesser extent calcium, and slow
their absorption.
20
Plant-based beverage: A beverage made from plant bases such as soy, rice, almond, etc.
21
Preterm birth: Defined as birth before 37 weeks of gestation.
16
Pre-eclampsia: Hypertension that develops during gestation with proteinuria and/or one or
more adverse conditions or severe complications (e.g. symptoms, signs of end-organ
dysfunction, and/or abnormal laboratory testing on a person who is pregnant, fetal
morbidity).
11,22,23
Pre-existing hypertension: High blood pressure that develops either pre-pregnancy or at
less than 20 weeks gestation.
9–11
Probiotics: Live microorganisms (bacteria or yeast) that, when administered in adequate
amounts, confer a health benefit on the host.
24
Probiotics are labelled by genus, species, and
strain.
Regular teas: These are beverages made from the shrub Camellia sinensis. Some examples
of teas are: black, white, green, oolong, jasmine, Formosa, Ceylon, India, and Darjeeling.
25
Small for gestational age (SGA): Weight below 10th percentile for gestational age.
1
Spontaneous abortion: A clinically recognized pregnancy loss before the 20
th
week of
gestation. Also known as miscarriage.
26
Stillbirth: The term used to describe fetal deaths at 20 weeks gestation or more.
17
The World
Health Organization defines stillbirth as at or after 28 weeks gestation.
27
Very-low birth weight: Birth weight less than 1500 g (up to and including 1499 g), regardless
of gestational age.
28

Nutrition Guideline
Revised January 2024
Page 6
Pregnancy
Key Questions List
Key nutrition questions related to pregnancy that are addressed in this NG are listed below.
Weight Gain During Pregnancy
• How does weight affect pregnancy outcomes?
• How much weight gain is appropriate during pregnancy?
• Is weight loss ever recommended during pregnancy?
Healthy Eating During Pregnancy
• Do people need to eat more during pregnancy?
• What nutrients are important during pregnancy?
o Folic acid
o Calcium and vitamin D
o Iron
o Omega-3 fatty acids
o Choline and iodine
Vegetarian Eating Patterns During Pregnancy
• Are there any extra considerations for vegetarian eating patterns?
Nutrient Supplements During Pregnancy
• What are the recommendations for a multivitamin supplement for pregnancy?
• What is the difference between a multivitamin and a ‘prenatal vitamin’?
• Are there benefits of taking a multivitamin compared to single-nutrient supplements?
• What if an individual who is pregnant requires higher amounts of iron or folic acid?
Other Nutrient Supplements
• Is the use of Lucky Iron Fish
TM
recommended to improve iron status during pregnancy?
• What advice can be given about omega-3 fatty acid supplements during pregnancy?
• Are protein supplements required during pregnancy?
• What is the concern with vitamin A supplements in pregnancy?
• What about the use of other supplements during pregnancy?

Nutrition Guideline
Revised January 2024
Page 7
Pregnancy
Beverage and Fluid Intake During Pregnancy
• How much fluid is needed during pregnancy?
• What are plant-based beverages and are they a nutritious choice during pregnancy?
• What is considered a safe intake of caffeine during pregnancy?
• What is the recommendation for caffeinated energy drinks during pregnancy?
• Are sugary drinks recommended during pregnancy?
• What herbal teas are considered safe to consume during pregnancy?
• Are nutrition supplement drinks needed during pregnancy?
Food Safety During Pregnancy
• Why is foodborne illness a concern during pregnancy?
• What is the best way to reduce the risk of foodborne illness during pregnancy?
• What foods are people advised to avoid during pregnancy and are there safer
alternatives?
• Is it safe to consume fish during pregnancy?
• What are the food safety concerns with cheese and what are safe cheese choices?
• What are other food-related safety considerations?
Common Discomforts of Pregnancy Considerations
• Nausea and vomiting – what can be done during pregnancy?
• Constipation – what can be done during pregnancy?
• Heartburn – what can be done during pregnancy?
Health Condition Considerations in Pregnancy
• Are there special nutrition considerations regarding diabetes in pregnancy?
• Are there nutrition considerations for hypertensive disorders of pregnancy?
• Are there recommended foods to avoid or eat during pregnancy to prevent infant
allergies?
Adolescent Pregnancy
• What are the nutrients of concern for pregnancy during adolescence?
• What are the recommendations for gestational weight gain in adolescents?

Nutrition Guideline
Revised January 2024
Page 8
Pregnancy
Substance Use During Pregnancy
• Is it safe to consume alcohol during pregnancy?
• Is it safe to consume cannabis during pregnancy?
Physical Activity During Pregnancy
• What needs to be considered when discussing physical activity during pregnancy?
Other Special Considerations
• Are there special considerations when working with individuals with culturally diverse
backgrounds?
• What are other important considerations when working with any individual?
Referral to a Registered Dietitian
• When is a referral to a registered dietitian recommended?
Resources
• What resources are available for professionals?
• What resources are available for the public?

Nutrition Guideline
Revised January 2024
Page 9
Pregnancy
Answers to Key Questions
Weight Gain During Pregnancy Return to Key Questions
How does weight affect pregnancy outcomes?
Weight gain is a normal and important part of a healthy pregnancy.
29
Appropriate weight gain
during pregnancy reduces the risk of complications while pregnant and at delivery and
promotes the long-term health of both parent and child.
1
An individual who does not gain enough weight during pregnancy is at greater risk of having a
low birth weight baby and is also at increased risk of preterm delivery.
1
Dieting and weight
loss are not recommended during pregnancy.
29,30
Studies conducted in Alberta on individuals
α
who are pregnant have documented that
approximately half (49%) of the study participants gained weight above guidelines.
31
Excessive weight gain can be concerning in pregnancy. People who gain excessive amounts
of weight are at increased risk for pre-eclampsia, gestational diabetes, preterm delivery,
cesarean section delivery, and retaining extra weight after delivery.
1
Parental obesity and
excessive weight gain during pregnancy are also associated with large-for-gestational-age
infants.
1
These infants are at increased risk for childhood obesity.
1
How much weight gain is appropriate during pregnancy?
As early in pregnancy as possible, assess pre-pregnancy body mass index (BMI) and provide
an individualized weight gain recommendation based on Health Canada guidelines.
1
Appropriate range of weight gain differs between categories of pre-pregnancy BMI, as
outlined in Table 1
.
1
Minimal weight gain is required in the first trimester of pregnancy for
singleton pregnancies, only 0.5–2.2 kg (1.1–4.4 lbs). The average weekly rate of weight gain
for the second and third trimesters ranges from 0.2–0.5 kg/week (0.5–1.1 lbs/week) depending
on the individual’s pre-pregnancy BMI category.
Monitor weight gain and review progress with clients regularly to help them gain within their
target range.
1,32
AHS has pregnancy weight gain graphs for singletons that can be used for
monitoring weight gain.

Nutrition Guideline
Revised January 2024
Page 10
Pregnancy
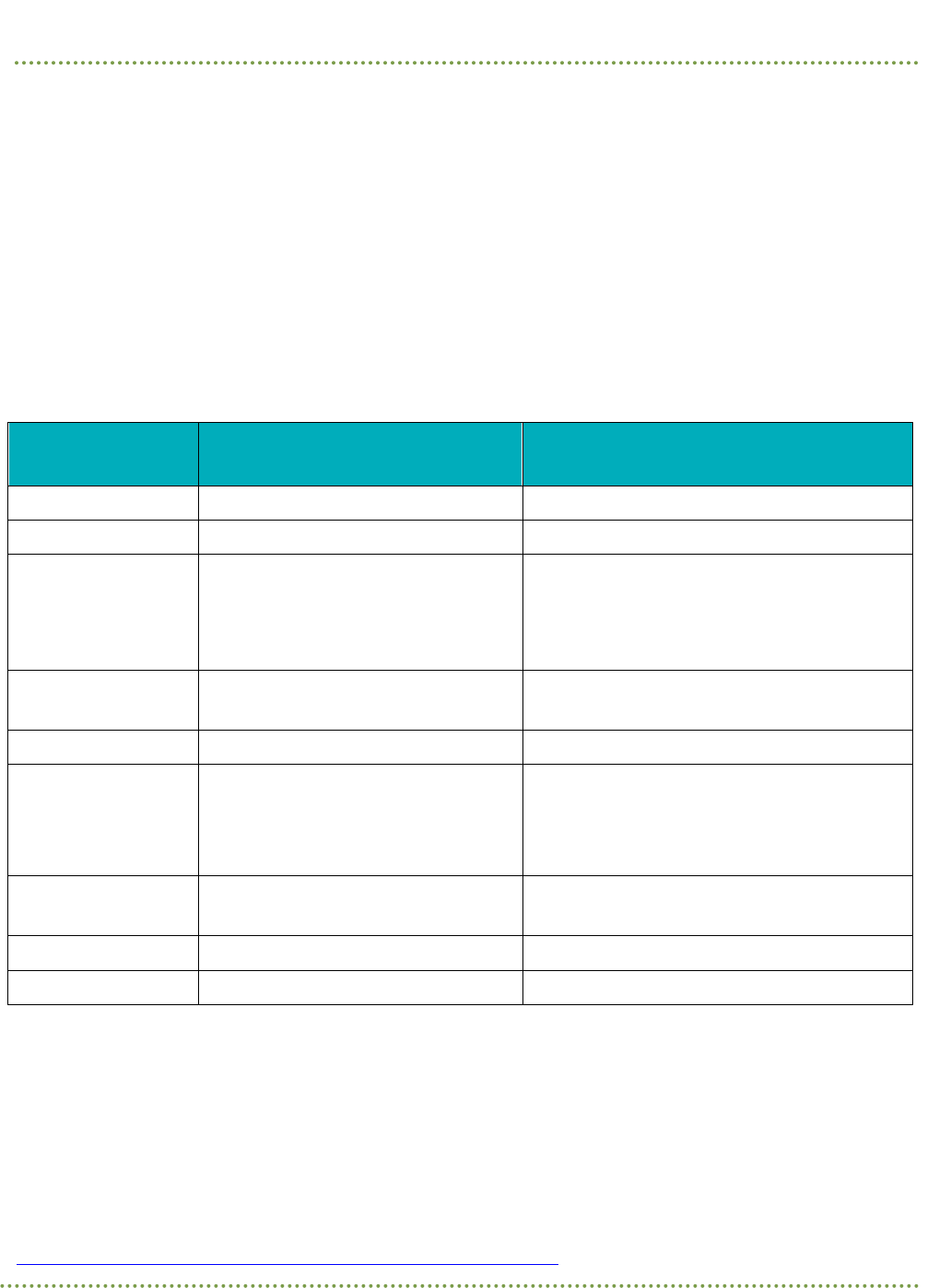
Table 1. Canadian Gestational Weight Gain Recommendations for Singletons
Pre-pregnancy BMI
Recommended Range of Total
Weight Gain During Pregnancy
Average Weekly Rate of
Weight Gain in Second
and Third Trimesters
Kilograms (kg)
Pounds (lbs)
Underweight
BMI less than 18.5 kg/m
2
12.5–18 28–40 0.5 kg (1.1 lbs)
Normal weight
BMI 18.5–24.9 kg/m
2
11.5–16 25–35 0.4 kg (0.9 lbs)
Overweight
BMI 25.0–29.9 kg/m
2
7–11.5 15–25 0.3 kg (0.6 lbs)
Obese
BMI greater than or equal to 30 kg/m
2
5–9 11–20 0.2 kg (0.5 lbs)
Source: Table S 1, New Recommendations for Total and Rate of Weight Gain during Pregnancy, by Pre-pregnancy
BMI, Weight Gain During Pregnancy: Re-examining the Guidelines. Institute of Medicine (US) and National
Research Council (US) Committee to Reexamine IOM Pregnancy Weight Guidelines; Rasmussen KM, Yaktine AL,
2009
32
Further assessment and follow-up is warranted for individuals who are gaining weight outside
of the recommendations.
1
Encourage clients to identify and implement practical, sustainable
healthy behaviours to meet weight gain recommendations.
1
Consider the social determinants
of health when counselling clients as these can impact weight gain in pregnancy.
1
Individuals
who have already surpassed the recommended weight gain can be encouraged to continue
gaining weight at the appropriate rate of gain according to their pre-pregnancy BMI.
29
Individuals who are gaining too much or not enough weight in pregnancy can be referred to an
RD for assessment and counselling.
29
See also:
When is a referral to a registered dietitian recommended?
What resources are available for healthcare providers?
For related Nutrition Guidelines see: Nutrition Guideline: Pregnancy: Multiples
Is weight loss ever recommended during pregnancy?
Weight loss during pregnancy is not recommended for people in any pre-pregnancy BMI
category, including individuals who have a high pre-pregnancy BMI. Individuals in the BMI
category greater than or equal to 30 before pregnancy who experience weight loss during
pregnancy are at increased odds of delivering small-for-gestational-age (SGA) infants.
1
It is
recommended that people follow a weekly rate of weight gain according to their pre-
pregnancy BMI.
29

Nutrition Guideline
Revised January 2024
Page 11
Pregnancy
Healthy Eating During Pregnancy Return to Key Questions
Do people need to eat more food during pregnancy?
People only need modest increases in calories during pregnancy to support their baby’s
growth and development. In the first trimester, no additional calories are required for most
individuals.
Additional food is recommended for individuals of any pre-pregnancy BMI category in the
second and third trimesters. Individuals with a pre-pregnancy BMI between 18.5–24.9 kg/m
2
will require additional energy requirements of approximately 350 calories for the second
trimester and 450 calories for the third trimester.
33
Advise clients that this is a small amount
of additional food, equivalent to a large snack or a small meal. The examples below
demonstrate 350–450 calories from a variety of healthy food choices.
Additional examples of appropriate snacks to meet additional food requirements are available
from Healthy Parents, Healthy Children.
Note that individual energy requirements will vary based on age, pre-pregnancy BMI, and
activity level. Individuals with a pre-pregnancy BMI less than 18.5 kg/m
2
may require
additional food to meet weight gain recommendations. Individuals with a pre-pregnancy BMI
less than or equal to 25 kg/m
2
may require less additional food to meet their recommended
weekly and total weight gain targets. Consider recommending individual consultation with an
RD if there is concern about caloric intake and food choices.
See also:
How much weight gain is appropriate during pregnancy?
When is a referral to a registered dietitian recommended?
Example 1:
fruit parfait containing yogurt (175 g or ¾ cup) with chopped walnuts (30 mL or 2 Tbsp.) and
sliced banana (125 mL or ½ cup) will provide about 350 calories
Example 2:
salmon salad containing canned salmon (75 g or 2.5 oz) with mayonnaise (15 mL or 1 Tbsp.)
on whole grain crackers (6 crackers) and 2% milk (250 mL or 1 cup) and a pear (one medium)
will provide about 450 calories
Nutrition Guideline
Revised January 2024
Page 12
Pregnancy
What nutrients are important during pregnancy?
Pregnancy is a period of accretion of certain tissues including the uterus, breast or chest,
blood, extravascular fluids, and fat stores, as well as the development of the fetus and
placenta.
1
The recommendations for many nutrients are higher during pregnancy.
1
The following table summarizes key nutrients of special concern during pregnancy. These
nutrients include calcium, vitamin D, iron, vitamin A, vitamin B
12
, folate, omega-3 fatty acids,
choline, iodine, and fibre.
Table 2. Nutrient Amounts Recommended for Pregnancy from All Sources
(food, multivitamin supplement, single-source supplement)
Nutrient
Recommended Amount Per Day
for Adult Pregnancy (19–50 years)
Upper Limit (UL)
Calcium
1000 mg
a
Total daily intake not to exceed 2500 mg
a
Choline
450 mg
a
Total daily intake not to exceed 3.5 g
a
Folate/Folic Acid
0.6 mg (600 mcg) with 0.4 mg (400
mcg) to come from a supplement
a
1 mg (1000 mcg
a
)
The UL for folate applies only to synthetic
forms obtained from supplements, fortified
foods, or a combination of these
a
Iodine
0.22 mg (220 mcg)
a
Total daily intake not to exceed 1.1 mg
(1100 mcg)
a
Iron
27 mg
a
Total daily intake not to exceed 45 mg
b
Omega-3 Fatty
Acids (DHA and
EPA)
Include at least 150 g (5 oz) cooked
fish rich in omega-3 fatty acids and
low in mercury each week during
pregnancy
c
Safe UL not defined
c
Vitamin A
770 mcg
a
(2567 IU)
3000 mcg/day (10,000 IU/day). UL is for
preformed vitamin A only
a
Vitamin B
12
2.6 mcg
a
Safe UL not defined
a
Vitamin D
600 IU
b
Total daily intake not to exceed 4000 IU
b
Sources:
a
Health Canada, 2010. Dietary Reference Intake Tables
34
b
IOM 2010
35
c
Health Canada, 2009. Prenatal Nutrition Guidelines for Health Professionals: Fish and Omega-3 Fatty Acids
36
Consider recommending individual consultation with an RD if there is concern about adequate
nutrient intake during pregnancy.
See also:
When is a referral to a registered dietitian recommended?

Nutrition Guideline
Revised January 2024
Page 13
Pregnancy
Folate (Folic Acid)
Folate is a B vitamin essential for the development of the spine, brain, and skull of the fetus
during the first four weeks of pregnancy.
37
Adequate folate has been shown to reduce the
risk of neural tube defects (NTD).
38,39
Folic acid, folacin, and folate are all forms of the same
B vitamin. Folate refers to what is naturally found in foods. Folic acid refers to supplements
and fortified sources.
21
Due to the high prevalence of unintended pregnancies, folic acid supplementation is
recommended for all people who could become pregnant. The benefits of folic acid are
highest in the very early weeks of pregnancy when people often do not know they are
pregnant.
37,39,40
People of reproductive age who could become pregnant are recommended to
consume folate-rich foods and take a multivitamin supplement that provides 0.4 mg
(400 mcg) folic acid in it every day.
People who are considering or planning for pregnancy and not taking a multivitamin
supplement containing folic acid are recommended to take a multivitamin supplement with
0.4 mg (400 mcg) folic acid in it every day, starting at least three months before
conception.
1,37,40
Folic acid supplementation is recommended throughout pregnancy, as part
of a multivitamin supplement that contains iron, vitamin D, and vitamin B
12
.
1
More than 1 mg (1000 mcg) folic acid/day or more than one daily dose of a multivitamin
supplement is not recommended for individuals at low risk of NTDs.
1
See also:
When Higher Folic Acid Supplementation may be Recommended

Nutrition Guideline
Revised January 2024
Page 14
Pregnancy
Table 3. Food Sources of Folate (Folic Acid)
Very high source
(greater than or equal to
55 mcg/serving)
High source
(greater than 33 mcg/serving)
Source
(greater than 11 mcg/serving)
Vegetables and Fruits
Asparagus
Avocado
Beets
Broccoli (cooked)
Brussels sprouts
Collards
Endive
French beans
Green snap peas
Papaya
Romaine lettuce
Seaweed
Spinach
Grains
Enriched pasta
Wheat germ
Protein Foods
Black beans
Chickpeas
Kidney beans
Lentils
Navy beans
Pinto beans
Peanuts
Soybeans
Sunflower seeds
White beans
Vegetables and Fruits
Canned beets
Bok choy
Butterhead lettuce
Green peas
Okra
Oranges
Orange juice
Parsnips
Grains
Enriched bread (look for 15% DV
for folate)
Enriched cereal
Enriched crackers
Protein Foods
Eggs
Fortified white flour
Vegetables and Fruits
Arugula
Bananas
Broccoli (raw)
Cabbage
Carrots
Cauliflower
Dandelion greens (raw)
Kale (raw)
Leeks
Lettuce (iceberg, loose-leaf,
radicchio, red leaf)
Pineapple
Potatoes
Rutabaga
Snap beans
Snow peas
Strawberries
Tomatoes
Grains
Wild rice
Protein foods
Cottage cheese
Lima beans
Milk
Tofu
Pistachio nuts
Sesame seeds
Walnut
Yogurt
Source: Health Canada. Canadian Nutrient File, Version 2015
41
nutrient claims using the 2016 Daily Values
42
and 2007
CFG serving sizes
43

Nutrition Guideline
Revised January 2024
Page 15
Pregnancy
All people who could become pregnant are advised:
• to choose folate-rich food choices
• to take a multivitamin supplement with 0.4 mg (400 mcg) folic acid in it
All individuals who are considering or planning a pregnancy are advised:
• to choose folate-rich food choices
• to take a multivitamin supplement with 0.4 mg (400 mcg) folic acid in it starting at least
two to three months before conception
• to talk to their care provider about the amount of folic acid that is right for them before
they start trying to become pregnant as some individuals may need more
All individuals who are pregnant and at low risk of NTDs are advised to:
• choose folate-rich food choices
• take a multivitamin supplement with 0.4 mg* (400 mcg) folic acid in it during their entire
pregnancy and for as long as lactation continues
* Note, some common prenatal vitamins contain more folic acid, advise individuals to choose a
product with a dosage close to 0.4 (400 mcg) folic acid and not more than 1.0 mg (1000 mcg)
folic acid.
When Higher Folic Acid Supplementation may be Recommended
Everyone is encouraged to talk to their care provider about the amount of folic acid that is
right for them before they start trying to become pregnant.
Individuals with a previous fetus or neonate with another folic acid-sensitive congenital
anomaly or those with other medical-surgical conditions associated with a risk of folate
deficiency require two separate periods of supplementation.
40
From preconception to 12
weeks gestation, the supplement dose recommended is 1 mg (1000 mcg) in a multivitamin
containing iron and vitamin B12.
40
After 12 weeks gestation, the folic acid dosage can return to
the low-dosage regime of 0.4 mg (400 mcg) folic acid in a multivitamin supplement.
40
Folic acid-sensitive anomalies can include but are not limited to:
40
• congenital heart defects
• oral facial clefts
• limb-reduction defects
• urinary-tract defects

Nutrition Guideline
Revised January 2024
Page 16
Pregnancy
Medical-surgical conditions include but are not limited to:
40
• pre-gestational diabetes (type 1 or 2)
• gastrointestinal conditions such as inflammatory bowel disease, Crohn's disease, celiac
disease, surgical gastric bypass, advanced liver disease
• use of medications with anti-folate physiological effects (methotrexate, phenytoin,
carbamazepine, valproate, sulfasalazine) alcohol use disorder
Individuals who have a high risk of a pregnancy affected by NTD need to discuss with their
physician the adequate dosage of folic acid as they may require doses of folic acid higher
than 1.0 mg (1000 mcg) before and during their first trimester.
40
This may include those with a
larger body size pre-conceptionally (BMI greater than 30 kg/m
2
).
At high risk for NTDs include individuals with a:
40
• previous pregnancy affected with an NTD
• personal or reproductive partner family history of NTD (had an NTD themselves)
• first-degree relative with an NTD
Individuals with a higher risk of a pregnancy affected by NTDs are advised:
• to choose folate-rich food choices such as ready-to-eat cereals, enriched breads and
pasta, dark green vegetables (peas, spinach, Brussels sprouts, and broccoli), beans and
lentils, and citrus fruits (oranges)
• to discuss with their physician about the adequate dosage of folic acid supplementation if
they have additional health risks or have a higher risk of a pregnancy affected by NTD
Calcium and Vitamin D
Calcium is a mineral that has a key role as a structural component of bones and teeth. It is
also important for muscle function, nerve activity, and hormone secretion.
35
Vitamin D is a fat-
soluble vitamin that has important roles in many body functions, including facilitating
intestinal absorption of calcium and supporting the delivery and utilization of calcium in bone
and teeth formation and nerve and muscle activity.
35
In people who are pregnant, calcium, and
vitamin D are also needed for the growth and development of the skeletal tissue of the
fetus.
44
During pregnancy, intestinal absorption of calcium is increased and bone calcium
mobilization is optimized.
9,44
Due to physiological changes occurring during pregnancy, requirements for calcium and
vitamin D remain the same as for individuals
α
who are not pregnant.
44
Adults need a total of
1000 mg calcium and 600 IU vitamin D daily to meet their requirements during pregnancy
(See Table 2
).
35
Evidence of calcium and vitamin D supplementation above these levels during
pregnancy to improve parental and neonatal outcomes has been inconclusive.
38,39,44

Nutrition Guideline
Revised January 2024
Page 17
Pregnancy
Calcium
Adequate calcium intake during pregnancy can be achieved by eating a variety of foods as
recommended by Canada’s food guide, including calcium-rich foods. Dairy foods, including
cow’s milk, yogurt, and cheese are some of the best food sources of calcium.
41
Some calcium
is provided in most multivitamin supplements.
Table 4. Food Sources of Calcium
About 300 mg or more
About 200 mg
About 100 mg
About 50 mg
• Cow’s milk, fluid (e.g.
skim, 1%, 2%, lactose-
free), 1 cup (250 mL)
• Cow’s milk, powder,
24 g, amount to make
250 mL
• Fortified plant-based
beverage
(e.g. fortified soy
beverage),
1 cup (250 mL)
• Blackstrap
molasses,
1 Tbsp (20 g)
• Cheese, hard
(e.g. cheddar,
Colby, Swiss),
1 oz (30 g)
• Cheese, Parmesan
(hard, shredded,
grated),
½ oz (15 g)
• Kefir,
¾ cup (188 mL)
• Sardines, canned
with bones,
2 oz (55 g)
• Soup made with
cow’s milk,
1 cup (250 mL)
• Tofu, made with
calcium,
⅔ cup (85 g)
• Yogurt,
½ cup (115 g)
• Almonds, shelled,
3 Tbsp (50 g)
• Brazil nuts, shelled,
3 Tbsp (50 g)
• Cottage cheese,
½ cup (125 g)
• Milk pudding,
½ cup (130 g)
• Salmon, canned
with bones,
2 oz (55 g)
• Soybeans,
½ cup (125 mL)
• White beans,
½ cup (125 mL)
• Almond butter,
1 Tbsp (15 g)
• Navy beans,
cooked,
½ cup (125 mL)
• Sesame butter
(tahini),
1 Tbsp (15 g)
Source:
Health Canada. Canadian Nutrient File, Version 2015
41
using Health Canada’s Nutrition Labelling – Table of
Reference Amounts for
45

Nutrition Guideline
Revised January 2024
Page 18
Pregnancy
People who do not consume milk, yogurt, cheese, or calcium-fortified plant-based beverages,
such as fortified soy beverages, are at risk of not meeting calcium requirements; an additional
calcium supplement may be required. Individuals
α
who are taking single-dose calcium
supplements are advised to take them in amounts that do not exceed 500 mg at a time.
1,9,46,47
Calcium supplements are best taken separately from multivitamin supplements containing
iron (at least 2 hours between) due to the potential of calcium and iron competing for
absorption.
48
Single nutrient supplementation is best advised by an RD, who will base
recommendations on individual client assessments. Calcium intake from food, supplements,
and medication (calcium-based antacids) is not to exceed the upper limit (UL) of
2500 mg/day.
47
α
Language in the original articles
See also:
What are the food safety concerns with cheese and what are safe cheese choices?
What are plant-based beverages and are they a nutritious choice during pregnancy?
Vitamin D
Vitamin D occurs naturally in very few foods (e.g., fatty fish and egg yolks).
35
Most foods that
are a source of vitamin D have been fortified. This includes cow’s milk, fortified goat’s milk,
fortified plant-based beverages, and margarine.
49
Health Canada is undertaking several
actions to increase the amount of vitamin D in the food supply. This includes approximately
doubling the mandatory amount of vitamin D in cow’s milk and margarine.
49
Fortification of
goat’s milk remains voluntary, but if fortified, the amount of vitamin D is mandated to match
the levels in cow’s milk.
50
Currently, there are no regulations that require plant-based
beverages to be fortified. If manufacturers choose to meet the specified conditions to fortify
their plant-based beverage product, they are permitted to match the level of vitamin D in
cow’s milk.
21
During the vitamin D fortification strategy transition period from December 2022
until December 31, 2025, manufacturers may fortify at either pre-strategy (original) or
strategy (new) levels (See Table 5
).
50
During pregnancy, food sources of vitamin D are recommended in addition to a daily
multivitamin dose of at least 400 IU (10 mcg) vitamin D to meet the recommended daily
amount of 600 IU.
35
The UL for vitamin D intake from food and supplement sources is
4000 IU/day.
35

Nutrition Guideline
Revised January 2024
Page 19
Pregnancy
Table 5. Food Sources of Vitamin D
About 200 IU
(5 mcg) or more
About 100 IU (2 ½ mcg)
About 50 IU (1 ¼ mcg)
• Fish, 3 ½ oz (100 g) cooked
o Herring
o Rainbow trout
o Salmon (farmed and
wild)
• Fish, 3 ½ oz (100 g) cooked
o Atlantic mackerel
o Hake
• Eggs, around 2 large (100 g)
• Fish, canned, 2 oz (55 g)
o Anchovies
o Sardines
• Yogurt, if fortified with
vitamin D, 1/2 cup (115 g)
• Milk, 1 cup (250 mL)
o Cow’s milk, all forms* and all types**
o Goat’s milk, if fortified with vitamin D, all forms* and all
types**
* forms – liquid, powdered, evaporated
** types – skim, 1%, 2%, 3.25% (homogenized), lactose-free
• Fortified plant-based beverages (e.g. fortified soy beverage),
1 cup (250 mL)
Margarine, 2 tsp (10 g)
Vitamin D Fortification Strategy Transition Period:
• During the transition period (until 2026), cow’s milk, fortified goat’s milk, and fortified plant-based beverages
will contain 100–200 IU per 1 cup (250 mL), and margarine will contain 50–100 IU per 2 tsp (10 g).
49,50
• To be fortified with vitamin D levels that match cow’s milk, plant-based beverages must meet specified
requirements for protein and fat.
21
• The fortification strategy indicates an intention to permit the direct addition of vitamin D to yogurt.
50,51
Vitamin
D in yogurt is currently only via the optional use of fortified milk in the production of yogurt.
Source: Health Canada. Canadian Nutrient File, Version 2015
41
and Government of Canada, Canada Gazette, Part II,
Vol 156, No.15
50
using Health Canada’s Nutrition Labelling – Table of Reference Amounts for Food
45
In summary, the IOM recommends adults who are pregnant (19–50 years of age) obtain the
following daily amounts of calcium and vitamin D from all sources (food and supplements):
35
• 1000 mg/day calcium
• 600 IU/day vitamin D
To help meet calcium and vitamin D requirements, all adults who are pregnant are advised to:
• consume food sources of calcium and vitamin D
• consume around 2 cups (500 mL) milk or a fortified plant-based beverage each day
• take a multivitamin supplement each day that contains at least 400 IU vitamin D

Nutrition Guideline
Revised January 2024
Page 20
Pregnancy
Individuals May Be At Risk For Inadequate Intake or Have Higher Requirements for
Calcium and Vitamin D
Individuals following vegan diets, with highly pigmented skin, who have limited sun exposure,
or those who live in northern latitudes are at higher risk of vitamin D deficiency.
1,9,38,39
In
addition, individuals with obesity, inflammatory disease, or who have undergone gastric
bypass surgery, may have impaired absorption and screening for vitamin D deficiency may be
necessary.
1
People, including both adolescents and adults, who have undergone gastric
bypass surgery have higher calcium requirements during pregnancy.
1
See also:
What are the nutrients of concern for pregnancy during adolescence?
Iron
Iron is a mineral that has many roles in the body, including functioning as a component of
several proteins, notably hemoglobin.
52
Low hemoglobin levels in pregnancy are associated
with increased risks of preterm birth,
53
low birth weight,
53,54
and small for gestational age
infants.
53
Additional iron is needed during pregnancy to increase the maternal red blood cell
mass and to supply the growing fetus and placenta.
55
The recommended daily allowance (RDA) for iron during pregnancy is 27 mg/day, an increase
of 9 mg/day over requirements for individuals
α
aged 19–50 who are not pregnant.
52
The UL for
iron is 45 mg/day.
48
Individuals who are being treated for iron-deficiency anemia during
pregnancy may be treated with higher doses of iron above the UL.
1
During pregnancy, individuals are advised to meet recommended iron requirements by
choosing iron-rich foods from Canada’s food guide and taking a multivitamin supplement
containing iron every day.
55
Health Canada dosage recommendation for iron supplementation
is 16-20 mg per day in a daily multivitamin supplement. Many common multivitamin
supplements available for pregnancy contain up to 27 mg iron. These doses are considered
safe during pregnancy. Practical guidance is to advise clients to look for a multivitamin that
contains between 16–27 mg iron/dose.
If single-dose calcium supplements are being used, these are best taken separately from
multivitamin supplements containing iron (at least two hours between) due to the potential of
calcium and iron competing for absorption.
48
Multivitamin supplements containing iron are
usually a once-daily dose. It is advised to take them as recommended on the product package.

Nutrition Guideline
Revised January 2024
Page 21
Pregnancy
Dietary iron is found in foods in both heme iron and non-heme iron forms. Heme iron is better
absorbed than non-heme iron.
55
Only meat (beef, pork, lamb, elk, deer, etc.), poultry (chicken,
turkey), fish, and seafood contain heme iron. Non-heme iron is found in meat, poultry, and fish,
as well as in eggs and plant-based foods such as tofu (medium or firm), legumes (such as
kidney beans, lentils, and chickpeas), nuts and seeds, and grains products. Some food
products, including ready-to-eat cold cereal, are enriched with iron.
Table 6. Food Sources of Iron
Very high source
(greater than or equal to
3.5 mg/serving)
High source
(greater than or equal to
2.1 mg/serving)
Source
(greater than or equal to
0.7 mg/serving)
Grains
Cold cereal, enriched
Instant hot cereal, enriched,
cooked
Protein Foods
Chickpeas
Lentils
Liver
Moose
Mussels or Oysters
Pumpkin seeds
Wild duck
Other Foods
Blackstrap molasses
Protein Foods
Beef
Clams
Elk
Kidney beans
Soybeans
Tofu
Venison
Grains
Pasta, enriched
Oatmeal
Protein Foods
Almond, cashew, peanut butter
Canned light tuna
Chicken
Eggs
Lamb
Pork
Sardines
Source: Health Canada. Canadian Nutrient File, Version 2015
41
nutrient claims using the 2016 Daily Values
42
and
2007 CFG serving sizes
43
* May also include almond, cashew or rice – if fortified
The absorption of non-heme iron from foods is improved when foods rich in vitamin C are
consumed at the same time.
48
In addition, absorption of non-heme iron from food high in
phytates (e.g. soybeans, black beans, lentils, split peas) improves when these foods are
soaked overnight in water or sprouted.
56
Table 7. Food Sources of Vitamin C
Food Sources of Vitamin C
• Broccoli
• Cantaloupe
• Grapefruit
• Kiwi
• Mango
• Oranges
• Potatoes
• Strawberries
• Sweet peppers
• Tomatoes
Source: Health Canada. Canadian Nutrient File, Version 2015.
41
Nutrition Guideline
Revised January 2024
Page 22
Pregnancy
All individuals who are pregnant are advised to:
• follow Canada’s food guide
• consume foods rich in both heme and non-heme iron
• consume foods rich in non-heme iron together with foods with vitamin C
• consider the iron daily dose when choosing a multivitamin supplement; look for one that
provides 16–27 mg of iron/daily.
Consider recommending individual consultation with an RD if there is concern about iron
intake from food choices.
See also:
What resources are available for the public?
Individuals Who May Require Higher Doses Of Supplemental Iron
People who have an increased risk of iron deficiency during pregnancy need to discuss with
their doctor the adequate dosage of supplemental iron as they may require doses of iron
higher than the amounts found in a multivitamin supplement or prenatal vitamin. Therapeutic
doses of iron may be required for people demonstrating biochemical evidence of iron deficiency
(low hemoglobin levels; low serum ferritin levels).
1
Individualization of treatment with a
physician is recommended for people who require therapeutic doses of iron. Treatment
typically includes decisions regarding the type (e.g. liquid, pill), mode of administration (e.g.
oral, intravenous), and formulation (e.g. sulphate, fumarate or gluconate) of iron.
57
Individuals at higher risk for iron deficiency during pregnancy include adolescents and
refugees or immigrants from low-income countries, as well as people with:
1
• low or no intake of meat (beef, pork, wild game), fish, and poultry
• significant blood loss due to menstruation before pregnancy
• low socioeconomic status
Review recommendations for fluid and fibre intakes for individuals taking therapeutic doses
of supplemental iron to minimize risks of constipation.
9
People with a higher risk of iron deficiency during pregnancy are advised to:
• choose iron-rich food choices from Canada’s food guide
• discuss the adequate dosage of iron supplementation with their physician
See also:
When is a referral to a registered dietitian recommended?
What are the nutrients of concern for pregnancy during adolescence?
Constipation – what can be done during pregnancy?

Nutrition Guideline
Revised January 2024
Page 23
Pregnancy
Omega-3 Fatty Acids
Omega-3 fatty acids are polyunsaturated fatty acids. Scientific research has focused on the
association between higher intakes of these nutrients and several health outcomes. Current
research is investigating the relationship between DHA intake during pregnancy and early
infancy and the early neurodevelopment of the infant.
58,59
Omega-3 fatty acids include:
• alpha-linolenic acid (ALA)
• eicosapentaenoic acid (EPA)
• docosahexaenoic acid (DHA)
EPA and DHA are primarily found in fish, shellfish, fish oil supplements, and omega-3-
enriched eggs.
60
ALA is found in plant sources such as walnuts, flaxseed, canola, and soybean
oils.
60
ALA is converted to EPA and DHA in humans, but the amount of ALA converted is very
low.
1,60
The majority of the documented health benefits of omega-3 fatty acids are from
research conducted on EPA and DHA rather than from plant-derived ALA.
60,61
The IOM has not set a recommendation for DHA or EPA intake.
61
Dietitians of Canada and the
Academy of Nutrition and Dietetics recommend 500 mg/day of DHA and EPA for healthy
individuals.
62
DHA is difficult to get from foods other than fish or DHA-supplemented food.
1
People who are pregnant are advised to choose fish that are high in EPA and DHA and low in
mercury.
36
These fish include herring, Atlantic hake, salmon, sardines, and rainbow trout.
36
Table 8. Low Mercury Food Sources of Omega-3 Fatty Acids
High Source
DHA and EPA
ALA
Sources:
a
Health Canada. Canadian
Nutrient File, Version 2015.
41
b
Burnbrae Farms
63,64
Note: Farmed and wild fish
may have different amounts
of DHA/EPA.
Ground flaxseeds
Herring
Mackerel, Atlantic
Rainbow Trout
Salmon, Atlantic
Walnuts
Source
DHA and EPA
ALA
Canola oil
a
Clams
Naturegg
™
Omega-3–1 large egg (53 g)
b
Naturegg
™
Omega Plus™–¼ cup (63 g)
b
Sardines
Shrimp
Tuna, light

Nutrition Guideline
Revised January 2024
Page 24
Pregnancy
All people who are pregnant are advised to:
• consume cooked fish rich in omega-3 fatty acids and low in mercury
• aim to include at least 150 g (5 oz) fish weekly
See also:
Is it safe to consume fish during pregnancy?
What advice can be given about omega-3 fatty acid supplements during pregnancy?
Other Food-related Safety Considerations: Flaxseed and Flaxseed Supplements
Choline
Choline is a nutrient involved in functions essential to fetal brain development and tissue
expansion.
1
Choline availability during embryogenesis and perinatal development may be
especially important.
65
Recent research is also exploring a potential relationship between low
serum choline levels during pregnancy and NTD risk.
66
Choline needs in pregnancy are believed to be greater than choline requirements during the
non-pregnant state.
65
Individuals
α
who are pregnant are recommended to obtain 450 mg/day
choline, an increase of 25 mg/day over the non-pregnant state to cover the amount needed
for the fetus and placenta.
65
UL values for choline are set at 3.5 g/day for individuals
α
19 years
and older who are pregnant, and 3.0 g/day for those 18 years and under who are pregnant.
The UL refers to total choline intakes from food, fortified food, and nutrient supplements.
65
Choline is found in both plant and animal food sources with the greatest concentrations in
eggs, beef, and milk. An Alberta study with individuals
α
who were pregnant found that those
who reported regular egg and milk consumption were more likely to meet choline intake
recommendations.
67
Choline may or may not be included in multivitamin supplements,
including those marketed for pregnancy in Canada.
68
Healthcare providers can promote
regular consumption of choline-rich foods.
40
Table 9. Food Sources of Choline
Protein Foods
Vegetables and Fruits
Source: Health Canada.
Canadian Nutrient File, Version
2015.
41
Beef
Chicken
Cow’s milk
Eggs
Fortified soy beverage
Kidney beans
Navy Beans
Pork
Salmon
Broccoli
Brussels sprouts
Cauliflower
Salad greens
(such as endive and romaine lettuce)
Spinach
Grains
Wheat germ

Nutrition Guideline
Revised January 2024
Page 25
Pregnancy
All individuals who are pregnant are advised to:
• follow Canada’s food guide; it describes a healthy eating pattern that includes dietary
choline and will guide them in meeting their needs for other nutrients
• regularly consume foods rich in choline, such as wheat germ, eggs, salmon, beef, chicken,
navy or kidney beans, and cow’s milk
Consider recommending individual consultation with an RD if there is concern about choline
intake from food choices.
See also:
When is a referral to a registered dietitian recommended?
Iodine
Iodine is a mineral that is an essential component of the thyroid hormones thyroxine (T4) and
triiodothyronine (T3), which are involved in the regulation of various enzymes and metabolic
processes, particularly protein synthesis
52
and required for proper skeletal and central
nervous system development.
9
Iodine deficiency can lead to goiter, stunted physical and
intellectual development, spontaneous abortion, and stillbirth.
69
Iodine requirements during pregnancy increase from 150 mcg/day before conception to 220
mcg/day during pregnancy.
52
The UL for iodine is 1100 mcg/day.
52
Although iodine deficiency is
a major public health concern in many countries, including the United States, Australia, and
New Zealand,
1,38
Canada’s mandatory iodization of salt in 1949 has resulted in adequate intake
levels of iodine for most Canadians.
69
The most recent information for the Canadian population,
based on 2009–2011 urinary iodine concentration, indicates iodine intake adequacy.
69
Food production and consumption patterns attributed to mild or moderate deficiencies in
iodine intake include the use of non-iodized salt, such as sea salt, reduction of salt in the diet,
and reduction of iodine supplementation in commercial dairy products.
69
Examples of dietary
sources of iodine include iodized salt, seafood, eggs, milk, and grain products. Analysis of
dietary consumption data in the United States indicates that dairy product consumption was
an important contributor to iodine status among all individuals (pregnant and non-pregnant).
70
Currently available multivitamin supplements marketed for pregnancy in Canada contain
iodine in sufficient amounts to meet needs during pregnancy.
1
All individuals who are pregnant are advised:
• to consume a varied diet as recommended by Canada’s food guide, including cow’s milk
and other dairy products such as yogurt and cheese
• when choosing salt, choose an iodized salt
• when choosing a multivitamin supplement, choose one containing iodine

Nutrition Guideline
Revised January 2024
Page 26
Pregnancy
Vegetarian Eating Patterns during Pregnancy
Return to Key Questions
Are there any extra considerations for vegetarian eating patterns?
Well-planned vegetarian eating patterns are appropriate for all stages of the life cycle,
including pregnancy and lactation.
1,71
Vegetarian eating patterns support good nutrition status
and health. However, ensuring nutritional adequacy becomes more challenging when foods
are avoided and when nutrient needs are higher, such as during pregnancy.
Individuals may identify themselves as vegetarian, or primarily vegetarian, although they eat
some fish or chicken, milk or dairy products, eggs, or animal by-products. Lacto-ovo
vegetarians avoid all animal flesh but eat eggs (ovo) and dairy products (lacto). Vegans
generally avoid all foods of animal origin.
71
To optimize nutrition, care providers are advised to:
• identify the type of vegetarian diet followed (e.g. lacto-ovo, vegan).
71
• encourage individuals following a vegetarian eating pattern to plan their diet well, by
including a variety of protein choices offered in Canada's food guide.
• advise individuals who are following a vegan eating pattern to ensure their multivitamin
supplement contains 2.6 mcg vitamin B
12
to meet the RDA during pregnancy.
72
• refer individuals following a vegan eating pattern who are pregnant or planning a
pregnancy to an RD for nutrition assessment and counselling.
Energy
The energy recommendations for individuals who are pregnant following a vegetarian eating
pattern do not differ from those following a non-vegetarian eating pattern.
73
Iron
Individuals who are pregnant and are following a vegetarian eating pattern are at higher risk
for iron deficiency.
48
Screening, by measuring hemoglobin and serum ferritin by their primary
care provider, is recommended.
1
Well-chosen vegetarian diets can provide adequate iron;
however, the iron needs of vegetarians are 1.8 times higher than non-vegetarians due to the
reduced bioavailability of vegetarian sources of iron.
1
Individuals following vegetarian diets
while pregnant are recommended to choose a multivitamin supplement with at least 27 mg
iron, an amount commonly found in prenatal branded supplements.
1,71
Additional iron
supplements may be needed to prevent or treat iron-deficiency anemia.
1,71

Nutrition Guideline
Revised January 2024
Page 27
Pregnancy
Calcium and Vitamin D
Individuals following a vegan eating pattern face the greatest risk of inadequate calcium
intake and are advised to include a wide variety of non-dairy sources of calcium in their diet.
71
Calcium requirements can be met by including around 2 cups (500 mL) fortified plant-based
beverages and by eating a variety of other calcium-containing foods such as calcium-set tofu
and leafy green vegetables.
1,71
The need for calcium supplementation can be assessed by an
RD.
71
Nutrition Services, Alberta Health Services recommends all individuals who are pregnant
ensure their multivitamin supplement contains at least 400 IU vitamin D. A higher dose
supplement may be needed for those individuals at risk for vitamin D deficiency.
74
Vitamin B
12
Individuals following a vegan eating pattern are at high risk of inadequate intake of vitamin B
12
,
a micronutrient which is only available from animal sources.
71,72
Those who exclude all animal
products from their diet will require vitamin B
12
from a combination of supplements, fortified
food, or a reliable plant source modified to contain a bio-available source of vitamin B
12
to meet
the daily requirement of 2.6 mcg. Individuals who are pregnant and following a vegan diet are
recommended to choose a multivitamin supplement containing at least the daily requirement
of 2.6 mcg vitamin B
12
.
40
Examples of dietary sources of vitamin B
12
appropriate for a vegan diet
include fortified plant-based beverages and fortified meat analogues such as ‘veggie
burgers’.
72
Zinc
In general, zinc status among individuals following a vegetarian eating pattern is adequate,
although lower than the zinc status of non-vegetarians.
71
However, as with iron, a high intake
of phytates may interfere with absorption and are potentially detrimental to zinc status.
71
Individuals following a vegetarian eating pattern are advised to consume zinc-rich foods such
as nuts, legumes, cheese, soy, whole grains, milk, and egg yolk often.
Omega-3 Fatty Acids
Individuals following a vegetarian eating pattern who avoid fish may not be consuming
adequate DHA. Vegetarians can consume ALA from plant sources that are converted into
DHA in the body; however, this process is inefficient. Vegetarians may have higher
requirements for ALA and are encouraged to consume foods rich in ALA such as walnuts,
canola oil, and soybean-based foods such as tofu and edamame.
71,75
In addition to ALA,
individuals following a vegetarian eating pattern are advised to choose food sources of DHA
that are appropriate for them, such as fortified foods, omega-3 eggs, and seaweed, or use a
microalgae-derived DHA supplement.
71
Nutrition Guideline
Revised January 2024
Page 28
Pregnancy
Other Nutrients of Concern
Choline and iodine may be low in the diets of individuals following a vegetarian eating pattern,
particularly a vegan diet.
1,71
During pregnancy encourage individuals to consume sources of
choline and iodine that are appropriate for them, such as eggs, dairy products, and sea
vegetables. Choosing iodized salt over sea salt or other non-iodized varieties will also
contribute to iodine requirements.
71
See also:
When is a referral to a registered dietitian recommended?
For related Nutrition Guidelines see Nutrition Guideline: Vegetarian Eating
Nutrient Supplements During Pregnancy Return to Key Questions
Consider recommending individual consultation with an RD if there is concern about
supplement intakes during pregnancy. Individuals are advised to look for a Natural Product
Number (NPN) when choosing a supplement.
36
See also:
When is a referral to a registered dietitian recommended?
What are the recommendations for a multivitamin supplement for
pregnancy?
A multivitamin is recommended to provide folic acid, iron, vitamin B
12
, and vitamin D every day.
1
Initiation of folic acid supplementation is recommended at least three months before
pregnancy to ensure adequate folic acid intake. Supplementation is recommended to
continue throughout pregnancy and after birth, throughout the reproductive years.
37
Note
that some commonly available multivitamin supplements (e.g. adult gummy multivitamins)
may not contain adequate amounts of nutrients important for pregnancy, such as iron. It is
recommended a multivitamin includes 2.6 mcg vitamin B
12
.
40
Available multivitamin
supplements that meet iron, vitamin D and folic acid recommendations have adequate B
12,
and
therefore, are not included in practical guidance information.
For individuals who have difficulty taking a multivitamin supplement, strategies that may help
include:
• Taking the supplement in the evening.
• Working with their physician or pharmacist who can recommend alternatives (e.g. smaller
pill size, different formulation).

Nutrition Guideline
Revised January 2024
Page 29
Pregnancy
Health Canada recommends taking a multivitamin with folic acid (0.4 mg), iron (16–20 mg),
vitamin D (400 IU) and vitamin B
12
every day. These exact amounts can be hard to find. When
assisting an individual who is pregnant in choosing a multivitamin, look for this information
on the label as these levels are safe:
• Iron: between 16–27 mg
• Vitamin D: at least 400 IU (10 mcg)
• Folic acid (folate): between 0.4–1 mg (400–1000 mcg)
• Vitamin B
12
: 2.6 mcg
What is the difference between a multivitamin and a prenatal vitamin?
‘Prenatal vitamins’ are multivitamin supplements marketed for people during pregnancy.
Typically, they contain higher doses of folic acid and iron. Some prenatal vitamins contain
0.8–1 mg (800–1000 mcg) folic acid. Individuals who are pregnant are recommended to not
consume more than 1 mg (1000 mcg) folic acid/day without a care provider’s advice. Iron
amounts of 27 mg are also common in prenatal vitamins. These amounts are considered safe
during pregnancy. Many common multivitamin brands contain adequate amounts of vitamins
and minerals to meet the increased needs of pregnancy, except for iron. Since the amounts of
various vitamins and minerals included in multivitamin brands and prenatal vitamins vary
across brands/types, individuals are encouraged to review supplement labels and discuss
amounts with their care provider.
Are there benefits of taking a multivitamin compared to single-nutrient
supplements?
Taking a multivitamin supplement containing iron and folic acid has been shown to reduce the
number of LBW
76–78
and SGA infants
77–79
compared to taking single iron supplements with or
without folic acid. A multivitamin supplement can support individuals, particularly those most
vulnerable to poor nutrient intakes, in meeting the higher nutrient needs of pregnancy.
33
In
addition to containing iron and folic acid, multivitamin supplements contain other nutrients
that can be difficult to get enough of from food alone such as zinc, magnesium, and vitamin
B
6
.
33
Individuals vulnerable to poor nutrient intakes include those with social, economic, or
geographic at-risk circumstances (e.g., those living in poverty),
1
as well as individuals
experiencing substance dependency, household food insecurity, anemia, strict vegetarian
(vegan) diet, or poor eating habits.
9

Nutrition Guideline
Revised January 2024
Page 30
Pregnancy
What if an individual who is pregnant requires higher amounts of iron or
folic acid?
Most multivitamin supplements will not provide adequate doses of iron or folic acid for
individuals identified as needing higher amounts. Additional single-dose supplementation may
be required for at-risk individuals during pregnancy.
See also:
People who may require higher folic acid supplementation
People who may require higher doses of supplemental iron
Other Nutrient Supplements Return to Key Questions
Is the use of Lucky Iron Fish
™
recommended to improve iron status during
pregnancy?
Most people without iron deficiency can meet their additional iron needs during pregnancy by
choosing a variety of iron-rich foods from Canada’s food guide and taking a multivitamin
supplement containing 16–27 mg iron. Lucky Iron Fish™ is not recommended as an alternative
to supplements for the prevention or treatment of iron deficiency in the Canadian pregnant
population.
There is insufficient evidence on the effectiveness of the Lucky Iron Fish™ in improving iron
status.
80–82
The studies were only conducted in low-income countries with a high prevalence
of anemia, therefore, the limited research may lack applicability to the Canadian population. If
a client chooses to use the Lucky Iron Fish™, advise them to use it according to the
manufacturer’s directions.
What advice can be given about omega-3 fatty acid supplements during
pregnancy?
Individuals are advised to consult a physician before taking an omega-3 fatty acid
supplement. Supplements are not considered equivalent to eating fish.
60,83
Evidence suggests
DHA and EPA supplements may increase gestation duration between 1–3 days in both low-
risk and high-risk pregnancies.
61,84
EPA and DHA may increase birth weight by approximately
45 g and 100 g in low-risk and high-risk pregnancies, respectively.
61,85,86
No benefits on
preeclampsia, reducing the risk of preterm delivery, or other neonatal outcomes such as the
reduced risk of intrauterine growth restriction (IUGR) have been found.
61,84–88

Nutrition Guideline
Revised January 2024
Page 31
Pregnancy
Fish Oil Supplements
Fish oil supplements vary in the levels of EPA and DHA they contain.
60
Doses of fish oil (EPA +
DHA) of less than 3 g/day can be safely used by most individuals.
89
However, fish liver oil
supplements (e.g. cod liver oil) contain high levels of vitamin A. Therefore, fish liver oil
supplements are not recommended for individuals who are pregnant, breastfeeding, or
chestfeeding.
36,61
Fish oil supplements are contraindicated for individuals with intra-uterine
bleeding and other bleeding disorders or those taking blood thinners.
61
People are advised to
look for an NPN when choosing a supplement.
36
Those who dislike the “fishy” taste of fish oil
supplements may be advised to store them in the freezer or look for an enteric-coated
supplement.
See also:
What is the concern with vitamin A supplements in pregnancy?
Algal Supplements
Supplements containing EPA and/or DHA made from algae are also available.
90
These would
be suitable for vegetarians and individuals who are allergic to fish.
Flaxseed and Flaxseed Supplements
Hypotheses exist that the mild estrogenic effects of flaxseed may have adverse effects on
pregnancies. However, there is insufficient reliable clinical evidence about the effects of
flaxseed on pregnancy outcomes.
91
There is some evidence from observational studies that
flaxseed oil is associated with an increased risk of preterm birth.
92
Because of the insufficient
evidence regarding the safety of flaxseed in pregnancy and potential negative outcomes,
91,92
it may be safest during pregnancy to consume flaxseed in the amounts commonly found in
foods or 1 Tbsp (15 mL)/day and to avoid flaxseed oil.
92
Krill Oil Supplements
Krill oil is currently not recommended as safe during pregnancy. More evidence is needed on
the safety and efficacy of krill oil supplements in order to recommend krill oil supplements in
pregnancy.
93

Nutrition Guideline
Revised January 2024
Page 32
Pregnancy
Are protein supplements required during pregnancy?
Protein supplements are not required during pregnancy. In the first half of pregnancy, protein
requirements (about 46 g/day) are the same as for the non-pregnant state.
73
Although
individuals who are pregnant need an additional 25 g/day protein in the second half of
pregnancy (about 71 g/day), they can continue to meet their protein needs by following a
healthy eating pattern and including a protein source at each meal and snack.
73
The
consumption of high protein supplements in pregnancy is not required and may contribute to a
diet unbalanced in protein and carbohydrate; limited evidence demonstrates a lack of
beneficial effects and possible risks to the fetus.
94
Soy protein supplements or isoflavone
supplements are not recommended during pregnancy as high intakes are mildly estrogenic
and potentially could adversely affect fetal development.
1,95
See also:
When is a referral to a registered dietitian recommended?
What is the concern with Vitamin A supplements in pregnancy?
Multivitamin supplements marketed for pregnancy may contain either preformed vitamin A or
beta-carotene or both forms of vitamin A. Beta-carotene is not associated with any adverse
effects during pregnancy.
52
Too much preformed vitamin A is associated with birth defects,
particularly during the first trimester.
96
The UL for vitamin A for adults is 3000 mcg/day
(10,000 IU/day) and is based on preformed vitamin A (retinyl esters and retinol).
52
The risk of exceeding the UL from a multivitamin supplement is minimal. Commonly used
terms for preformed vitamin A in the ingredient list include retinyl acetate, retinyl succinate, or
retinyl palmitate. People who are taking multiple supplements (e.g. multivitamin supplements,
single supplements, fish liver oil supplements, or nutrition supplement drinks) and foods high
in preformed vitamin A, especially the liver, may be at risk of exceeding the UL.
See also:
Other Food-Safety Related Considerations – Liver
What about the use of other supplements during pregnancy?
People are encouraged to inform their care provider about the supplements they are taking
and learn about the safety of their use during pregnancy. For example, advise those taking
probiotic supplements that limited evidence exists on the safety of their use during
pregnancy and it is best to avoid probiotic supplement use.
See also:
Other Food-related Safety Considerations - Probiotic-containing Foods

Nutrition Guideline
Revised January 2024
Page 33
Pregnancy
Beverage and Fluid Intake during Pregnancy
Return to Key Questions
How much fluid is needed during pregnancy?
Adequate hydration is essential as a person accumulates 6–9 L of water during gestation.
9
During pregnancy, people are recommended to consume about 10 cups (~2.5 L) fluids/day for
adequate hydration.
9
One cup is equivalent to 250 mL (8 oz). This total amount of fluids
includes all beverages, including drinking water.
9
Note that sugar-sweetened beverages such
as iced tea, fruit juice, sports drinks, specialty coffees and teas, flavoured waters with added
sugars, and fruit-flavoured drinks like fruit punch, add little nutritional value. Water is
recommended as the main source of fluids.
Individuals who are pregnant are advised:
• to drink water throughout the day
• that healthy drink options other than water include milk and fortified plant-based
beverages
• to consume 10 cups (~2.5 L) fluids/day and possibly more if they are experiencing
constipation
• that if they are experiencing nausea and vomiting during pregnancy, additional actions
may be needed to prevent dehydration
Advise people who are pregnant and are experiencing signs of dehydration to contact their
physician or Health Link at 811.
See also:
Constipation – what can be done during pregnancy?
Nausea and vomiting – what can be done during pregnancy?

Nutrition Guideline
Revised January 2024
Page 34
Pregnancy
What are plant-based beverages and are they a nutritious choice during
pregnancy?
Plant-based beverages include soy, almond, coconut, cashew, oat, and other beverages
derived from legumes, nuts, seeds, or grains.
21
Plant-based beverages do not contain many of
the vitamins and minerals that are naturally present in cow’s milk such as vitamin B
12
,
riboflavin, and zinc.
97
Currently, there are no mandatory regulations that plant-based
beverages must be fortified.
21
If fortified, these beverages are required to be fortified with
vitamin A, vitamin D, vitamin B
12
, riboflavin, calcium, and zinc.
21
Individuals who are pregnant and choose to drink plant-based beverages are advised to:
• consume around 2 cups (500 mL) fortified plant-based beverages each day
• choose a fortified plant-based beverage that, per 1 cup (250 mL):
o provides at least 6 g of protein
21
o provides at least 23% daily value of calcium; and
o provides at least 10% daily value of vitamin D
Individualized assessment and counselling by an RD may be considered.
See also:
What nutrients are important during pregnancy: calcium and vitamin D
When is a referral to a registered dietitian recommended?
What is considered a safe intake of caffeine during pregnancy?
Health Canada’s recommendation for safe intake of caffeine in pregnancy is to limit
consumption to 300 mg or less/day.
98,99
Evidence suggests a dose-response association
between caffeine intake during pregnancy and an increased risk of adverse birth outcomes,
including low birth weight,
100,101
spontaneous abortion, stillbirth, and small-for-gestational-
age.
101
However, evidence of causal effects of caffeine intake on birth outcomes during
preconception and pregnancy is lacking and inconclusive.
102

Nutrition Guideline
Revised January 2024
Page 35
Pregnancy
Table 10. Beverage and Food Sources of Caffeine
Beverages with between
100–200 mg/1 cup (250 mL) serving
Beverages and foods with
less than 100 mg/1 cup (250 mL)
(or standard serving size)
Coffee, brewed
Coffee, roasted and ground, filter drip
Coffee, roasted and ground, percolated
Baking chocolate (unsweetened) (28 g)
Candy chocolate (milk, sweet) (28 g)
Chocolate milk
Coffee, espresso (30 mL single shot)
Coffee, instant
Coffee, instant, decaffeinated
Coffee, roasted and ground, decaffeinated
Cola beverage, regular (355 mL can)
Cola beverage, diet (355 mL can)
Hot cocoa mix (prepared)
Iced tea
Tea, regular (average blend, leaf, or bag)
Sources: Health Canada. Canadian Nutrient File, Version 2015; Health Canada, Caffeine in Food
41,98
Note: caffeine content of coffee and tea can vary depending on the plant variety and growing conditions, brewing
method and time, the proportion of coffee or tea to water, roasting method, particle size (‘grind’) and serving size.
Advise individuals who are pregnant:
• to limit caffeine intake to 300 mg/day, from all sources
• common sources of caffeine for most people are:
o Coffee: about 150 mg caffeine/250 mL (1 cup)
o Tea, green and black: about 30–50 mg caffeine/250 mL (1 cup)
o Cola beverages: about 23–40 mg caffeine/250 mL (1 cup)
o Chocolate: about 3–50 mg caffeine in 1 chocolate bar
See also:
What is the recommendation for caffeinated energy drinks during pregnancy?

Nutrition Guideline
Revised January 2024
Page 36
Pregnancy
What is the recommendation for caffeinated energy drinks during
pregnancy?
Individuals are advised to avoid all energy drinks during pregnancy. An energy drink is any
beverage that contains some form of legal stimulant and/or vitamin added to provide a short-
term boost in energy. These drinks may contain substantial and varying amounts of sugar and
caffeine as well as other substances including taurine, carnitine, inositol, ginkgo, and milk
thistle.
9
Many of these have not been studied for safety during pregnancy.
9,103
These drinks
provide a caffeine content similar to or exceeding the amount of caffeine in the same volume
of coffee: 75–85 mg in 1 cup (250 mL) and 70–240 mg in 1 can (473 mL).
104–108
See also:
What is considered a safe intake of caffeine during pregnancy?
Are sugary drinks recommended during pregnancy?
Sugary drinks or sugar-sweetened beverages include regular sodas, sports drinks, energy
drinks, fruit juice, fruit drinks, fruit punch, fruit cocktails, flavoured waters with added sugars,
iced tea, and specialty coffee and teas.
9,109,110
These drinks are similar in that they contain a
large amount of sugar and a low nutrient and high-calorie content. An additional concern with
sugary beverages is the possibility of their intake displacing nutrient-dense choices. It is
healthiest to limit or avoid these products.
109
What herbal teas are considered safe to consume during pregnancy?
Evidence is limited regarding the safety of herbal teas in pregnancy. The following herbs are
generally considered safe if limited to the amount commonly found in foods or consumed in
moderation as an herbal tea:
111
• orange peel
111
• bitter orange
111
• ginger root
112,113
• peppermint leaf
114,115
• rose hip
116
It is best to follow the preparation instructions on the label. General guidance is to limit intake
of teas made from these herbs to no more than 3 cups daily during pregnancy and to steep
the tea for a short period (e.g. 3–5 minutes).
Other herbal teas may be safe to consume during pregnancy; however, due to insufficient or
conflicting messaging of their safety during pregnancy, they are not listed in this guideline as
safe, e.g. red raspberry leaf, fennel, chamomile, lemon balm, red bush (rooibos), and valerian.

Nutrition Guideline
Revised January 2024
Page 37
Pregnancy
Since many teas are often a mixture of herbs, it is best to check the ingredient labels to make
sure all ingredients in the tea are safe.
111
Even ‘safe’ herbs are not recommended in pregnancy
if used in large or concentrated doses.
115,116
Advise individuals who are pregnant to check the
ingredients of all other beverages including chai and herbal teas marketed for pregnancy.
Chai is made by blending black tea with various spices, herbs, and steamed milk. As chai
products often contain multiple ingredients, the ingredients in the product need to be
carefully examined before use to ensure that all the ingredients are safe for consumption
during pregnancy.
Many herbs are not considered safe in pregnancy due to a lack of evidence. Clients who have
questions about an herbal ingredient or product can be encouraged to check with a
healthcare provider educated about herbal products (e.g. pharmacist, RD) or call 811 to ask a
Health Link RD.
Are nutrition supplement drinks needed during pregnancy?
Nutrition supplement drinks (e.g. Similac Mom
TM
, Ensure
TM
, Boost
TM
) are not required for a
healthy diet during pregnancy. They have no nutrition benefit over a healthy food snack (e.g.
whole grain toast, peanut butter, and milk) and are low in fibre.
41,117
Many nutrients aren’t
found in supplement drinks that can only be found in real food. People are encouraged to eat
a variety of foods from Canada’s food guide daily.
43
Nutrition supplement drinks are not
recommended as a multivitamin supplement replacement as they do not contain the right
amount of nutrients included in recommended multivitamin supplements such as folic acid,
vitamin D, and iron. If people are using these products regularly while pregnant, they may be
at risk of both inadequate and/or excessive intake of certain nutrients.
Consider recommending individual consultation with an RD if there is concern about a
person’s nutrient intake from food or supplement intakes during pregnancy.
See also:
When is a referral to a registered dietitian recommended?

Nutrition Guideline
Revised January 2024
Page 38
Pregnancy
Food Safety During Pregnancy Return to Key Questions
Why is foodborne illness a concern during pregnancy?
Both the individual who is pregnant and their fetus are at higher risk for foodborne illness
compared to a person who is not pregnant. Foodborne illness is caused by eating foods that
have been contaminated by toxins or harmful organisms such as bacteria, parasites, and
viruses.
118
During pregnancy, the higher production of progesterone can cause the immune
system to become suppressed, making it more difficult to fight off infections.
119
Some
bacteria can pass through the placenta and this can be problematic for the unborn baby.
118,120
The consequences of foodborne illness during pregnancy can result in miscarriage, stillbirth,
or a baby born premature or ill.
118,119
What is the best way to reduce the risk of foodborne illness during
pregnancy?
Safe food handling is the best way to reduce the risk of foodborne illness. People can reduce
their risk of foodborne illness by properly cooking, cleaning, chilling, storing, and separating
foods.
121
Advise individuals who are pregnant to follow basic food safety practices:
118
• Wash hands (with warm, soapy water for at least 20 seconds):
o Before handling any food.
o After handling food such as raw meat, poultry, and fish.
o After handling animals or pets.
• Wash all raw fruit and vegetables thoroughly. Wash food with potable water.
• Keep raw foods and cooked foods separate.
• Wash and disinfect (with diluted household bleach) food preparation surfaces and utensils
that have been in contact with raw meat, poultry, fish, and seafood.
• Use refrigerated raw meat, poultry, fish, and seafood by the “best before” date, or no more
than 2–4 days after buying it.
• Make sure hot foods are hot (above 60°C/140°F), cold foods are cold (below 4°C/39°F),
and all meats are well-cooked. Cook eggs until the yolk is firm.
• Cook meats, poultry, fish, and seafood to their safe internal temperature (refer to the Safe
Internal Cooking Temperatures Chart).
• Cool cooked foods quickly. Bacteria can grow if left out for more than 1 hour during
summer outdoor activities or 2 hours at room temperature.
• Reheat any cooked food to at least 74°C/165°F.
118,121
Reheat leftovers only once.
118,121
• Eat refrigerated leftovers as soon as possible (within 2–4 days).
See also:
What resources are available for the public?

Nutrition Guideline
Revised January 2024
Page 39
Pregnancy
What foods are people advised to avoid during pregnancy and are there
safer alternatives?
People who are planning to become pregnant and those who are pregnant are advised to
avoid many raw and undercooked foods. Table 11 provides a summary of foods to avoid and
safer alternatives during pregnancy.
118
Table 11. Foods to Avoid and Safe Food Alternatives for Pregnancy
Foods to Avoid
Safer Alternatives
• Raw and undercooked: fish (e.g. sushi),
shellfish (e.g. raw oysters), meats (e.g.
steak tartare), and poultry.
• Oysters, clams, and mussels that are cooked until
the shell has opened.
• Sushi that does not contain raw fish.
• Meat and poultry that are cooked to a safe internal
temperature.
o Beef or pork (including ground) 71°C (160°F)
o Wild game (deer, elk, small game) 74°C (165°F)
o Poultry 74°C (165°F)
o
Fish 70°C (158°F)
• Ready-to-eat meat and poultry such as
hot dogs and deli meats (e.g. bologna,
roast beef, and turkey breast).
• Dried and salted deli meats (e.g. salami and
pepperoni).
• Hot dogs and deli meats can be eaten if heated
until steaming hot.
o Heat deli meats and hot dogs to at least 74°C
(165°F)
• Refrigerated pates, meat spreads,
smoked seafood, and fish.
• When these products are sold in a can.
• When they are heated to a safe internal
temperature.
o Heat refrigerated meat spreads, smoked fish,
or shellfish until at least 74°C (165°F)
• Foods that contain raw or undercooked
eggs such as homemade Caesar
vinaigrette, cookie dough, cake batter,
and homemade eggnog.
• Cook eggs until the yolk is firm.
• Egg dishes that are well cooked to a safe internal
temperature of 74°C (165°F).
• Pasteurized eggnog
• Use pasteurized egg products when making
uncooked food that calls for raw eggs.
• Foods that contain raw or undercooked
flour (e.g. raw dough or batter or any other
product containing raw non-baked
flour).
122
• Cooked flour.

Nutrition Guideline
Revised January 2024
Page 40
Pregnancy
Foods to Avoid
Safer Alternatives
• Raw or unpasteurized milk and dairy
products (e.g. yogurt made from
unpasteurized milk).
• Pasteurized milk.
• Pasteurized dairy products that are cooked, in a
casserole or au gratin.
• Unpasteurized
and
pasteurized soft, semi-
soft and blue-veined cheeses such as
Havarti, Brie, Camembert, and Mexican-
style cheeses (e.g. queso fresco, queso
blanco).
• For additional information on cheese safety during
pregnancy see:
What are the food safety concerns
with cheese and what are safe cheese choices?
• Unpasteurized fruit juice and cider.
• Pasteurized fruit juice and cider.
• Raw and cooked sprouts (e.g. alfalfa,
clover, radish, and mung bean). Usual
cooking methods don’t consistently cook
sprouts thoroughly to make them safe for
consumption.
Source: Health Canada, 2016 Aug 09
118
Is it safe to consume fish during pregnancy?
Most fish can be safely consumed during pregnancy. Fish is a widely consumed, highly
nutritious source of protein, vitamin D, and omega-3 fatty acids.
36
Health Canada
recommends that people eat at least 150 g (5 oz) of cooked fish every week while pregnant.
36
Along with the potential benefits of fish consumption, there are risks of exposure to harmful
contaminants. A form of mercury known as methylmercury (MeHg) is a toxin present in the
environment and trace amounts in all foods,
58
with fish being the primary source for
humans.
123
Infants who have had very high MeHg exposure in the womb may experience
neurodevelopment abnormalities.
124
At chronic lower exposure levels, other
neurodevelopment deficits, such as deficits in memory, motor, attention, and verbal skills,
may also occur.
124
Individuals who are pregnant are advised to:
• consume a variety of fish and shellfish that are low in MeHg and high in omega-3 fatty
acids. Fish that are low in MeHg include anchovy, capelin, hake, herring, Atlantic mackerel,
pollock (Boston bluefish), salmon (farmed and wild), smelt, rainbow trout, shrimp, clams,
mussels, and oysters.
123
• choose canned “light” tuna instead of canned “white” or albacore tuna – as “light” tuna
contains less MeHg.
58,123
• avoid fish that are high in MeHg. High MeHg fish include fresh or frozen tuna, shark,
swordfish, escolar, marlin, and orange roughy.
123
• avoid raw fish and shellfish to reduce the risk of bacterial illness.
9,118

Nutrition Guideline
Revised January 2024
Page 41
Pregnancy
Fish consumption advisories for fish caught in Alberta lakes and rivers can be accessed at
aephin.alberta.ca/ShouldIEatThisFish
or by calling Alberta Environment and Sustainable
Resource Development toll-free at 1-877-944-0313.
A free mobile app for fish consumption developed by the Government of Alberta is available
on Apple and Google Play platforms.
125
The app is called Should I Eat This Fish?
See also:
What advice can be given about omega-3 fatty acid supplements during pregnancy?
What are the food safety concerns with cheese and what are safe cheese
choices?
Soft, semi-soft, and blue-veined cheeses have a higher risk of Listeria monocytogenes
(L. monocytogenes) contamination, which can result in listeriosis. The highest incidence of
listeriosis is amongst the vulnerable population including individuals who are pregnant.
126
Symptoms of listeriosis are typically mild in people during pregnancy, but the passage of the
organism through the placenta can cause miscarriage, stillbirth, perinatal septicemia, and
meningitis in the newborn baby.
126
Due to the risk it carries to the unborn child, individuals who
are pregnant are advised to follow cheese safety recommendations.
Soft, semi-soft, and blue-veined cheeses contain higher levels of moisture than hard or firm
cheeses. Higher moisture content can aid in the growth of L. monocytogenes. In addition, soft,
semi-soft, and blue-veined cheeses can also support the growth of the bacteria
L. monocytogenes if contaminated after pasteurization (e.g. during packaging, while storing at
home).
127
Safe cheese choices during pregnancy include:
118,128
• hard cheeses (e.g. parmesan, Romano), firm cheeses (e.g. cheddar, Swiss, and Colby)
processed cheese slices and spreads, cream cheese, and cottage cheese when made from
pasteurized milk.
• well-cooked soft, semi-soft, and blue-veined cheeses made from pasteurized milk.

Nutrition Guideline
Revised January 2024
Page 42
Pregnancy
Clarification on cheese safety messaging:
• AHS's recommendations are more cautious and advise the public is to choose pasteurized
milk products.
o Health Canada resources list unpasteurized hard cheeses as a safe alternative, due to
their low moisture content.
118
o Health Canada resources list cheese dishes (e.g. casserole or au gratin) that contain
unpasteurized and/or pasteurized soft, semi-soft, and blue-veined cheeses as safe to
consume if cooked to an internal temperature of 74°C (165°F).
118,129
• Popular cheeses such as mozzarella, feta, Monterey Jack, and paneer can vary in risk.
Advise people to consume only when cooked well when pregnant.
126,128,130
What are other food-related safety considerations?
Arsenic
Arsenic is a naturally occurring element found in our environment. It can enter groundwater
through soil or erosion, and compounds of arsenic can be used for the manufacturing of
products that can enter our environment.
131,132
Arsenic may be found at very low levels in many
foods including meat and poultry, milk and dairy products, bakery goods and cereals,
vegetables, fruits and fruit juices, and fish and shellfish.
132
The inorganic form of arsenic is of
concern as it may contribute to potential adverse health effects including an increased risk of
cancer.
131,132
Rice and some types of seaweed can contain higher amounts of inorganic arsenic
compared to other foods.
132
Some evidence has shown a positive relationship between in-utero arsenic exposure and
acute respiratory tract infections among infants when high levels of arsenic were present in
drinking water.
133
There are limitations in the research studies investigating associations
between arsenic and adverse outcomes.
133,134
As well, there is uncertainty about short and
long-term health risks associated with a low dose, chronic arsenic exposure.
135
More research is needed to determine if there is an association between levels of arsenic
exposure during pregnancy and adverse outcomes in infants and children. The Canadian Food
Inspection Agency (CFIA) continues to monitor arsenic in foods and the potential human
health risks associated with arsenic exposure.
132
People are advised to follow a balanced diet
that contains a variety of grains and whole grains (e.g. barley, oats, rice, and wheat).
135

Nutrition Guideline
Revised January 2024
Page 43
Pregnancy
Flaxseed and Flaxseed Supplements
There is insufficient evidence regarding the safety of flaxseed in pregnancy.
91,92
Current
recommendations are for individuals who are pregnant to restrict their consumption of
flaxseed to the amounts commonly found in foods or to a maximum of 1 tbsp (15 mL)/day.
91
During pregnancy, people are also advised to avoid flaxseed oil.
92
See also:
What advice can be given about omega-3 fatty acid supplements during pregnancy?
Honey
Both pasteurized and unpasteurized honey are considered safe for consumption during
pregnancy.
136
Questions about the safety of honey arise because it can be contaminated with
the spores of the bacteria Clostridium botulinum, which can grow in the digestive tract and
produce harmful toxins, leading to botulism.
136–139
In healthy adults, including during
pregnancy, the digestive tract is able to protect against botulism infection.
136,140,141
Botulism in
adults is very rare.
136,140,141
Honey has very low moisture content and high acidity, which makes
contamination of honey with other harmful bacteria unlikely.
137
Honey is not recommended for
children under one year of age as they are at risk of developing botulism because they have
yet to develop sufficient protective bacteria in their intestines.
142
Liver
Individuals who are consuming foods high in preformed vitamin A, especially liver, may be at
risk of exceeding the UL for vitamin A, depending on preformed vitamin A intake from other
food and supplement sources. People are recommended to limit their consumption of beef
liver, particularly during the first trimester of pregnancy, to less than 75 grams (2½ ounces)
every two weeks.
1,96
Public resources are more cautious in their recommendations and may
suggest individuals who are pregnant limit liver consumption to no more than
75 g (2½ ounces) every two weeks, with no specification for the trimester of pregnancy.
143
This recommendation is below the tolerable upper limit level (UL) for vitamin A and
considered safe for individuals
α
who are pregnant when taking a multivitamin supplement
containing vitamin A.
96
Individual assessment and counselling by an RD can support people in adapting food and
nutrient recommendations to their unique situations.
See also:
What is the concern with vitamin A supplements in pregnancy?
When is a referral to a registered dietitian recommended?

Nutrition Guideline
Revised January 2024
Page 44
Pregnancy
Probiotic-containing Foods
Probiotics consumed in moderation from common foods with a long history of consumption
such as yogurt and kefir are generally considered safe.
24
The probiotics generally used in
these foods are usually Lactobacillus and Bifidobacterium.
144
Advise individuals who are
pregnant to check with their care provider before consuming other popular food products. A
specific example of a probiotic food product that has health and safety risks,
145,146
may have
adverse effects in immunocompromised individuals
145
and is not recommended during
pregnancy is kombucha tea of any form.
147
Few probiotic strains have been tested for their safety during pregnancy.
148
Adverse effects
have been reported for the probiotic Saccharomyces.
148
Advise people who are pregnant and
considering taking probiotic supplements that limited evidence exists on the safety of their
use during pregnancy and it is best to avoid probiotic supplement use.
Soy-containing Foods
The amount of soy commonly found in foods or beverages is unlikely to be a concern during
pregnancy.
1,95
Soy protein supplements or isoflavone supplements are not recommended
during pregnancy as high intakes are mildly estrogenic and potentially could adversely affect
fetal development.
1,95
Sugar Substitutes
Moderation is encouraged when consuming or recommending products sweetened with sugar
substitutes.
149
Sugar substitutes include artificial sweeteners and intense sweeteners
obtained from natural sources.
150
They may be bought as tabletop products or present in
beverages (such as pop or fruit-flavoured beverages), ‘diet’ products, yogurt, breakfast
cereals, canned fruit packed in water, baked goods, desserts, spreads, salad dressings, and
chewing gums.
The moderate use of sugar substitutes during pregnancy is considered safe.
149
It is
recommended that people who are pregnant avoid excessive consumption of products
containing sugar substitutes as such foods could replace nutrient-dense, energy-yielding
foods.
149

Nutrition Guideline
Revised January 2024
Page 45
Pregnancy
Table 12. Sugar Substitutes and Common Brands Considered Safe in Moderate Amounts
151
Sugar Substitutes
Common Brand Names
Acesulfame Potassium Ace-K or Sunett
®
Aspartame Nutrasweet
®
, Equal
®
, private label brand
Saccharin Hermesetas
®
Stevia Krisda
®
, Truvia
®
, stevia, Pure Via
TM
Sucralose (Splenda
®
)
Note: Advise clients to read the ingredient label as name brands and store brands can have multiple products with
different sugar substitutes. For example, the Sugar Twin
®
brand products may use cyclamate, sucralose, or stevia
sugar substitutes.
Cyclamates:
• Caution
149
or avoidance is recommended for the use of cyclamates (Sucaryl
®
, Sugar Twin
®
,
Sweet N’Low
®
, Weight Watchers Table-Top Sweetner
®
) during pregnancy due to unknown
risks associated with consumption above the acceptable daily intake (ADI) of 11 mg/kg
body weight. People who are using cyclamates are advised to limit their intake to below
the ADI. Limit intake to two packages of Sugar Twin
®
containing cyclamate/day to remain
within this recommendation.
152
Stevia leaves:
• Stevia leaves (fresh, dried, or powdered) and crude extracts of stevia leaves are available
in Canada for use in personal cooking.
150
The safety of this product for consumption during
pregnancy is not known.
153
Other:
• Other sugar substitutes permitted for use in Canada
151
and considered safe for
consumption at or below the ADI for the specific sugar substitute include advantame,
D-tagatose, neotame, and thaumatin.
154
• Sugar alcohols permitted for use as food additives in Canada include hydrogenated starch
hydrolysates, isomalt, lactitol, maltitol, maltitol syrup, mannitol, sorbitol, sorbitol syrup,
xylitol, and erythritol. Health Canada advises that the consumption of approved sugar
alcohols does not pose a health risk during pregnancy.
154,155

Nutrition Guideline
Revised January 2024
Page 46
Pregnancy
Common Discomforts of Pregnancy Considerations
Return to Key Questions
Nausea and vomiting–what can be done during pregnancy?
Nausea and vomiting during pregnancy (NVP) is the most common medical condition of
pregnancy, affecting 50% to 80% of all individuals
α
who are pregnant.
156
In most cases NVP
subsides by the 16
th
week of pregnancy, however, up to 20% of individuals continue to have
symptoms throughout their pregnancy.
157
It is recommended that other causes of nausea and
vomiting (gastrointestinal, genitourinary, central nervous system, and toxic/metabolic
problems) be ruled out when assessing clients.
1
Hyperemesis gravidarum (HG) is a severe form of NVP that affects approximately 0.3–2% of
pregnancies.
156
HG has been defined as persistent and excessive vomiting starting before the
end of the 22
nd
week of pregnancy and may be diagnosed as mild or severe.
156
Severe HG may
include metabolic disturbances such as carbohydrate depletion, dehydration, and electrolyte
imbalance.
156
Large ketonuria and a significant weight loss of at least 5% from pre-pregnancy
weight are often included as criteria for diagnosis of HG.
1
Treatment for HG may require
hospitalization and interventions such as intravenous fluid replacement therapy, total
parenteral nutrition, and anti-nausea medication.
Individuals with NVP or HG can experience substantial physical and emotional impacts on
their daily functioning, affecting their well-being and quality of life. Supportive counselling
from any care provider is recommended to help clients deal more positively with the
effects.
156
Supplementation with a multivitamin containing iron may not be tolerated for some people
experiencing NVP. If a multivitamin supplement with iron is not tolerated and iron stores are
sufficient, a multivitamin supplement with lower iron or without iron may be taken until NVP
subsides. If any multivitamin supplement is not tolerated single vitamin supplements of
0.4 mg (400 mcg) folic acid and 400 IU vitamin D may be taken until NVP subsides.
156,157
Advise clients experiencing NVP to eat pregnancy-safe foods that are appealing and
tolerable to them while aiming for a healthy diet. Anecdotal evidence suggests dietary
strategies that may reduce symptoms of nausea and vomiting include:
• Eat small frequent meals every 1–2 hours to avoid a full stomach.
• Separate solids and liquids to prevent the stomach from becoming too full. For example,
eat a small portion of food, wait 20–30 minutes, then take some liquids.
• Choose dry, bland, salty, and/or high-protein foods for snacks and meals.
• Eat foods and beverages at room temperature and avoid those that are hot or cold
(depending on personal preference).

Nutrition Guideline
Revised January 2024
Page 47
Pregnancy
• Choose lower-fat, higher-protein foods.
• Eat before getting out of bed and when nausea is less severe.
• Eat before, or as soon as feeling hungry to avoid an empty stomach that may aggravate
nausea.
• Do not swallow excessive saliva (spit out the saliva and rinse mouth frequently).
• Avoid offensive odours or sensory stimuli.
• Try colder fluids, including ice chips and Popsicles
®
.
Individuals with nausea are encouraged to drink fluids as tolerated, particularly fluids with
electrolytes if dehydration is a concern.
158
When liquids cannot be tolerated without vomiting
and vomiting has not responded to outpatient management, a physician may recommend
hospitalization for evaluation and treatment. Fatigue may exacerbate NVP; clients can be
encouraged to lie down as needed and increase rest.
156
Advise individuals experiencing NVP to
discuss the condition with their physician, especially when medical or alternative therapies for
NVP are being considered.
Constipation–what can be done during pregnancy?
Constipation occurs among 11–38% of people
α
during pregnancy.
9,159
It may occur as a side
effect of high doses of supplemental iron and/or as part of the digestive changes associated
with pregnancy.
9
Constipation is often caused by increased levels of progesterone and a
decrease in gut transit time in the second and third trimesters.
159
There is limited evidence to support the effectiveness of interventions to manage
constipation during pregnancy.
9
Anecdotal evidence suggests strategies that may reduce
symptoms of constipation include:
• Drinking 10 cups (~2.5 L) fluids every day.
9
One cup is equivalent to 250 mL (8 oz). This
total amount of fluids includes all types of non-alcoholic beverages such as milk and
plant-based beverages and fluids found in soups. Water is recommended to be the main
source of fluids.
9
• Increasing fibre intake by eating high-fibre foods including legumes such as beans, split
peas and lentils, whole grain breads, 100% bran cereals, and vegetables and fruit.
9
• Regular physical activity including safe activities during pregnancy such as walking and
swimming.
9
Additional support from an RD is recommended for people with severe ongoing constipation
issues for dietary intervention. Advise clients to discuss the use of fibre supplements and
laxatives with a physician before use.
See also:
When is a referral to a registered dietitian recommended?
What advice can be given to people about physical activity during pregnancy?

Nutrition Guideline
Revised January 2024
Page 48
Pregnancy
Heartburn–what can be done during pregnancy?
Approximately 17–45% of individuals
α
who are pregnant experience acid reflux or heartburn.
9
Heartburn is a sensation of burning in the upper part of the digestive tract including the
throat. It is caused by pregnancy hormones affecting the muscle that keeps food in the
stomach and letting acid in the stomach come back up the throat.
160
Heartburn is a concern if
it discourages eating during pregnancy. Relief from heartburn may be achieved through
dietary and lifestyle changes. However, there has been no evidence-based recommendation
for the treatment of heartburn in pregnancy.
160
Anecdotal evidence of strategies that may reduce symptoms of heartburn include:
• avoiding foods and drinks that make symptoms worse
160,161
• eating small, more frequent meals
9,160–162
• eating slowly and chewing food well
162
• drinking fluids between meals, not with meals
162
• avoiding carbonated drinks and beverages containing caffeine
9,162
• avoiding lying down right after eating
9,161,162
• raising head and shoulders when lying down
9,160–162
• avoiding fried or greasy foods
9,162
People with resistant symptoms are recommended to seek advice from their physicians about
the use of over-the-counter and prescription medications to relieve symptoms.
Health Condition Considerations in Pregnancy
Return to Key Questions
Are there special nutrition considerations regarding diabetes in
pregnancy?
Nutrition counselling by an RD is a recommended component of care for people at risk for or
diagnosed with diabetes in pregnancy, including people with pre-existing type 1 diabetes,
type 2 diabetes, or those diagnosed with gestational diabetes mellitus (glucose intolerance
with onset or first recognition during pregnancy).
163
Individuals with pre-existing diabetes
(type 1 or type 2) who are of reproductive age are advised to seek preconception care from an
interdisciplinary team.
163
Recommended counselling components for individuals with pre-
existing diabetes include the importance of glycemic control prior to pregnancy, the impact
of BMI on pregnancy outcomes, and the need for a multivitamin supplement containing 1 mg
(1000 mcg) folic acid every day, starting at least three months prior to pregnancy.
163

Nutrition Guideline
Revised January 2024
Page 49
Pregnancy
People at high risk for gestational diabetes mellitus (GDM) can be referred for nutrition
counselling on healthy eating and prevention of excessive gestational weight gain in early
pregnancy, ideally, before 15 weeks of gestation, to reduce the risk of developing GDM. Risk
factors for GDM include:
163
• age 35 or older
• BMI greater than or equal to 30 kg/m
2
• member of a high-risk population (Indigenous, Hispanic, South Asian, Asian, African, Arab)
• parent or sibling with type 2 diabetes
• corticosteroid use
• prediabetes
• previous GDM diagnosis
• previous delivery of a macrosomic infant (large for gestational age)
• polycystic ovarian syndrome
• acanthosis nigricans (darkened patches of skin)
Screening for GDM at 24–28 weeks gestation is recommended for all people during
pregnancy while screening at any stage of pregnancy is recommended for people with a high
risk of GDM.
163
Individualized nutrition care from an RD for people at risk for or diagnosed with
diabetes in pregnancy can promote adequate nutrition intake, achievement of target glucose
levels, and appropriate weight gain and growth of the fetus.
163
See also:
When is a referral to a registered dietitian recommended?
For related Nutrition Guidelines see: Nutrition Guideline: Diabetes in Pregnancy
Are there nutrition considerations for hypertensive disorders of
pregnancy?
Hypertensive disorders of pregnancy are the leading cause of adverse health and perinatal
outcomes.
1
Hypertensive disorders of pregnancy include pre-existing hypertension,
gestational hypertension, and pre-eclampsia or eclampsia.
11
Risks of uncontrolled pre-
eclampsia include preterm delivery, intrauterine growth restriction, and morbidity and
mortality during pregnancy.
9
It is advised that individuals with pre-existing or chronic hypertension manage their blood
pressure by monitoring sodium intake and following a balanced diet.
164
Individuals who are
pregnant and have chronic hypertension combined with inadequate calcium intake during
pregnancy may require a calcium supplement in doses of 1000–2500 mg per day to reduce
their risk of preeclampsia.
22
Referral to an RD is recommended to assess adequate calcium
intake and the need for supplementation among clients with chronic hypertension.

Nutrition Guideline
Revised January 2024
Page 50
Pregnancy
Different dietary interventions for the prevention of gestational hypertension have been
suggested. These include dietary salt restriction, calcium supplementation, vitamin D
supplementation (alone or combined with calcium supplementation), multivitamin supplement
with folic acid, and vitamin C and/or E supplementation.
22
However, there is insufficient
evidence at this time to make recommendations for specific dietary interventions or
strategies.
22,23
A healthy pre-pregnancy body weight is associated with a decreased risk of
gestational hypertension. Note, however, that individuals are advised to follow the weight
gain recommendations for their pre-pregnancy BMI. Weight loss or caloric restriction at any
time during pregnancy is not recommended.
22
To manage hypertensive disorders during pregnancy, individuals who are pregnant are
advised to:
• follow recommendations for adequate weight gain during pregnancy.
• monitor sodium intake and follow a balanced diet following Canada’s food guide.
• take a multivitamin supplement that meets the recommendations of iron, folic acid, and
vitamin D every day.
• meet calcium requirements with calcium-rich foods or to talk with an RD to assess the
need for single mineral supplementation.
See also:
When is a referral to a registered dietitian recommended?
How much weight gain is appropriate during pregnancy?
Nutrients: Calcium and Vitamin D
Are there recommended foods to avoid during pregnancy to prevent
infant allergies?
There is insufficient evidence to recommend avoidance of any single nutrient or any single
food during pregnancy to prevent an allergy from developing in the infant.
165
During
pregnancy, no restriction or avoidance of particular foods
166
or addition of foods or
supplements
167
are proven to prevent allergy in the infant at this time. This is an area of
current research.
166,167
During pregnancy, people are advised to follow a varied diet based on Canada’s food guide.
Dietary exclusion of nutritious foods can put the individual who is pregnant and their fetus at
risk of nutrition inadequacy. When there is a diagnosed allergy, it is necessary to avoid foods
that contain the allergy. There is evidence that reducing the number of times a person suffers
from allergic reactions while pregnant can help reduce infant morbidity and mortality.
168,169
Nutrition Guideline
Revised January 2024
Page 51
Pregnancy
Refer individuals with multiple food allergies, or who restrict foods (protein foods, grains,
and/or fruits and vegetables) due to pre-existing allergies, to an RD for nutrition counselling.
See also:
When is a referral to a registered dietitian recommended?
Adolescent Pregnancy Return to Key Questions
Adolescent pregnancies are considered high-risk.
170,171
Adolescents who are pregnant are at
increased risk of anemia, preterm birth, intrauterine growth restriction (IUGR), low birth
weight (LBW), congenital anomalies, neonatal intensive care unit (NICU) admissions, and
neonatal death.
170
Evidence suggests that medical risks are most severe for adolescents
under 15 years.
171
What are the nutrients of concern for pregnancy during adolescence?
The growing adolescent has distinct nutrition needs compared to adults, such that their
nutrient requirements are higher than at any other point in life.
172
Limited evidence suggests
that nutrient intakes that fall most frequently below the DRI for adolescents during
pregnancy are energy, iron, folate, calcium, vitamin E, and magnesium.
171
Dietary survey
findings from the 2004 Canadian Community Health Survey indicate that adolescents have
inadequate intakes of nutrients of concern in pregnancy including folate, vitamin B
12
, calcium,
iron, and fibre.
173
During pregnancy, adolescents’ calcium needs are higher than those of
adults.
48
Adolescents who are pregnant need a total of 1300 mg calcium and 600 IU vitamin D
daily to meet their requirements.
48
Energy needs are influenced by many factors, including growth status, pregravid weight,
physical activity, stage of pregnancy, and body composition. Adolescents who are pregnant
are at increased risk of anemia, and monitoring by their care provider for diagnosis and
treatment is recommended.
166
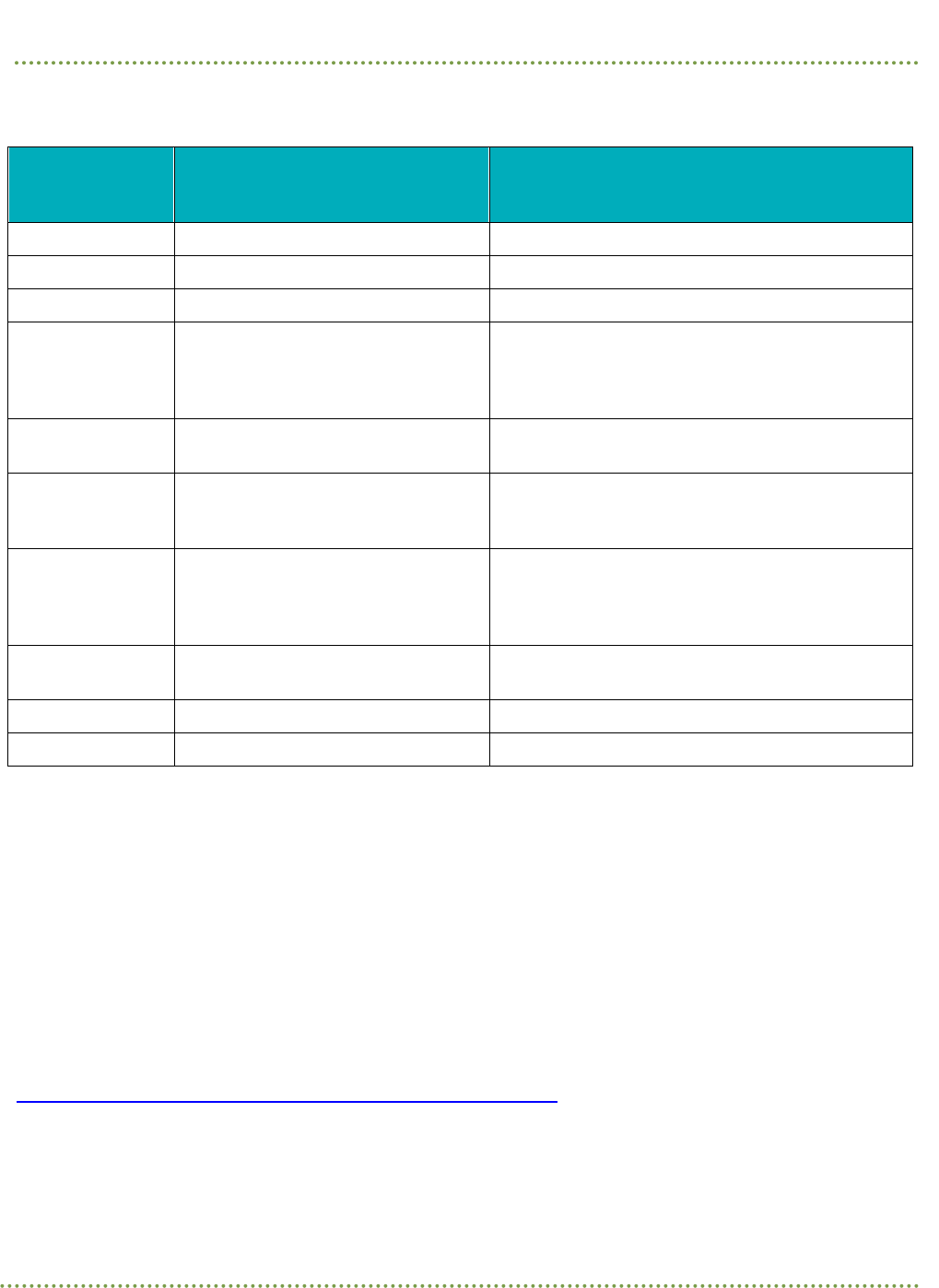
Nutrition Guideline
Revised January 2024
Page 52
Pregnancy
Table 13. Nutrient Amounts Recommended for Adolescent Pregnancy from All Sources
(food, multivitamin supplement, single-source supplement)
Nutrient
Recommended Amount Per Day
for Adolescent Pregnancy
(under 19 years)
Upper Limit (UL)
Calcium 1300 mg
a
Total daily intake not to exceed 3000 mg
a
Choline 450 mg
a
Total daily intake not to exceed 3.0 g
a
Fibre 28 g
a
Safe upper limit not defined
a
Folate/Folic
Acid
0.6 mg (600 mcg)
a
0.8 mg (800 mcg
a
)
The UL for folate applies only to synthetic forms
obtained from supplements, fortified foods, or a
combination of the two
a
Iodine 0.22 mg (220 mcg)
a
Total daily intake not to exceed 1.1 mg
(1100 mcg)
a
Iron 27 mg
a
Total daily intake not to exceed 45 mg
a,b
unless
advised by a physician. Monitor iron status
closely.
Omega-3 Fatty
Acids (DHA and
EPA)
Include at least 150 g (5 oz) cooked
fish rich in omega 3 fatty acids and
low in mercury each week during
pregnancy
c
Safe upper limit not defined
c
Vitamin A 750 mcg
a
(2500 IU) 2800 mcg
a
(9333 IU
UL is for preformed vitamin A only
a
Vitamin B
12
2.6 mcg
a
Safe upper limit not defined
a
Vitamin D 600 IU
a
Total daily intake not to exceed 4000 IU
a
Sources:
a
Health Canada, 2010. Dietary Reference Intake Tables
34,48
b
IOM 2006
48
c
Health Canada, 2009. Prenatal Nutrition Guidelines for Health Professionals: Fish and Omega-3 Fatty Acids
37
Referral to an RD for nutrition assessment and counselling is recommended, as this may
result in improvements in mean birth weights, reduced low birth weight, and reduced preterm
birth.
170,174
Referral to a Canada Prenatal Nutrition Program, where projects are available in
their community, is also recommended.
See also:
When is a referral to a registered dietitian recommended?

Nutrition Guideline
Revised January 2024
Page 53
Pregnancy
What are the recommendations for gestational weight gain in adolescents?
Adolescents are at increased risk of preterm delivery and having low birth weight (LBW) and
small gestational age (SGA) infants. The 2009 IOM report concluded there is insufficient
evidence to support a modification of the gestational weight gain guidelines for adolescents
greater than two years post-menarche.
32
The IOM and the AND recommend that adolescents
gain weight within the ranges for adult individuals
α
for their pre-pregnancy BMI category.
9,32
Very young adolescents (under 16 years of age) are at higher risk of delivering a small infant
compared to those aged 16 years and older, despite the similar weight gain, and are advised to
strive for weight gain at the upper end of the recommended range for their pre-pregnancy BMI
category.
32
Nutrition assessment and counselling regarding weight gain during pregnancy is
recommended for all adolescents.
170
See also:
When is a referral to a registered dietitian recommended?
How much weight gain is appropriate during pregnancy?
Substance Use During Pregnancy Return to Key Questions
Is it safe to consume alcohol during pregnancy?
Advise all people to avoid alcohol during pregnancy.
9,175,176
Alcohol consumption in pregnancy
can cause fetal harm.
9,175–177
Alcohol is a teratogen that can cross the placenta and pass from
parent to fetus. It is well established that exposure to alcohol at high-risk levels can have
physical and neurodevelopmental effects on the infant.
175
Evidence of fetal safety or harm at low levels of alcohol consumption is inconsistent; therefore,
a safe level of alcohol consumption cannot be established.
9,175,177
Amount, timing, and frequency
of alcohol intake alongside factors such as fetal genetic susceptibility and the health of the
individual impact fetal alcohol spectrum disorder (FASD) risk.
178
Alcohol abstinence during
pregnancy prevents FASD and the resulting birth defects and developmental disabilities.
178
Care providers are advised to create a safe environment for people to report alcohol
consumption and to offer motivational counselling strategies aimed at helping to reduce or
eliminate alcohol use.
175
Is it safe to consume cannabis during pregnancy?
Evidence exists about the side effects of cannabis or cannabis-derived products (e.g. cannabis
edibles) used during pregnancy.
179
Cannabis use has been linked to birth defects, premature
delivery, and low birth weight.
180
People are advised to avoid the use of these products
throughout pregnancy and lactation.
179,180

Nutrition Guideline
Revised January 2024
Page 54
Pregnancy
Physical Activity During Pregnancy Return to Key Questions
What needs to be considered when discussing physical activity during
pregnancy?
There are many benefits to being physically active throughout pregnancy for both parent and
fetus. Physical activity during pregnancy has been shown to have benefits such as the
prevention of excessive gestational weight gain, gestational diabetes, and hypertensive
disorders, as well as impacting appropriate birth weight, the timing of delivery, and child body
composition.
181–183
Contraindications to physical activity may include, but are not limited to
previous preterm birth or spontaneous abortion, intrauterine growth restriction, anemia,
malnutrition or eating disorder, and other medical conditions such as uncontrolled type 1
diabetes, pregnancy-induced hypertension, and cardiovascular, respiratory, or systemic
disorders.
183
The key recommendations of the 2019 Canadian Guideline for Physical Activity throughout
Pregnancy are:
183
• Physical activity reduces the risk of common pregnancy complications.
• It is recommended to accumulate at least 150 minutes of moderate-intensity physical
activity each week. There are many ways to achieve this including activities such as
walking, that have minimal added expenses.
• Previously inactive people can safely start physical activity and gradually progress toward
the recommended amount.
When participating in physical activity people should be cautious of activities where falling or
direct physical contact may result in harm to themselves or their fetus.
Individuals who are pregnant are advised:
• to be physically active throughout pregnancy unless they have contraindications to being
physically active and/or have been told not to be active by a care provider.
• to consult with their physician, obstetrician, or another prenatal provider (nurse
practitioner or midwife) regarding advice about physical activity.
• that a physical activity professional (such as a kinesiologist, certified exercise
physiologist, or an exercise therapist) can provide advice on being physically active
throughout pregnancy

Nutrition Guideline
Revised January 2024
Page 55
Pregnancy
Other Special Considerations Return to Key Questions
Are there special considerations when working with individuals with
culturally diverse backgrounds (e.g. Indigenous peoples, immigrants, and
refugees)?
Pregnancy may be a time for many people that provokes culturally-based responses and
reactions from themselves, their families, and others. Care providers are encouraged to
approach each client interaction as unique, avoiding stereotyping possible cultural influences
in pregnancy based on past experiences or knowledge of cultural food practices.
Care providers are advised to continually assess and improve their own cultural competence.
While no care provider can be an expert in all aspects of diversity, cultural competence
involves continual learning that arises from experiences, encounters, and ongoing reflection.
7
What are other important considerations when working with any
individual?
Household Food Insecurity
Household food insecurity (HFI) is defined as “an inadequate or insecure access to food
because of financial constraints”;
184
it impacts physical, mental and social well-being. Care
providers will encounter clients living in food-insecure households, due to the high prevalence
of HFI among those accessing health care.
185
HFI is best addressed through income-based interventions.
184,186,187
Those experiencing HFI
have food preparation, budgeting, and cooking skills similar to the general population.
188
Interventions focused on food skills do not protect people from, nor improve HFI.
188
Emergency food programs (e.g. food banks) may provide temporary relief.
189
However, these
programs do not solve HFI and are inappropriate and/or inaccessible for many clients.
189
Care providers can offer better support if they are aware when clients are worried about
having enough money for food and are experiencing other challenges because of financial
strain.
190,191
Care providers are encouraged to work with clients to develop interventions that
are sensitive to financial strain.
Key steps for care providers include:
• Learn about financial strain, how to screen clients for poverty, and the link between
poverty and poorer health through the
Identifying Financial Strain and Addressing
Financial Barriers to Health Care Modules; available on MyLearningLink for AHS staff
and on CLiC for Covenant Health staff.

Nutrition Guideline
Revised January 2024
Page 56
Pregnancy
• Review the Nutrition Guideline: Household Food Insecurity for additional information on
how to support clients experiencing HFI.
• Assist clients in accessing available income supports. 211 Alberta (ab.211.ca) is a provincial
directory that can be used to identify financial benefits, programs, and services.
Cost can be an obstacle to timely and appropriate folic acid supplementation and a significant
barrier to healthy eating during pregnancy.
40
Support clients can access all eligible
pregnancy-specific special diet funding and vitamin and mineral supplementation funding.
Additional income or nutrition supplement support may exist for individuals during their
pregnancy:
• People who receive Assured Income for the Severely Handicapped (AISH) or Income
Support (Alberta Works) may be eligible for funding to help cover the cost of a healthy
diet during pregnancy.
• Multivitamin supplements may be available through the Alberta Adult Health Benefit
(AAHB), Alberta Child Health Benefit (ACHB), Interim Federal Health Program (IFHP), the
Non-Insured Health Benefits (NIHB) for First Nations and Inuit, Assured Income for the
Severely Handicapped (AISH), and Income Support (Alberta Works).
Refer to the Point of Care Reference: Funding Options for Special Diets and Nutrition
Products (via ahs.ca/FoodInsecurity
) for details on all programs, eligibility and required steps
to access coverage.
Canada Prenatal Nutrition Program
(CPNP) projects in your community may provide vitamins,
food, food coupons, and/or nutrition counselling.
Referral to a Registered Dietitian Return to Key Questions
When is a referral to a registered dietitian (RD) recommended?
A nutrition assessment by an RD will help determine if an individual has adequate calorie and
nutrient intake. In addition to calorie and macronutrient intake, specific micronutrients to be
assessed in pregnancy include calcium, vitamin D, omega-3 fatty acids, folic acid, and iron.
Referrals for individual nutrition assessment and counselling by an RD are especially
important for individuals who:
• Are adolescents (less than 15 years old or less than 3 years since the onset of menses).
• Are pregnant with twins, triplets, or higher-order multiples.
• Previously had a low birth weight infant.
• Have a low pre-pregnancy weight–defined as less than 90% of desirable body weight or
BMI less than 18.5 kg/m
2
.

Nutrition Guideline
Revised January 2024
Page 57
Pregnancy
• Have a poor weight gain in the second or third trimester–defined as less than 0.25 kg
(0.5 lbs)/week for people with a pre-pregnancy BMI of 18.5–24.9 kg/m
2
and less than 0.5
kg
(1 lb)/week for multiple gestations and people with a pre-pregnancy BMI below 18.5 kg/m
2
.
• Have a nutrition-related health condition they are managing in conjunction to their
pregnancy, such as gestational diabetes, pre-eclampsia, or other medical conditions with
an impact on nutrition (e.g. inflammatory bowel disease, bariatric surgery, celiac disease).
Other reasons that could indicate an RD referral:
• Severe nausea and vomiting of pregnancy.
• Higher requirements for specific nutrients (e.g. additional folic acid needs above those
recommended for most pregnancies).
• Weight gain during pregnancy that exceeds the recommended range based on pre-
pregnancy BMI
• Risk for poor nutrient intake due to other factors including alcohol and substance use,
poverty, and low socioeconomic status.
• Food allergies or food intolerances that cause severe food restrictions.
• Other restricted patterns of eating such as following a restricted vegetarian or vegan
pattern of eating.
Referral processes will vary based on zone and site policy. Referral information and referral
forms can be found at the Alberta Referral Directory.
Members of the public can also access a dietitian through 811. If Albertans over the age of 18
have a nutrition question, they can complete a self-referral at ahs.ca/811
or call 811 and ask to
talk to a dietitian. For more information about the dietitian services offered through Health
Link, visit
Health Link Dietitian Service.
Resources Return to Key Questions
What resources are available for professionals?
Prenatal Nutrition Tool (PreNuT)
The Prenatal Nutrition Tool (PreNuT) helps prenatal programs or care providers identify
nutrition issues to discuss with clients during their pregnancy and offer client-centred
conversations about key nutrition issues. The tool is meant to be used by the care providers in
discussions with a client.

Nutrition Guideline
Revised January 2024
Page 58
Pregnancy
Nutrition Guidelines and Supporting Resources
• Nutrition Guidelines for care providers on a variety of healthy eating and active living
topics including general nutrition and nutrient information can be found on the
Nutrition
Guidelines page.
• Nutrition Guidelines for care providers on Pregnancy: Multiples.
• Health Canada Prenatal and Pregnancy Guidelines
• Resources to support healthy gestational weight gain:
o Healthy pregnancy weight gain charts for singletons
o BMI calculator wheel
o Healthy pregnancy weight gain poster
• An accredited continuing medical education learning program on healthy pregnancy
weight gain. Registration is free. All care providers are welcome to register.
o Look for Healthy Pregnancy Weight Gain in the listing of Self-Paced eLearning
Courses on the University of Calgary Continuing Medical Education and Professional
Development online learning platform.
• Clinical Practice Guideline on the Management of Nausea and Vomiting of Pregnancy
from the Society of Obstetrics and Gynecology Canada
• Natural Medicines Database provides information on health and safety considerations
associated with food, herbs, and supplements.
• A Clinical Guide to Probiotic Products Available in Canada: Translates scientific evidence
available for probiotic products into practical, clinically relevant information for health
care providers.
Community Programs for At-Risk Individuals
• The Canada Prenatal Nutrition Program (CPNP) is a community-based program that
provides support to improve the health and well-being of people who are pregnant, new
parents, and babies facing challenging life circumstances.

Nutrition Guideline
Revised January 2024
Page 59
Pregnancy
What resources are available for the public?
Preconception Health
• For information on preconception health: ReadyOrNotAlberta.ca
Pregnancy and Birth
• General pregnancy nutrition information for the public can be found in Healthy Parents,
Healthy Children.
• Health Canada has a website devoted to pregnancy information.
• Best Start has a How to Survive Morning Sickness Guide with tips for managing nausea
and vomiting of pregnancy
• My Health Alberta also has a video on Managing Morning Sickness
Nutrition Handouts
• For nutrition resources visit Nutrition Education Materials.
• To access pictorial handouts for clients who are pregnant look under "Pregnancy &
Breastfeeding". These pictorial handouts were created to support all individuals with food
knowledge and skill-building during pregnancy, including English language learners.
Food Safety Handouts
• Health Canada: Food Safety for Pregnant Women
α
. (Note: the sprout information does not
align with AHS recommendations)

Nutrition Guideline
Revised January 2024
Page 60
Pregnancy
References
1. O’Connor DL, Blake J, Bell R, Bowen A, Callum J, Fenton S, et al. Canadian Consensus on Female
Nutrition: Adolescence, Reproduction, Menopause, and Beyond. J Obstet Gynaecol Canada JOGC
= J d’obstetrique Gynecol du Canada JOGC. 2016;38(6):508-554.e18.
2. Ramakrishnan U, Grant F, Goldenberg T, Zongrone A, Martorell R. Effect of women’s nutrition
before and during early pregnancy on maternal and infant Outcomes: A systematic review.
Paediatr Perinat Epidemiol. 2012 Jul;26:285–301.
3. Procter SB, Campbell CG. Position of the Academy of Nutrition and Dietetics: nutrition and
lifestyle for a healthy pregnancy outcome. J Acad Nutr Diet. 2014 Jul;114(7):1099–103.
4. Bartick M, Stehel EK, Calhoun SL, Feldman-Winter L, Zimmerman D, Noble L, et al. Academy of
breastfeeding medicine position statement and guideline: Infant feeding and lactation-related
language and gender. Breastfeed Med. 2021;16(8):587–90.
5. Alberta Health Services. Guide to creating safer and more welcoming places for sexual and
gender minority (LGBTQ2S+) people. 2018; Available from:
https://insite.albertahealthservices.ca/Main/assets/tms/dvi/tms-dvi-diversity-inclusion-gender-
sexual-diversity-guide.pdf
6. World Health Organization. Health topics - congenital anomalies. [Internet]. 2019 [cited 2022 Jun
16]. Available from: https://www.who.int/topics/congenital_anomalies/en/
7. Betancourt JR, Green AR, Carrillo JE. Cultural Competence in Health Care: Emerging
Frameworks and Practical Approaches. Policy File. 2002 Oct 1;
8. Brown J. Nutrition through the lifecycle. 4th ed. Belmont (CA): Wadsworth, Cengage Learning;
2011.
9. Academy of Nutrition and Dietetics. Practice Paper of the Academy of Nutrition and Dietetics:
Nutrition and lifestyle for a healthy pregnancy outcome. J Acad Nutr Diet. 2014;114(9):1447.
10. Schoenaker D, Soedamah-Muthu SS, Mishra GD. The association between dietary factors and
gestational hypertension and pre-eclampsia: a systematic review and meta-analysis of
observational studies. BMC Med. 2014;12(1):157.
11. Magee LA, Pels A, Helewa M, Rey E, Dadelszen P. Diagnosis, evaluation, and management of the
hypertensive disorders of pregnancy: Executive summary. J Obstet Gynaecol Canada.
2014;36(5):416–38.
12. Locatelli CA, Vecchio S, Petrolini VM, Giampreti A, Lonati D, Manzo L. Alternative medicine and
toxicology: Are the risks well known? In: XXXIII International Congress of the European
Association of Poisons Centres and Clinical Toxicologists, (EAPCCT) 28-31 May 2013,
Copenhagen Denmark. Clin Toxicol. 2013;31(4):260–1.
13. Lausman A, Kingdom J. Intrauterine growth restriction: Screening, diagnosis, and management. J
Obstet Gynaecol Canada. 2013;35:741–8.
14. Government of Canada, Statistics Canada. Birth-related indicators (low and high birth weight,
small and large for gestational age, pre-term births), by sex, three-year period, health regions
and peer groups. Table 13-10-0745-01. Footnote 17. [Internet]. 2019 [cited 2022 Jun 16]. Available

Nutrition Guideline
Revised January 2024
Page 61
Pregnancy
from: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310074501
15. World Health Organization. Promoting optimal fetal development. Report of a technical
consultation. [Internet]. Geneva, Switzerland: WHO Document Production Services.; 2006.
Available from:
https://apps.who.int/iris/bitstream/handle/10665/43409/9241594004_eng.pdf?ua=1
16. World Health Organization. Managing complications in pregnancy and childbirth: a guide for
midwives and doctors - 2nd ed. [Internet] [Internet]. Geneva; 2017. Available from:
https://apps.who.int/iris/bitstream/handle/10665/255760/9789241565493-eng.pdf
17. Barfield WD. Standard Terminology for Fetal, Infant, and Perinatal Deaths. Pediatrics. 2016
May;137(5):e20160551.
18. Health Canada. Licensed Natural Health Products Database (LNHPD) [Internet]. 2007 [cited
2022 Jun 16]. Available from: https://www.canada.ca/en/health-canada/services/drugs-health-
products/natural-non-prescription/applications-submissions/product-licensing/licensed-
natural-health-products-database.html
19. Government of Canada, Statistics Canada. Infant deaths and mortality rates, by age group.
Table: 13-10-0712-01. Footnote 12. [Internet]. 2019 [cited 2022 Jun 16]. Available from:
https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310071301
20. Dietitians of Canada. Vegetarianism background. Phytate background in: Practice-based
evidence in nutrition [PEN]. [Internet]. 2012 [cited 2019 Aug 28]. Available from:
www.pennutrition.com Access only by subscription
21. Health Canada, Bureau of Nutritional Sciences, Food Directorate, Health Products and Food
Branch. Interim policy on the use of expired interim marketing authorizations related to food
fortification. 2022.
22. Dietitians of Canada. What lifestyle interventions can prevent the development of preeclampsia
in pregnancy? In: Practice-based Evidence in Nutrition [PEN]. [Internet]. 2017 [cited 2018 May
22]. Available from: www.pennutrition.com Access only by subscription
23. Hofmeyr GJ, Manyame S. Calcium supplementation commencing before or early in pregnancy, or
food fortification with calcium, for preventing hypertensive disorders of pregnancy. Cochrane
database Syst Rev. 2017;9:CD011192.
24. Dietitians of Canada. What are the risks associated with probiotic intake? In: Practice-based
Evidence in Nutrition [PEN]. [Internet]. 2010 [cited 2018 Oct 26]. Available from:
www.pennutrition.com Access only by subscription
25. Tea and Herbal Association of Canada. What is tea? [Internet]. 2018 [cited 2019 Aug 14].
Available from: https://www.tea.ca/learn/tea/what-is-tea/
26. Prager S, Micks E, Dalton V. Pregnancy loss (miscarriage): Terminology, risk factors, and
etiology [Internet]. 2022 [cited 2022 Jun 16]. Available from:
https://www.uptodate.com/contents/pregnancy-loss-miscarriage-terminology-risk-factors-and-
etiology
27. World Health Organization. Maternal, newborn, child and adolescent health. Stillbirths.
[Internet]. 2019 [cited 2022 Jun 16]. Available from: https://www.who.int/health-

Nutrition Guideline
Revised January 2024
Page 62
Pregnancy
topics/stillbirth#tab=tab_1
28. World Health Organization, UNICEF. Low birthweight. Country, regional and global estimates.
The United Nations Children’s Fund and World Health Organization; 2004.
29. Health Canada. The Canadian gestational weight gain recommendations. [Internet]. 2010 [cited
2022 Jun 16]. Available from: https://www.canada.ca/content/dam/hc-sc/migration/hc-sc/fn-
an/alt_formats/pdf/nutrition/prenatal/ewba-mbsa-eng.pdf
30. Dietitians of Canada. What is the recommended weight gain in pregnancy? In: Practice-based
Evidence in Nutrition [PEN] [Internet]. 2015 [cited 2017 Oct 20]. Available from:
www.pennutrition.com Access only by subscription
31. Jarman M, Mathe N, Ramazani F, Pakseresht M, Robson PJ, Johnson ST, et al. Dietary patterns
prior to pregnancy and associations with pregnancy complications. Nutrients.
2018;10(7):10.3390/nu10070914.
32. Institute of Medicine. Weight Gain During Pregnancy: Reexamining the Guidelines [Internet].
Rasmussen KM, Yaktine AL, editors. Washington (DC): National Academies Press (US); 2009.
Available from: http://www.ncbi.nlm.nih.gov/books/NBK32813/
33. Health Canada. Prenatal Nutrition Guidelines for Health Professionals - Background on
Canada’s Food Guide. [Internet]. 2009 [cited 2022 Jun 16]. Available from:
https://www.canada.ca/en/health-canada/services/publications/food-nutrition/prenatal-
nutrition-guidelines-health-professionals-background-canada-food-guide-2009.html
34. Health Canada. Dietary Reference Intake Tables [Internet]. 2010 [cited 2022 Jun 16]. Available
from: https://www.canada.ca/en/health-canada/services/food-nutrition/healthy-eating/dietary-
reference-intakes/tables.html
35. Institute of Medicine. Dietary reference intakes for calcium and vitamin D. Washington, DC:
National Academies Press; 2011.
36. Health Canada. Prenatal nutrition guidelines for health professionals - fish and omega-3 fatty
acids. [Internet]. 2009 [cited 2022 Jun 16]. Available from:
https://www.canada.ca/content/dam/hc-sc/migration/hc-sc/fn-an/alt_formats/hpfb-
dgpsa/pdf/pubs/omega3-eng.pdf
37. Health Canada. Prenatal Nutrition Guidelines for Health Professionals - Folate Contributes to a
Healthy Pregnancy [Internet]. 2009 [cited 2022 Jun 16]. Available from:
https://www.canada.ca/en/health-canada/services/food-nutrition/reports-publications/nutrition-
healthy-eating/prenatal-nutrition-guidelines-health-professionals-folate-contributes-healthy-
pregnancy-2009.html
38. Dietitians of Canada. What are the indications for the use of vitamin/mineral supplements during
pregnancy? Practice point #2 Folic Acid. In: Practice-based Evidence in Nutrition [PEN]
[Internet]. 2015 [cited 2018 Nov 13]. Available from: www.pennutrition.com Access only by
subscription
39. De-Regil LM, Peña-Rosas JP, Fernández-Gaxiola AC, Rayco-Solon P. Effects and safety of
periconceptional oral folate supplementation for preventing birth defects. Cochrane database
Syst Rev. 2015;(12):Art No.CD007950 DOI:10.1002/14651858.CD007950.pub3.

Nutrition Guideline
Revised January 2024
Page 63
Pregnancy
40. Wilson RD, O’Connor D. Guideline No. 427: Folic Acid and Multivitamin Supplementation for
Prevention of Folic Acid–Sensitive Congenital Anomalies. J Obstet Gynaecol Canada. 2022
Jun;44(6):707–19.
41. Health Canada. Canadian nutrient file [Internet]. 2015 [cited 2023 Oct 27]. Available from:
https://food-nutrition.canada.ca/cnf-fce/index-eng.jsp
42. Government of Canada. Percent daily value [Internet]. 2019 [cited 2022 Nov 28]. Available from:
https://www.canada.ca/en/health-canada/services/understanding-food-labels/percent-daily-
value.html
43. Health Canada. Eat well. Live well. Canada’s food guide. [Internet]. 2019 [cited 2022 Jun 16].
Available from: http://www.hc-sc.gc.ca/fn-an/food-guide-aliment/index-eng.php
44. Scientific Advisory Committee on Nutrition. SCAN Vitamin D and Health Report [Internet]. 2016
[cited 2022 Jun 16]. Available from: https://www.gov.uk/government/publications/sacn-vitamin-
d-and-health-report
45. Health Canada. Nutrition Labelling – Table of Reference Amounts for Food [Internet]. 2022
[cited 2023 Oct 27]. Available from: https://www.canada.ca/en/health-
canada/services/technical-documents-labelling-requirements/table-reference-amounts-
food/nutrition-labelling.html
46. World Health Organization. Guideline. Calcium supplementation in pregnant women. [Internet].
Geneva (Switzerland): World Health Organization (WHO); 2013. Available from:
https://apps.who.int/iris/bitstream/handle/10665/85120/9789241505376_eng.pdf?sequence=1
47. Dietitians of Canada. What type of calcium supplements are safe to take during pregnancy? In:
Practice-based Evidence in Nutrition [PEN] [Internet]. 2012 [cited 2001 Nov 13]. Available from:
www.pennutrition.com Access only by subscription
48. Institute of Medicine. Dietary Reference Intakes: The Essential Guide to Nutrient Requirements
[Internet]. Washington (DC): The National Academies Press; 2006. Available from:
https://www.nap.edu/read/11537/chapter/1
49. Government of Canada. Marketing Authorization for Vitamin D in Milk, Goat’s Milk and
Margarine. Canada Gazette, Part II [Internet]. 2021 [cited 2022 Nov 28];156(2). Available from:
https://www.gazette.gc.ca/rp-pr/p2/2022/2022-01-19/html/sor-dors278-eng.html
50. Government of Canada. Regulations Amending the Food and Drug Regulations (Nutrition
Symbols, Other Labelling Provisions, Vitamin D and Hydrogenated Fats or Oils). [Internet].
Canada Gazette, Part 2, Volume 156, Number 15. 2022. Available from:
https://www.gazette.gc.ca/rp-pr/p2/2022/2022-07-20/html/sor-dors168-eng.html
51. Health Canada, Bureau of Nutritional Sciences, Food Directorate, Health Products and Food
Branch. Notice of intent regarding the Minister of Health’s intention to publish marketing
authorizations to permit vitamin D fortification of yogurt and kefir and expand the eligibility for
the dairy-related exemption from the front-of-package nutrition labellin [Internet]. 2023.
Available from: https://www.canada.ca/en/health-canada/services/food-nutrition/public-
involvement-partnerships/notice-intent-marketing-authorizations-permit-vitamin-d-fortification-
yogurt-kefir-expand-eligibility-dairy-related-exemption-front-of-package-nutrition-labelli

Nutrition Guideline
Revised January 2024
Page 64
Pregnancy
52. Institutes of Medicine. Dietary reference intakes for vitamin A, vitamin K, arsenic, boron,
chromium, copper, iodine, iron, manganese, molybdenum, nickel, silicon, vanadium, and zinc
[Internet]. Vol. 101. Washington, DC: National Academy Press; 2001. 294–301 p. Available from:
https://www.sciencedirect.com/science/article/pii/S0002822301000785
53. Ahankari A L-BJ. Maternal hemoglobin and birth weight: systematic review and meta-analysis.
Int J Med Sci Public Heal. 2015;4(4).
54. Sukrat B, Wilasrusmee C, Siribumrungwong B, McEvoy M, Okascharoen C, Attia J, et al.
Hemoglobin concentration and pregnancy outcomes: A systematic review and meta-analysis.
Biomed Res Int [Internet]. 2013;2013:769057–9. Available from:
http://dx.doi.org/10.1155/2013/769057
55. Health Canada. Prenatal Nutrition Guidelines for Health Professionals - Iron Contributes to a
Healthy Pregnancy [Internet]. 2009 [cited 2022 Jun 16]. Available from:
https://www.canada.ca/en/health-canada/services/food-nutrition/reports-publications/nutrition-
healthy-eating/prenatal-nutrition-guidelines-health-professionals-iron-contributes-healthy-
pregnancy-2009.html
56. Gupta RK, Gangoliya SS, Singh NK. Reduction of phytic acid and enhancement of bioavailable
micronutrients in food grains. J Food Sci Technol. 2015 Feb;52(2):676–84.
57. Dietitians of Canada. What is recommended for managing or treating iron deficiency or iron-
deficiency anemia among non-pregnant adults? In: Practice-based Evidence in Nutrition [PEN]
[Internet]. 2016 [cited 2019 Aug 14]. Available from: www.pennutrition.com Access only by
subscription
58. Cunningham E. Methylmercury and seafood: what are the latest guidelines? J Acad Nutr Diet.
2017;117(5):824.
59. Imhoff‐Kunsch B, Briggs V, Goldenberg T, Ramakrishnan U. Effect of n‐3 long‐chain
polyunsaturated fatty acid intake during pregnancy on maternal, infant, and child health
outcomes: a systematic review. Paediatr Perinat Epidemiol. 2012 Jul;26:91–107.
60. National Institute of Health. Omega 3 fatty acids: fact sheet for health professionals. [Internet].
Vol. 2018. 2018 [cited 2022 Jun 16]. Available from:
https://ods.od.nih.gov/factsheets/Omega3FattyAcids-HealthProfessional/
61. Dietitians of Canada. Is there evidence to support a benefit for taking omega-3 fatty acid
supplements during pregnancy? In: Practice-based Evidence in Nutrition [PEN]. [Internet]. 2017
[cited 2018 Nov 26]. Available from: www.pennutrition.com Access only by subscription
62. American Dietetic Association. Position of the American Dietetic Association and Dietitians of
Canada: dietary fatty acids. J Am Diet Assoc. 2007;107:1599–611.
63. Burnbrae Farms. Naturegg Omega 3 [Internet]. 2017 [cited 2022 Jun 16]. Available from:
https://www.burnbraefarms.com/en/products/shelled-eggs
64. Burnbrae Farms. Naturegg Omega Plus [Internet]. 2017 [cited 2022 Jun 16]. Available from:
https://www.burnbraefarms.com/en/products/shelled-eggs
65. Institute of Medicine. Dietary reference intakes for thiamin, riboflavin, niacin, vitamin B6, folate,
vitamin B12, pantothenic acid, biotin, and choline. Washington, DC: National Academies Press;

Nutrition Guideline
Revised January 2024
Page 65
Pregnancy
1998.
66. Dietitians of Canada. What effects does dietary choline intake outside of the AI have on the
healthy population? In: Practice-based Evidence in Nutrition [PEN]. [Internet]. 2014 [cited 2018
Mar 18]. Available from: www.pennutrition.com Access only by subscription
67. Lewis ED, Subhan FB, Bell RC, McCargar LJ, Curtis JM, Jacobs RL, et al. Estimation of choline
intake from 24 h dietary intake recalls and contribution of egg and milk consumption to intake
among pregnant and lactating women in Alberta. Br J Nutr. 2014 Jul 14;112(1):112–21.
68. Masih SP, Plumptre L, Ly A, Berger H, Lausman AY, Croxford R, et al. Pregnant Canadian women
achieve recommended intakes of one-carbon nutrients through prenatal supplementation but
the supplement composition, including choline, requires reconsideration. J Nutr. 2015
Aug;145(8):1824–34.
69. Government of Canada, Statistics Canada. Fact sheets. Iodine status of Canadians, 2009 to 2011.
[Internet]. 2013 [cited 2022 Jun 16]. Available from: https://www150.statcan.gc.ca/n1/pub/82-
625-x/2012001/article/11733-eng.htm
70. Perrine CG, Herrick K, Serdula MK, Sullivan KM. Some Subgroups of Reproductive Age Women
in the United States May Be at Risk for Iodine Deficiency. J Nutr. 2010;140(8):1489–94.
71. Academy of Nutrition and Dietetics. Position of the Academy of Nutrition and Dietetics:
Vegetarian diets. J Acad Nutr Diet. 2016;116(12):1970–80.
72. Dietitians of Canada. Do vegetarians need to take a supplement in order to meet
recommendations for iron and/or vitamin B12 intake? In: Practice-based Evidence in Nutrition
[PEN]. [Internet]. 2012 [cited 2018 May 29]. Available from: www.pennutrition.com Access only by
subscription
73. Institute of Medicine. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids,
cholesterol, protein, and amino acids. Washington, DC: National Academies Press; 2005.
74. Papaioannou A, Morin S, Cheung AM, Atkinson S, Brown JP, Feldman S, et al. 2010 clinical
practice guidelines for the diagnosis and management of osteoporosis in Canada: summary. C
Can Med Assoc J = J l’Association medicale Can. 2010;182(17):1864–73.
75. Dietitians of Canada. Are the Adequate Intakes (AIs) for alpha linolenic acid (ALA) adequate for
vegetarian (lacto-ovo, lacto, and vegan) women who are pregnant and breastfeeding? [Internet].
2012. Available from: www.pennutrition.com Access only by subscription.
76. Shah PS, Ohlsson A, Births KSG on D of LBW and P. Effects of prenatal multimicronutrient
supplementation on pregnancy outcomes: a meta-analysis. C Can Med Assoc J. 2009 Jun
9;180(12):99.
77. Haider BA, Bhutta ZA. Multiple-micronutrient supplementation for women during pregnancy.
Cochrane Database Syst Rev. 2017;Issue 4.
78. Zerfu TA, Ayele HT. Micronutrients and pregnancy; effect of supplementation on pregnancy and
pregnancy outcomes: a systematic review. Nutr J. 2013;12(1):20.
79. Haider BA, Yakoob MY, Bhutta ZA. Effect of multiple micronutrient supplementation during
pregnancy on maternal and birth outcomes. BMC Public Health. 2011 Apr 13;11(Suppl 3):S19–S19.

Nutrition Guideline
Revised January 2024
Page 66
Pregnancy
80. Cooper M, Greene-Finestone L, Lowell H, Levesque J, Robinson S. Iron sufficiency of Canadians.
Stat Canada, Heal Reports. 2012;23(4):41–8.
81. World Health Organization. The global prevalence of anaemia in 2011 [Internet]. World Health
Organization; 2015. Available from: http://www.who.int/iris/handle/10665/177094
82. Rappaport AI, Whitfield KC, Chapman GE, Yada RY, Kheang KM, Louise J, et al. Randomized
controlled trial assessing the efficacy of a reusable fish-shaped iron ingot to increase
hemoglobin concentration in anemic, rural Cambodian women. Am J Clin Nutr. 2017
Aug;106(2):667–74.
83. Dietitians of Canada. Should omega-3 fatty acids (fish or plant-based food or supplements) be
recommended for primary or secondary prevention of cardiovascular disease in adults? In:
Practice-based Evidence in Nutrition [PEN]. [Internet]. 2019 [cited 2019 Feb 26]. Available from:
www.pennutrition.com Access only by subscription
84. Saccone G, Berghella V. Omega-3 long chain polyunsaturated fatty acids to prevent preterm
birth: a systematic review and meta-analysis. Obstet Gynecol. 2015 Mar;125(3):663–72.
85. Chen B Zhang L, Hou Z, Li C, Tong Y. JX. Fish oil supplementation improves pregnancy outcomes
and size of the newborn: A meta-analysis of 21 randomized controlled trials. . J Matern Neonatal
Med. 2016;29(12):2017–27.
86. Saccone G, Berghella V, Maruotti GM, Sarno L, Martinelli P. Omega‐3 supplementation during
pregnancy to prevent recurrent intrauterine growth restriction: systematic review and meta‐
analysis of randomized controlled trials. Ultrasound Obstet Gynecol. 2015 Dec;46(6):659–64.
87. Saccone G, Saccone I, Berghella V. Omega-3 long-chain polyunsaturated fatty acids and fish oil
supplementation during pregnancy: which evidence? J Matern Fetal Neonatal Med.
2016;29(15):2389.
88. Gould JF, Smithers LG, Makrides M. The effect of maternal omega-3 (n-3) LCPUFA
supplementation during pregnancy on early childhood cognitive and visual development: a
systematic review and meta-analysis of randomized controlled trials. Am J Clin Nutr. 2013
Mar;97(3):531–44.
89. Therapeutic Research Center, Natural Medicines. Foods, herbs and supplements-professional.
Fish oil. [Internet]. 2018 [cited 2022 Jun 16]. Available from:
https://naturalmedicines.therapeuticresearch.com/databases/food,-herbs-
supplements/professional.aspx?productid=993
90. Dietitians of Canada. What sources of DHA and EPA are acceptable to vegetarians? In: Practice-
based Evidence in Nutrition [PEN] [Internet]. 2014 [cited 2018 Nov 26]. Available from:
www.pennutrition.com Access only by subscription
91. Therapeutic Research Center, Natural Medicines. Foods, herbs and supplements-professional.
Flaxseed. [Internet]. 2018 [cited 2022 Jun 16]. Available from:
https://naturalmedicines.therapeuticresearch.com/databases/food,-herbs-
supplements/professional.aspx?productid=991
92. Therapeutic Research Center, Natural Medicines. Foods, herbs and supplements-professional.
Flaxseed oil. [Internet]. 2018 [cited 2022 Jun 16]. Available from:

Nutrition Guideline
Revised January 2024
Page 67
Pregnancy
https://naturalmedicines.therapeuticresearch.com/databases/food,-herbs-
supplements/professional.aspx?productid=990
93. Therapeutic Research Center, Natural Medicines. Food, herbs and supplements-professional.
Krill oil. [Internet]. 2018 [cited 2022 Jun 16]. Available from:
https://naturalmedicines.therapeuticresearch.com/databases/food,-herbs-
supplements/professional.aspx?productid=1172
94. Dietitians of Canada. Are there adverse effects of high protein diets (including protein powder
supplements) in pregnant and lactating women? In: Practice-based Evidence in Nutrition [PEN].
[Internet]. 2012 [cited 2018 Nov 29]. Available from: www.pennutrition.com Access only by
subscription
95. Dietitians of Canada. Is soy safe to take during pregnancy or the preconception period? In:
Practice-based Evidence in Nutrition [PEN]. [Internet]. 2012 [cited 2018 May 29]. Available from:
www.pennutrition.com Access only by subscription
96. Dietitians of Canada. Are vitamin A supplements (including cod/fish liver oil supplements) and
other rich food sources of vitamin A, such as liver, safe to consume in any amount during
pregnancy? In: Practice-based Evidence in Nutrition [PEN]. [Internet]. 2012 [cited 2018 Nov 30].
Available from: www.pennutrition.com Access only by subscription
97. Lott M, Callahan E, Duffy EW, Story M, Daniels S. Healthy Beverage Consumption in Early
Childhood: Recommendation from Key National Health and Nutrition Organizations Consensus
Statement. Durham, NC: Heal Eat Res [Internet]. 2019;(September):1–13. Available from:
http://healthyeatingresearch.org
98. Health Canada. Caffeine in foods [Internet]. 2012 [cited 2022 Jun 16]. Available from:
https://www.canada.ca/en/health-canada/services/food-nutrition/food-safety/food-
additives/caffeine-foods/foods.html
99. Health Canada. Health Canada is advising Canadians about safe levels of caffeine consumption.
[Internet]. 2017 [cited 2022 Jun 16]. Available from: http://healthycanadians.gc.ca/recall-alert-
rappel-avis/hc-sc/2017/63362a-eng.php
100. Chen L-W, Wu Y, Neelakantan N, Chong MF, Pan A, van Dam RM. Maternal caffeine intake during
pregnancy is associated with risk of low birth weight: a systematic review and dose-response
meta-analysis. BMC Med. 2014;12:174.
101. Greenwood DC, Thatcher NJ, Ye J, Garrard L, Keogh G, King LG, et al. Caffeine intake during
pregnancy and adverse birth outcomes: a systematic review and dose-response meta-analysis.
Eur J Epidemiol. 2014 Oct;29(10):725–34.
102. Dietitians of Canada. What is the impact of caffeine intake in pregnancy and lactation? In:
Practice-based Evidence in Nutrition [PEN]. [Internet]. 2017 [cited 2019 Feb 26]. Available from:
www.pennutrition.com Access only by subscription
103. Thorlton J. Energy drinks: Implications for the breastfeeding mother. MCN, Am J Matern child
Nurs. 2016;41(3):1–6.
104. NOS Energy Company. NOS Flavors. Performance Energy Drinks [Internet]. 2018 [cited 2018 Jan
26]. Available from: https://www.drinknos.com/products#/16oz-Rowdy

Nutrition Guideline
Revised January 2024
Page 68
Pregnancy
105. National Center for Complementary and Integrative Health. Energy Drinks | NCCIH [Internet].
2018 [cited 2022 Jun 10]. Available from: https://www.nccih.nih.gov/health/energy-drinks
106. LLC Energy Beverages. Full throttle energy drink [Internet]. 2017 [cited 2018 Jan 26]. Available
from: https://www.drinkfullthrottle.com/en-us/
107. Pepsico. The Facts About Your Favorite Beverages (U.S.). Rockstar Originial Sugar Free.
[Internet]. [cited 2022 Jun 15]. Available from:
https://www.pepsicobeveragefacts.com/Home/Product?formula=BACX509&form=RTD&size=16
108. Pepsico. The Facts About Your Favorite Beverages (U.S.) | Caffeine [Internet]. [cited 2022 Jun 15].
Available from: https://www.pepsicobeveragefacts.com/home/caffeine
109. Dietitians of Canada. The Juicy Story on Drinks [Internet]. 2018 [cited 2018 Dec 13]. Available
from: www.pennutrition.com Access only by subscription
110. Government of Canada. Sugary drinks and your teen. [Internet]. 2019 [cited 2019 Aug 14].
Available from: https://food-guide.canada.ca/en/healthy-eating-recommendations/make-water-
your-drink-of-choice/sugary-drinks/sugary-drinks-and-your-teen/
111. Dietitians of Canada. What herbal beverages/supplements are safe to take during pregnancy
and lactation? In: Practice-based Evidence in Nutrition [PEN]. [Internet]. 2012. Available from:
www.pennutrition.com Access only by subscription.
112. Viljoen E, Visser J, Koen N, Musekiwa A. A systematic review and meta-analysis of the effect and
safety of ginger in the treatment of pregnancy-associated nausea and vomiting. Nutr J.
2014;13(1):20.
113. Matthews A, Haas DM, O’Mathúna DP, Dowswell T. Interventions for nausea and vomiting in
early pregnancy. Cochrane database Syst Rev. 2015;(9):CD007575.
114. Moussally K, Berard A. Exposure to specific herbal products during pregnancy and the risk of
low birth weight. Altern Ther Health Med. 2012 Mar;18(2):36.
115. Therapeutic Research Center, Natural Medicines. Foods, herbs and supplements-professional.
Peppermint. [Internet]. 2019 [cited 2022 Jun 16]. Available from:
https://naturalmedicines.therapeuticresearch.com/databases/food,-herbs-
supplements/professional.aspx?productid=705
116. Therapeutic Research Center, Natural Medicines. Foods, herbs and supplements-professional.
Rose hip. [Internet]. 2018 [cited 2022 Jun 16]. Available from:
https://naturalmedicines.therapeuticresearch.com/databases/food,-herbs-
supplements/professional.aspx?productid=839
117. Abbott. SimilacR Mom [Internet]. 2018 [cited 2019 Mar 25]. Available from:
https://similac.ca/en/products/similac-mom-drink
118. Health Canada. Food safety for pregnant women. [Internet]. 2016 [cited 2022 Jun 16]. Available
from: https://www.canada.ca/en/health-canada/services/food-safety-vulnerable-
populations/food-safety-pregnant-women.html
119. Dietitians of Canada. Are pregnant women more at risk for serious health outcomes when
exposed to foodborne pathogens than non-pregnant women or men? If so, what steps should be
Nutrition Guideline
Revised January 2024
Page 69
Pregnancy
taken to reduce the risk of foodborne illness? In: Practice-based Evidence in Nutrition [PEN].
[Internet]. 2014 [cited 2018 Jun 22]. Available from: www.pennutrition.com Access only by
subscription
120. Heymann D, Editor. Control of communicable diseases manual. 10th Edition. Washington D.C.:
APHA Press; 2015.
121. Health Canada. General food safety tips: food safety and you. [Internet]. 2014 [cited 2022 Jun
16]. Available from: https://www.canada.ca/en/health-canada/services/general-food-safety-
tips/food-safety-you.html
122. Health Canada. Public Health Notice - Outbreak of E. coli infections linked to various flours and
flour products. [Internet]. 2017 [cited 2022 Jun 16]. Available from:
https://www.canada.ca/en/public-health/services/public-health-notices/2017/public-health-
notice-outbreak-e-coli-infections-linked-various-flours-flour-products.html
123. Health Canada. Mercury in fish consumption advice: making informed choices about fish.
[Internet]. 2017 [cited 2022 Jun 16]. Available from: https://www.canada.ca/en/health-
canada/services/food-nutrition/food-safety/chemical-contaminants/environmental-
contaminants/mercury/mercury-fish.html
124. Mergler D Hing Man Chan L, Mahaffey KR, Murray M, Sakamoto M, Stern AH. AHA.
Methylmercury exposure and health effects in humans: a worldwide concern. Ambio.
2007;36(1):3–11.
125. Government of Alberta. Should I eat this fish? [Internet]. 2018 [cited 2022 Jun 16]. Available from:
https://itunes.apple.com/us/app/should-i-eat-this-fish/id1119021760?mt=8
126. Health Canada. Policy on Listeria Monocytogenes in Ready to Eat (RTE) foods (2011). [Internet].
2015 [cited 2022 Jun 16]. Available from: https://www.canada.ca/en/health-
canada/services/food-nutrition/legislation-guidelines/policies/policy-listeria-monocytogenes-
ready-eat-foods-2011.html#appb
127. Health Canada, US Department of Health and Human Services. Join FDA/Health Canada
quantitative assessment of the risk of Listeriosis from soft-ripened cheese consumption in the
United States and Canada: draft interpretive summary. [Internet]. 2012 [cited 2022 Jun 16].
Available from: https://www.fda.gov/downloads/Food/FoodScienceResearch/UCM338618.pdf
128. Government of Canada. Food and Drug Regulations: Division 8 Cheese. [Internet]. 2019. Available
from: https://laws-lois.justice.gc.ca/PDF/C.R.C.,_c._870.pdf
129. Health Canada. General food safety tips: safe internal cooking temperatures. [Internet]. 2014
[cited 2022 Jun 16]. Available from: https://www.canada.ca/en/health-canada/services/general-
food-safety-tips/safe-internal-cooking-temperatures.html
130. Government of Canada. Canadian Dairy Information Centre: Glossary for the classification of
cheeses. [Internet]. 2017 [cited 2022 Jun 16]. Available from: http://cheese-
fromage.agr.gc.ca/glossary-lexique_eng.cfm?menupos=1.4
131. World Health Organization. Fact Sheets. Arsenic [Internet]. 2018 [cited 2021 Jul 8]. Available
from: https://www.who.int/en/news-room/fact-sheets/detail/arsenic
132. Health Canada. Food and nutrition. Arsenic. [Internet]. 2017 [cited 2022 Jun 16]. Available from:

Nutrition Guideline
Revised January 2024
Page 70
Pregnancy
https://www.canada.ca/en/health-canada/services/food-nutrition/food-safety/chemical-
contaminants/environmental-contaminants/arsenic.html
133. Sanchez TR, Perzanowski M, Graziano JH. Inorganic arsenic and respiratory health, from early
life exposure to sex-specific effects: A systematic review. Environ Res. 2016;147:537–55.
134. Quansah R, Armah FA, Essumang DK, Luginaah I, Clarke E, Marfoh K, et al. Association of arsenic
with adverse pregnancy outcomes/infant mortality: A systematic review and meta-analysis.
Environ Health Perspect. 2015;123(5):412–21.
135. Dietitians of Canada. Trending Topic: Do new parents or parents-to-be need to be concerned
about dietary arsenic exposure? 2018; Available from: www.pennutrition.com Access only by
subscription
136. Tam C, Erebara A, Einarson A. Food-borne illnesses during pregnancy: Prevention and treatment.
Can Fam Physician. 2010;56(4):341–3.
137. Grabowski NT KG. Microbiology and foodborne pathogens in honey. Crit Rev Food Sci Nutr
[Inernet]. 2017;57(9):1852–62.
138. World Health Organization. Fact sheets. Botulism. [Internet]. 2018 [cited 2022 Jun 16]. Available
from: https://www.who.int/en/news-room/fact-sheets/detail/botulism
139. Hatheway CL. Toxigenic clostridia. Clin Microbiol Rev. 1990;3(1):66–98.
140. Lund BM, O’Brien SJ. The occurrence and prevention of foodborne disease in vulnerable people.
Foodborne Pathog Dis [Internet]. 2011;8(9):961–73.
141. Fenicia L Aureli P. AF. Intestinal toxemia botulism in Italy, 1984-2005. Eur J Clin Microbiol Infect
Dis. 2007;26(6):385–94.
142. Health Canada, Canadian Pediatric Society, Dietitians of Canada, Breastfeeding Committee for
Canada. Nutrition for Healthy Term Infants: Recommendations from Six to 24 Months [Internet].
2014 [cited 2022 Jun 16]. Available from: https://www.canada.ca/en/health-
canada/services/canada-food-guide/resources/infant-feeding/nutrition-healthy-term-infants-
recommendations-birth-six-months/6-24-months.html
143. MyHealth.Alberta.ca. Healthy Parents, Healthy Children | Eating & Food Safety During
Pregnancy [Internet]. 2019. Available from: https://www.healthyparentshealthychildren.ca/im-
pregnant/overview-of-pregnancy/eating-food-safety/#iron
144. Health Canada. Questions and answers on probiotics [Internet]. 2009 [cited 2022 Jun 16].
Available from: https://www.canada.ca/en/health-canada/services/food-nutrition/food-
labelling/health-claims/questions-answers-probiotics.html
145. Kole AS Christensen R, Gladstein J. JHD. A case of Kombucha tea toxicity. J Intensive Care Med.
2009;24(3):205–7.
146. Watawana MI, Jayawardena N, Gunawardhana CB, Waisundara VY. Health, wellness, and safety
aspects of the consumption of Kombucha. J Chem. 2015;2015:1–11.
147. Therapeutic Research Center, Natural Medicines. Food, herbs and supplements-professional.
Kombucha tea. [Internet]. 2019 [cited 2022 Jun 16]. Available from:
https://naturalmedicines.therapeuticresearch.com/databases/food,-herbs-

Nutrition Guideline
Revised January 2024
Page 71
Pregnancy
supplements/professional.aspx?productid=538
148. Dugoua J Zhu X, Chen X, Koren G, Einarson T MM. Probiotic safety in pregnancy: A systematic
review and meta-analysis of randomized controlled trials of Lactobacillus, Bifidobacterium and
Saccharomyces. J Obstet Gynaecol Canada. 2009;31(6):542–52.
149. Health Canada. The Safety of Sugar Substitutes [Internet]. 2008 [cited 2022 Jun 16]. Available
from: https://www.canada.ca/en/health-canada/services/healthy-living/your-health/food-
nutrition/safety-sugar-substitutes.html
150. Health Canada. Sugar substitutes [Internet]. 2010. Available from:
https://www.canada.ca/en/health-canada/services/food-nutrition/food-safety/food-
additives/sugar-substitutes.html
151. Health Canada. List of permitted sweeteners (lists of permitted food additives) [Internet]. 2017
[cited 2022 Jun 16]. Available from: https://www.canada.ca/en/health-canada/services/food-
nutrition/food-safety/food-additives/lists-permitted/9-sweeteners.html
152. Diabetes Canada. Sugar and sweeteners [Internet]. 2018. Available from:
http://guidelines.diabetes.ca/docs/patient-resources/sugars-and-sweeteners.pdf
153. Therapeutic Research Center, Natural Medicines. Foods, herbs and supplements-professional.
Stevia. [Internet]. 2019 [cited 2022 Jun 16]. Available from:
https://naturalmedicines.therapeuticresearch.com/databases/food,-herbs-
supplements/professional.aspx?productid=682
154. Dietitians of Canada. Are there any specific considerations with regard to the use of sugar
alcohols as sweeteners in pregnancy/lactation? In: Practice-based Evidence in Nutrition [PEN]
[Internet]. 2013. Available from: www.pennutrition.com Access only by subscription
155. Health Canada. Sugar Alcohols (Polyols) and Polydextrose Used as Sweeteners in Foods - Food
Safety - Health Canada - Canada.ca [Internet]. 2015 [cited 2020 Nov 6]. Available from:
https://www.canada.ca/en/health-canada/services/food-nutrition/food-safety/food-
additives/sugar-substitutes/sugar-alcohols-polyols-polydextrose-used-sweeteners-foods-food-
safety.html
156. Campbell K, Rowe H, Azzam H, Lane CA. The Management of Nausea and Vomiting of
Pregnancy. J Obstet Gynaecol Canada. 2016;38(12):1127–37.
157. Einarson A, Maltepe C, Boskovic R, Koren G. Treatment of nausea and vomiting in pregnancy: An
updated algorithm. Can Fam Physician. 2007;53(12):2109–11.
158. Hunter LP, Sullivan CA, Young RE, Weber CE. Nausea and vomiting of pregnancy: clinical
management. Am J Nurse Pr. 2007;11(8):57–67.
159. Jewell DJ, Young G. Interventions for treating constipation in pregnancy. Cochrane database
Syst Rev [Internet]. 2001;(2):CD001142. Available from:
https://pubmed.ncbi.nlm.nih.gov/11405974/
160. Phupong V, Hanprasertpong T. Interventions for heartburn in pregnancy. Cochrane database
Syst Rev [Internet]. 2015;(9):CD011379. Available from:
https://pubmed.ncbi.nlm.nih.gov/26384956/

Nutrition Guideline
Revised January 2024
Page 72
Pregnancy
161. The American College of Obstetrics and Gynecologists. Frequently asked questions. FAQ 2012
women’s health. [Internet]. 2014 [cited 2022 Jun 16]. Available from:
https://www.acog.org/Patients/FAQs/Problems-of-the-Digestive-System
162. Public Health Agency of Canada. The sensible guide to a healthy pregnancy. Heartburn.
[Internet]. 2019 [cited 2022 Jun 16]. Available from: https://www.canada.ca/en/public-
health/services/health-promotion/healthy-pregnancy/healthy-pregnancy-guide.html
163. Feig DS, Berger H, Donovan L, Godbout A, Kader T, Keely E, et al. Diabetes Canada 2018 Clinical
Practice Guidelines for the Prevention and Management of Diabetes in Canada: Diabetes and
Pregnancy. Can J Diabetes. 2018;42(Suppl 1):S255–82.
164. Dietitians of Canada. What are nutrition recommendations for pregnant women with pre-existing
moderate or severe hypertension? Is sodium restriction advisable? In: Practice-based Evidence
in Nutrition [PEN]. [Internet]. 2016 [cited 2018 Jul 24]. Available from: www.pennutrition.com
Access only by subscription
165. Dietitians of Canada. Do infants with a parental history of allergy have a reduced incidence of
allergy if their mothers avoid common allergenic foods during pregnancy as compared to infants
of mothers who do not restrict their diets during pregnancy? In: Practice-based Eviden [Internet].
2009 [cited 2018 Jun 12]. Available from: www.pennutrition.com Access only by subscription
166. de Silva D, Geromi M, Halken S, Host A, Panesar SS, Muraro A, et al. Primary prevention of food
allergy in children and adults: systematic review. Allergy - Eur J Allergy Clin Immunol. 2014
May;69(5):581–9.
167. Sicherer SH, Sampson HA. Food allergy: A review and update on epidemiology, pathogenesis,
diagnosis, prevention, and management. J Allergy Clin Immunol. 2018 Jan;141(1):41–58.
168. Pali-Schöll I, Namazy J, Jensen-Jarolim E. Allergic diseases and asthma in pregnancy, a
secondary publication. World Allergy Organ J. 2017;10(1):10.
169. Simons FER, Ebisawa M, Sanchez-Borges M, Thong BY, Worm M, Tanno LK, et al. 2015 update of
the evidence base: World Allergy Organization anaphylaxis guidelines. World Allergy Organ J.
2015;8(1):32.
170. Fleming N, O’Driscoll T, Becker G, Spitzer RF. Adolescent pregnancy guidelines. J Obstet
Gynaecol Canada. 2015;37(8):740–56.
171. Moran VH. A systematic review of dietary assessments of pregnant adolescents in industrialised
countries. Br J Nutr. 2007;97(3):411–25.
172. Bushnik T. The health of girls and women in Canada. [Internet]. Canadian Research Index. Ann
Arbor: ProQuest Micromedia; 2016. Available from: https://www150.statcan.gc.ca/n1/pub/89-
503-x/2015001/article/14324-eng.htm
173. Health Canada. Do Canadian adolescents meet their nutrient requirements through food intake
alone? [Internet]. 2012 [cited 2022 Jun 16]. Available from: https://www.canada.ca/en/health-
canada/services/food-nutrition/food-nutrition-surveillance/health-nutrition-surveys/canadian-
community-health-survey-cchs/canadian-adolescents-meet-their-nutrient-requirements-
through-food-intake-alone-health-canada-2012.ht
174. Salam RA, Hooda M, Das JK, Arshad A, Lassi ZS, Middleton P, et al. Interventions to Improve

Nutrition Guideline
Revised January 2024
Page 73
Pregnancy
Adolescent Nutrition: A Systematic Review and Meta-Analysis. J Adolesc Heal. 2016;59(4S):29–
39.
175. Carson G, Cox LV, Crane J, Croteau P, Graves L, Kluka S, et al. Alcohol use and pregnancy
clinical guidelines. J Obstet Gynaecol Can. 2017;39(9):e255–92.
176. Butt P, Beirness D, Gliksman L, Paradis C, Stockwell T. Alcohol and health in Canada: a summary
of evidence and guidelines for low-risk drinking. Ottawa, ON: Canadian Centre on Substance
Abuse; 2011. 66 pages.
177. Dietitians of Canada. Is any amount of alcohol safe to consume during pregnancy? In: Practice-
based Evidence in Nutrition [PEN]. [Internet]. 2013 [cited 2018 Jul 23]. Available from:
www.pennutrition.com Access only by subscription
178. Public Health Agency of Canada. Research update: Alcohol use and pregnancy: An important
Canadian public health and social issue. Ottawa, Canada: Public Health Agency of Canada; 2006.
179. Porath AJ, Kent P, Konefal S. Canadian Centre on Substance Abuse. Clearing the Smoke on
Cannabis: Maternal Cannabis Use during Pregnancy - An Update [Internet]. Clearing the Smoke
on Cannabis. Canadian Centre on Substance Abuse; 2018 [cited 2022 Jun 16]. Available from:
https://publications.gc.ca/site/eng/9.864008/publication.html
180. Alberta Health Services. Cannabis & Pregnancy/Breastfeeding [Internet]. [cited 2022 Jun 16].
Available from: https://www.albertahealthservices.ca/info/Page17998.aspx
181. Muktabhant B, Lawrie TA, Lumbiganon P, Laopaiboon M. Diet or exercise, or both, for preventing
excessive weight gain in pregnancy. Cochrane Database Syst Rev. 2015 Jun 15;(6):CD007145.
182. Mudd LM, Owe KM, Mottola MF, Pivarnik JM. Health benefits of physical activity during
pregnancy: an international perspective. Med Sci Sport Exerc. 2013;45(2):268–77.
183. Mottola MF, Davenport M, Ruchat S, Davies G, Poitras V, Gray D. 2019 Canadian Guideline for
Physical Activity throughout Pregnancy. Journal of Obstetrics and Gynaecology Canada. 2018.
184. Tarasuk V, Mitchell A. Household food insecurity in Canada, 2017-18 [Internet]. Toronto:
Research to identify policy options to reduce food insecurity (PROOF); 2020. Available from:
https://proof.utoronto.ca/
185. Men F, Gundersen C, Urquia ML, Tarasuk V. Food insecurity is associated with higher health care
use and costs among canadian adults. Health Aff. 2020;39(8):1377–85.
186. Alberta Health Services. Household food insecurity evidence review: Lived experience and
strategy effectiveness [Internet]. 2020. Available from:
https://albertahealthservices.ca/assets/info/nutrition/if-nfs-pph-evrev-fullreport-household-
food-insecurity.pdf
187. Ontario Dietitians in Public Health. Position statement and recommendations on responses to
food insecurity [Internet]. 2020. Available from: odph.ca.
188. Huisken A, Orr SK, Tarasuk V. Adults’ food skills and use of gardens are not associated with
household food insecurity in Canada. Can J Public Heal. 2016;107(6):e526–32.
189. Loopstra R, Tarasuk V. The relationship between food banks and household food insecurity
among low-income Toronto Families. Can Public Policy. 2012;38(4):497–514.

Nutrition Guideline
Revised January 2024
Page 74
Pregnancy
190. Andermann A. Taking action on the social determinants of health in clinical practice: A
framework for health professionals. Cmaj. 2016;188(17–18):E474–83.
191. Sivakumar G, Chau B. Poverty: A clinical instrument for family physicians. Univ West Ont Med J.
2017 Dec 3;86(2):62–4.
