
Making Progress on HPV Vaccination
in New York State
March 2022

Contents
1 Executive Summary
3 Key Findings
5 HPV Vaccination Coverage in NY
6 Overall
7
B
y Gender
8 By Race/Ethnicity
10
B
y Geographic Area
13 Discussion
19 Conclusion
20 Methods
22 Limitations
24 Appendix

Executive Summary
The development of coronavirus vaccines has generated renewed interest in the power
of vaccination to improve population health. With the recent emergency approval of the
COVID-19 vaccine for children ages 5 and up, governments, schools, and other groups
are taking steps to ensure that children are immunized. This is a unique moment to assess
childhood vaccination coverage and policies for other vaccine-preventable diseases,
including the human papillomavirus (HPV).
HPV is a common virus spread through sexual contact. Nearly 43 million Americans have HPV,
making it the single most common sexually transmitted infection.
1
HPV can cause six types of
cancers, including cervical cancer.
2
From 2013 to 2017, an average of 2,730 New Yorkers were
diagnosed with an HPV-related cancer each year, with about 60% of cases among women
and 40% among men.
3
The HPV vaccine prevents the development of more than 90% of
these cancers, making it one of only two vaccines that prevent cancer.
4,5
The HPV vaccine is
administered to adolescents so they are fully protected against the virus before ever being
exposed to it. The Centers for Disease Control and Prevention recommends that adolescents
receive two doses of the HPV vaccine when they are ages 11–12 years.
6
This report examines HPV vaccination coverage in New York State from 2018 to 2020.
Vaccination coverage refers to the percentage of 13-year-olds who completed the two-
dose HPV vaccine series by the age of 13 years. Data on adolescent vaccination were made
available through the New York State Immunization Information System (see more details
1
Centers for Disease Control and Prevention, “Sexually Transmitted Infections Prevalence, Incidence, and Cost Estimates
in the United States,” Centers for Disease Control and Prevention, January 25, 2021, https://www.cdc.gov/std/statistics/
prevalence-2020-at-a-glance.htm.
2
Centers for Disease Control and Prevention, “Cancers Caused by HPV,” July 23, 2021, https://www.cdc.gov/hpv/parents/
cancer.html.
3
New York State Department of Health, “HPV-Related Cancer Incidence and HPV Vaccination Rates in New York State,
2013-2017,” https://www.health.ny.gov/statistics/cancer/docs/hpv_related_cancer_13-17.pdf.
4
Centers for Disease Control and Prevention, “Cancers Caused by HPV are Preventable,” September 2020, https://www.
cdc.gov/hpv/hcp/protecting-patients.html.
5
American Cancer Society, “Cancer Vaccines and Their Side Effects,” January 8, 2020, https://www.cancer.org/treatment/
treatments-and-side-effects/treatment-types/immunotherapy/cancer-vaccines.html.
6
Centers for Disease Control and Prevention, “HPV Vaccine Schedule and Dosing,” August 15, 2019, https://www.cdc.gov/
hpv/hcp/schedules-recommendations.html.
1
Making Progress on HPV Vaccination in New York State

Executive Summary (continued)
on the data in the Methods section).
Data on New York City immunizations are maintained
by a separate immunization information system and were not made available for analysis.
Approximately 60% of the statewide population of 13-year-olds resides outside of New York
City.
7,8
7
2019 county population estimates of age group 10–14 were divided by 5 to estimate the number of 13-year-olds per
county. See: United States Census Bureau, “Annual County and Resident Population Estimates by Selected Age Groups
and Sex: April 1, 2010 to July 1, 2019 (CC-EST2019-AGESEX),” https://www.census.gov/data/tables/time-series/demo/
popest/2010s-counties-detail.html.
8
Total statewide population of 13-year-olds calculated in endnote 7 was compared with separate data and found to be
similar. See: United States Census Bureau, “Annual Estimates of the Resident Population by Single Year of Age and Sex for
New York: April 1, 2010 to July 1, 2019,” https://www.census.gov/data/tables/time-series/demo/popest/2010s-state-detail.
html.
2
Making Progress on HPV Vaccination in New York State

Key Findings
z Overall adolescent HPV vaccination coverage increased in New York State (all data are
exclusive of New York City) from 2018 to 2020. In 2020, 24.5% of 13-year-olds had received
both shots of the HPV vaccine series by age 13. By comparison, 20.1% of similarly aged
adolescents completed the HPV vaccine series by age 13 in 2018.
z Although these gains are encouraging, New York State regions outside of New York City
are still falling far short of the State’s Prevention Agenda goal of 37.4% coverage among
13-year-olds by 2024.
9
z Both girls and boys experienced an increase in HPV vaccination coverage over the
study period. While the gap between genders decreased slightly over the time period, a
dierence of 2.5 percentage points in vaccination coverage remained between 13-year-old
girls (25.9%) and boys (23.4%) in 2020.
z Contrary to trends for many other vaccinations, Hispanic or Latino and Black or African-
American adolescents had the highest rates of HPV vaccination coverage over the
study period. The coverage rate increased for all races and ethnicities from 2018–2020 but
remained consistently lower for Asian and white adolescents.
z There was substantial variation in HPV vaccination coverage across counties in New York
State, with only two counties (Cortland and Niagara) meeting the State’s Prevention
Agenda goal of 37.4%. The 2020 coverage rate in the county with the lowest rate, Jeerson,
was less than one-quarter as high as the county with the highest rate, Cortland (9.9%
compared with 40.8%).
z The lowest regional rates of HPV vaccination coverage were consistently found in the
Lower Hudson and Long Island regions (in 2020, 20.5% and 20.9%, respectively). These
regions also had the lowest vaccination coverage for other pediatric vaccinations, studied
in an earlier NYSHealth report here.
New York State is making important progress in improving HPV vaccination rates; policy
changes and public health interventions seem to be working. Factors that may have
contributed to the recent increase in vaccination coverage include improving provider
communication strategies about HPV with parents, expanding adolescent self-consent
policies, and using school-based health centers as HPV vaccinators.
9
New York State Department of Health, “Prevention Agenda 2019-2024: Prevent Communicable Diseases Action Plan,”
https://www.health.ny.gov/prevention/prevention_agenda/2019-2024/comm.htm#FA1.
3
Making Progress on HPV Vaccination in New York State

Key Findings (continued)
Dierences by race and ethnicity persist, however. The higher vaccination coverage rate
among Hispanic or Latino and Black or African-American adolescents may in part be
explained by the higher incidence of HPV-related cancers among those groups compared
with their white counterparts, which may have led to increased vaccination awareness,
outreach, and/or demand.
Despite the notable gains, most New York regions are still not meeting the State’s targets
for HPV vaccinations. In some counties, the gap between current rates and the target is
considerable. Although it is encouraging to see gains for all genders, racial and ethnic
groups, and geographic regions of the State, persistent disparities must be closed so that
all adolescents are equally protected. To end these gaps, New York State could consider
additional policies, including requiring the HPV vaccine for school attendance and studying
the potential of pharmacists to administer the HPV vaccine to young people.
4
Making Progress on HPV Vaccination in New York State

HPV Vaccination Coverage in NY
HPV is a common virus spread through sexual contact. Nearly 43 million Americans have HPV,
making it the single most common sexually transmitted infection.
10
HPV can cause six types of
cancers, including cervical cancer.
11
From 2013 to 2017, an average of 2,730 New Yorkers were
diagnosed with an HPV-related cancer each year, with about 60% of cases among women and
40% among men.
12
In the United States, the Advisory Committee on Immunization Practices (ACIP) issues
recommendations to the Centers for Disease Control and Prevention (CDC) to determine
which vaccinations adolescents should receive. A 2-vaccine series recommended by ACIP
protects against the development of more than 90% of HPV-related cancers, including
cervical cancer and precancers, oropharyngeal cancer, and vaginal and penile cancers.
13
The
CDC recommends that adolescents receive their HPV vaccination at ages 11–12 years, but the
series may be started as early as age 9 and given to young adults through age 26.
14
In this analysis, HPV vaccination coverage was assessed among 3 cohorts of 13-year-old
adolescents (see Table 1) in 2018, 2019, and 2020. The vaccination coverage rate measures
whether they completed the 2-dose HPV vaccine series before the age of 13 years. For
example, adolescents in the 2018 cohort were born from July 2, 2004–July 1, 2005. On July
1, 2018, when the adolescents in this cohort were between the ages of 13 and 14, their
vaccination coverage was assessed to determine if they completed the HPV vaccine series
before the age of 13 years. Only adolescents with at least one administered vaccine (any kind)
recorded in the New York State Immunization Information System (NYSIIS) or a New York State
(exclusive of New York City) birth certicate are included in each cohort.
10
Centers for Disease Control and Prevention, “Sexually Transmitted Infections Prevalence, Incidence, and Cost Estimates in
the United States,” https://www.cdc.gov/std/statistics/prevalence-2020-at-a-glance.htm.
11
Centers for Disease Control and Prevention, “Cancers Caused by HPV,” https://www.cdc.gov/hpv/parents/cancer.html.
12
New York State Department of Health, “HPV-Related Cancer Incidence and HPV Vaccination Rates in New York State,
2013-2017,” https://www.health.ny.gov/statistics/cancer/docs/hpv_related_cancer_13-17.pdf.
13
Centers for Disease Control and Prevention, “Cancers Caused by HPV are Preventable,” September 2020, https://www.
cdc.gov/hpv/hcp/protecting-patients.html.
14
Centers for Disease Control and Prevention, “HPV Vaccination: What Everyone Should Know,” November 16, 2021, https://
www.cdc.gov/vaccines/vpd/hpv/public/index.html.
5
Making Progress on HPV Vaccination in New York State

HPV Vaccination Coverage in NY (continued)
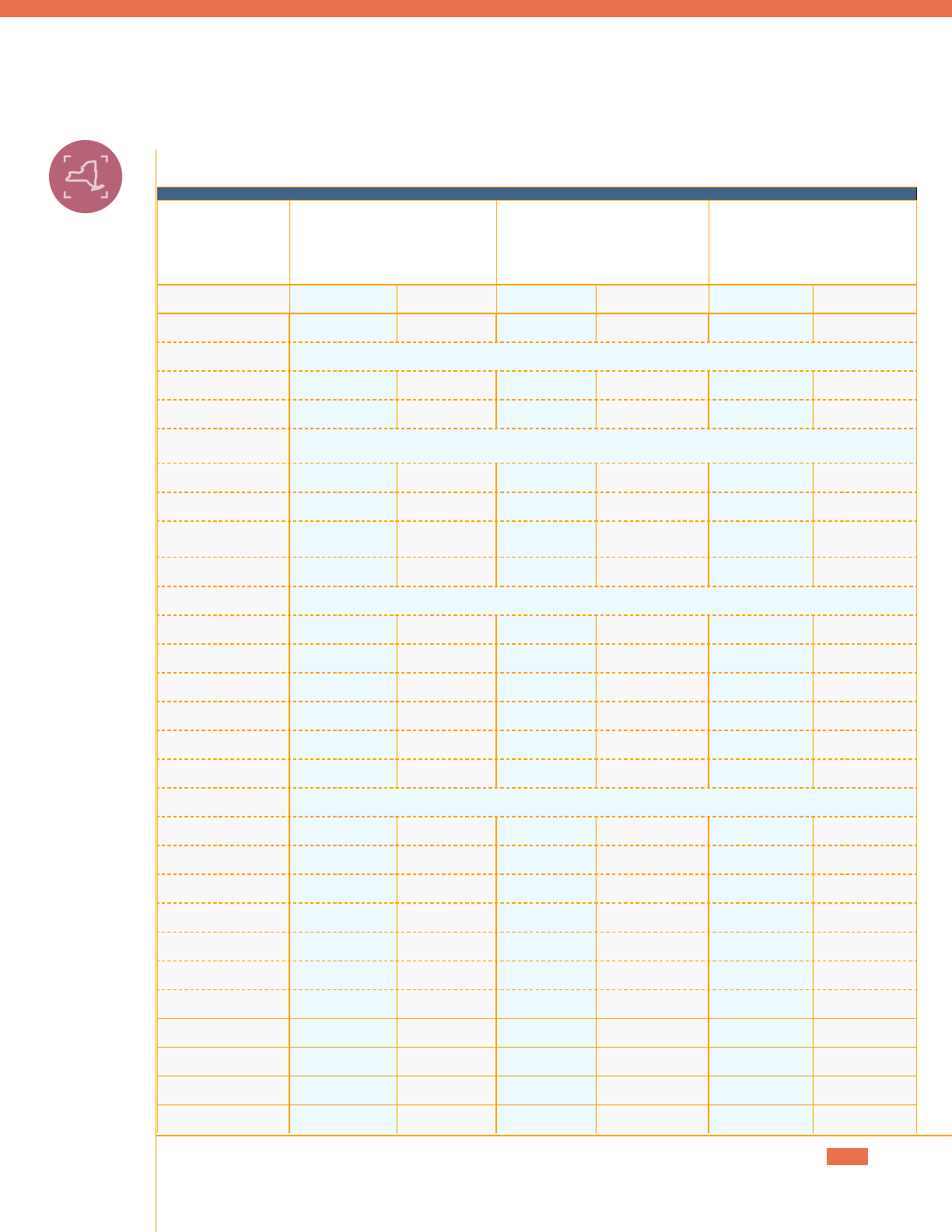
Table 1: Cohorts of Adolescents Studied
Cohort Name Coverage assessed on July 1 of
(age 13 years on this date)
Adolescents born Number of adolescents in
cohort
2018 Cohort 2018 July 2, 2004–July 1, 2005 178,332
2019 Cohort 2019 July 2, 2005–July 1, 2006 175,500
2020 Cohort 2020 July 2, 2006–July 1, 2007 17 7,961
OVERALL
Among 13-year-old adolescents, the HPV vaccination coverage rate grew from 20.1% in July
2018 to 24.5 % in July 2020 (see Figure 1). Despite these improvements, the coverage rate for
the HPV series in parts of the State outside New York City is still well below the State’s 2019–
2024 Prevention Agenda goal of 37.4% for 13-year-olds.
15
FIGURE 1 . HPV Vaccination Coverage in New York State Among
13-Year-Old Adolescents
New York State 2019–2024 Prevention Agenda Target
0%
10%
20%
30%
40%
22.6%
24.5%
20.1%
37.4%
Vaccination Coverage
2018 2019 2020
Note: Age is calculated as of July 1st of each year. Data do not include New York City vaccinations.
Source: NYSHealth analysis of New York State Immunization Information System data.
15
New York State Department of Health, “Prevention Agenda 2019-2024: Prevent Communicable Diseases Action Plan,”
https://www.health.ny.gov/prevention/prevention_agenda/2019-2024/comm.htm#FA1.
6
Making Progress on HPV Vaccination in New York State

HPV Vaccination Coverage in NY (continued)
New York State has experienced similar incremental gains from 2018–2020 with early
childhood vaccinations (such as the Measles, Mumps, and Rubella vaccine), although also
still falling short of key public health targets. Many experts anticipated that the emerging
COVID-19 pandemic would lead to a decrease in vaccination rates in 2020, but creative
approaches for administering vaccines safely (including drive-through and mobile clinics)
likely contributed to increased childhood immunizations during that time. These trends, as
well as a discussion of the potential impact of COVID-19 on vaccinations, are included in
a September 2021 NYSHealth report, “Getting a Fair Shot: Progress and Disparities in Early
Childhood Vaccination in New York State.”
Data on New York City immunizations are maintained by a separate immunization information
system and were not made available for analysis. However, the New York City Department of
Health and Mental Hygiene reports data on HPV vaccination coverage among adolescents
ages 13–17 years. In 2020, 49.9% of adolescents ages 13–17 years in New York City received
a complete HPV series.
16,17
The New York City HPV vaccination coverage rate may be higher
than the State rate in part because it is measured among a wider age range, allowing more
time for adolescents to initiate and complete the vaccine series.
BY GENDER
HPV vaccination coverage increased among both girls and boys from 2018 to 2020. The
coverage rate for girls increased from 21.8% to 25.9% and the rate for boys increased from
18.7% to 23.4% (see Figure 2). Although the gap in coverage between genders decreased over
this period, a dierence of 2.5 percentage points in vaccination coverage persisted between
adolescent girls and boys in 2020.
Adolescent girls historically have had higher rates of HPV vaccination coverage, both
in New York State and nationally.
18
This disparity may be inuenced in part by parental
underestimation of the need to vaccinate adolescent boys against HPV, considering HPV’s
association with cervical cancer. Furthermore, the HPV vaccine was originally approved for
adolescent girls in 2006 and later expanded to boys in 2009, creating lingering misperceptions
of the universal need for HPV vaccination regardless of gender.
16
Dave A. Chokshi, “Fiscal 2021 Mayor’s Management Report - Department of Health and Mental Hygiene,” https://www1.
nyc.gov/assets/operations/downloads/pdf/mmr2021/dohmh.pdf.
17
Dave A. Chokshi, “Department of Health and Mental Hygiene Indicator Definitions, Fiscal 2021 Mayor’s Management
Report,” https://www1.nyc.gov/assets/operations/downloads/pdf/mmr2021/dohmh_idf.pdf.
18
Centers for Disease Control and Prevention, “TeenVaxView: ≥2 Doses HPV Vaccination Coverage by Year among Females
and Males Age 13-17 Years, National Immunization Survey-Teen,” https://www.cdc.gov/vaccines/imz-managers/coverage/
teenvaxview/data-reports/index.html.
7
Making Progress on HPV Vaccination in New York State

HPV Vaccination Coverage in NY (continued)
The gap in vaccination coverage between boys and girls appears to increase as adolescents
get older. A dierent State data source measured HPV vaccination coverage among New York
adolescents ages 13–17 years in 2019 and found that adolescent boys had a coverage rate
nearly 7 percentage points lower than girls.
19
FIGURE 2. HPV Vaccination Coverage in New York State Among
13-Year-Old Adolescents, by Gender
Vaccination Coverage
0%
10%
20%
30%
40%
Male
Female
202020192018
21.8%
18.7%
24.1%
21.3%
25.9%
23.4%
New York State 2019–2024 Prevention Agenda Target
37.4%
Note: Age is calculated as of July 1st of each year. Data do not include New York City vaccinations.
Source: NYSHealth analysis of New York State Immunization Information System data.
BY RACE/ETHNICITY
The vaccination coverage rate for all races and ethnicities increased from the earliest to
the most recent cohorts studied (see Figure 3). Hispanic or Latino adolescents consistently
had the highest rates of vaccination coverage, with a rate of 40.3% in 2020. Black or African-
American adolescents had a slightly lower rate of 36.1%. Asian and white adolescents had
considerably lower vaccination coverage, with rates of 28.9% and 27.2%, respectively. These
disparities do not appear to be closing; the gap between Hispanic or Latino and both white
and Asian adolescents grew from 2018 to 2020. These patterns are similar on the national
19
Centers for Disease Control and Prevention, “TeenVaxView: ≥2 Doses HPV Vaccination Coverage by Year among Females
and Males Age 13-17 Years, National Immunization Survey-Teen,” https://www.cdc.gov/vaccines/imz-managers/coverage/
teenvaxview/data-reports/index.html.
8
Making Progress on HPV Vaccination in New York State

HPV Vaccination Coverage in NY (continued)
level. From 2015–2019, Hispanic adolescents ages 13–17 years had the highest rate of HPV
vaccination coverage, whereas white adolescents had the lowest rate.
20
(Note: The data used for this report do not include information on vaccinations for adolescents
in New York City, which is home to a higher proportion of New Yorkers of color than the rest
of the State. Data from the rest of the State may not be reective of vaccination coverage in
New York City. Additionally, the data do not have complete race or ethnicity information for all
vaccinations. See Limitations for more details.)
The higher vaccination coverage rate among Hispanic or Latino and Black or African-
American adolescents is a trend that diers from other vaccinations (see prior NYSHealth
research) and may be inuenced by many factors. First, in New York State from 2013–2017,
Black non-Hispanic and Hispanic women had the highest rates of HPV-related cancers.
21
This
disproportionate disease burden may have inuenced HPV vaccination awareness, outreach,
and/or demand. Second, a separate State data source shows that New York (inclusive of New
York City) adolescents ages 13–17 years insured through Medicaid had the highest rates of
HPV vaccination completion compared with those covered by all other types of insurance.
22
Adolescents of color are more likely to be insured through Medicaid in New York State, which
may also contribute to their higher vaccination coverage rate.
23
Finally, researchers have found
that living in lower-income communities is associated with higher HPV vaccination initiation.
24
Although having a low income is typically associated with barriers to health care access,
adolescents in these communities may be more likely to use safety-net immunization services
like the Vaccines for Children (VFC) program. This federally funded program provides vaccines
at no cost to children who might otherwise be unvaccinated because of inability to pay.
25
VFC
20
Centers for Disease Control and Prevention, “Vaccination Coverage among Adolescents Age 13–17 Years, Survey Years
2015-2019, United States, National Immunization Survey-Teen,” accessed October 2021, https://www.cdc.gov/vaccines/
imz-managers/coverage/teenvaxview/data-reports/index.html.
21
New York State Department of Health, “HPV-Related Cancer Incidence and HPV Vaccination Rates in New York State,
2013-2017,” https://www.health.ny.gov/statistics/cancer/docs/hpv_related_cancer_13-17.pdf.
22
Centers for Disease Control and Prevention, “TeenVaxView: Vaccination Coverage among Adolescents Age 13–17 Years,
Survey Years 2015-2019, New York, National Immunization Survey-Teen,” https://www.cdc.gov/vaccines/imz-managers/
coverage/teenvaxview/data-reports/index.html.
23
Centers for Disease Control and Prevention, “Vaccination Coverage among Adolescents Age 13–17 Years, Survey Years
2015-2019, New York, National Immunization Survey-Teen,” https://www.cdc.gov/vaccines/imz-managers/coverage/
teenvaxview/data-reports/index.html.
24
Kevin A. Henry et al., “Geographic Factors and Human Papillomavirus (HPV) Vaccination Initiation among Adolescent
Girls in the United States,” Cancer Epidemiology Biomarkers & Prevention 25, no. 2 (February 2016): 309–17, https://doi.
org/10.1158/1055-9965.EPI-15-0658.
25
Centers for Disease Control and Prevention, “Vaccines for Children Program (VFC),” February 18, 2016, https://www.cdc.
gov/vaccines/programs/vfc/index.html.
9
Making Progress on HPV Vaccination in New York State

HPV Vaccination Coverage in NY (continued)
providers participate in a CDC immunization quality improvement program, through which
local health departments work with VFC providers to implement evidence-based strategies
to increase vaccination coverage levels and decrease missed vaccination opportunities
(e.g., scheduling the next vaccination visit before the patient leaves, giving a strong vaccine
recommendation, leveraging immunization information systems to identify patients).
26
Hispanic or Latino and Black or African-American adolescents may in part have higher rates
of HPV vaccination coverage because they are more likely to see a provider trained in these
strategies.
FIGURE 3. HPV Vaccination Coverage in New York State Among
13-Year-Old Adolescents, by Race/Ethnicity
0%
10%
20%
30%
40%
50%
White
Asian
Black or African American
Hispanic or Latino
202020192018
New York State 2019–2024
Prevention Agenda Target
37.4%
33%
31.5%
24.4%
22.4%
Vaccination Coverage
37.9%
34.1%
26.6%
25%
40.3%
36.1%
28.9%
27.2%
Note: Data do not include New York City vaccinations. Adolescents with an ethnicity of Hispanic or Latino in the data
were categorized as Hispanic or Latino. Adolescents with an ethnicity of non-Hispanic or “ethnicity unknown” were
categorized as Black or African American, white, or Asian, according to their race identied in the data.
Source: NYSHealth analysis of New York State Immunization Information System data.
BY GEOGRAPHIC AREA (COUNTY & REGION)
Signicant dierences in vaccination coverage exist across counties in New York State. Among
the 2020 cohort of adolescents, the vaccination coverage rate in the county with the lowest
26
Centers for Disease Control and Prevention, “Immunization Quality Improvement for Providers (IQIP),” July 13, 2020, https://
www.cdc.gov/vaccines/programs/iqip/at-a-glance.html.
10
Making Progress on HPV Vaccination in New York State
HPV Vaccination Coverage in NY (continued)
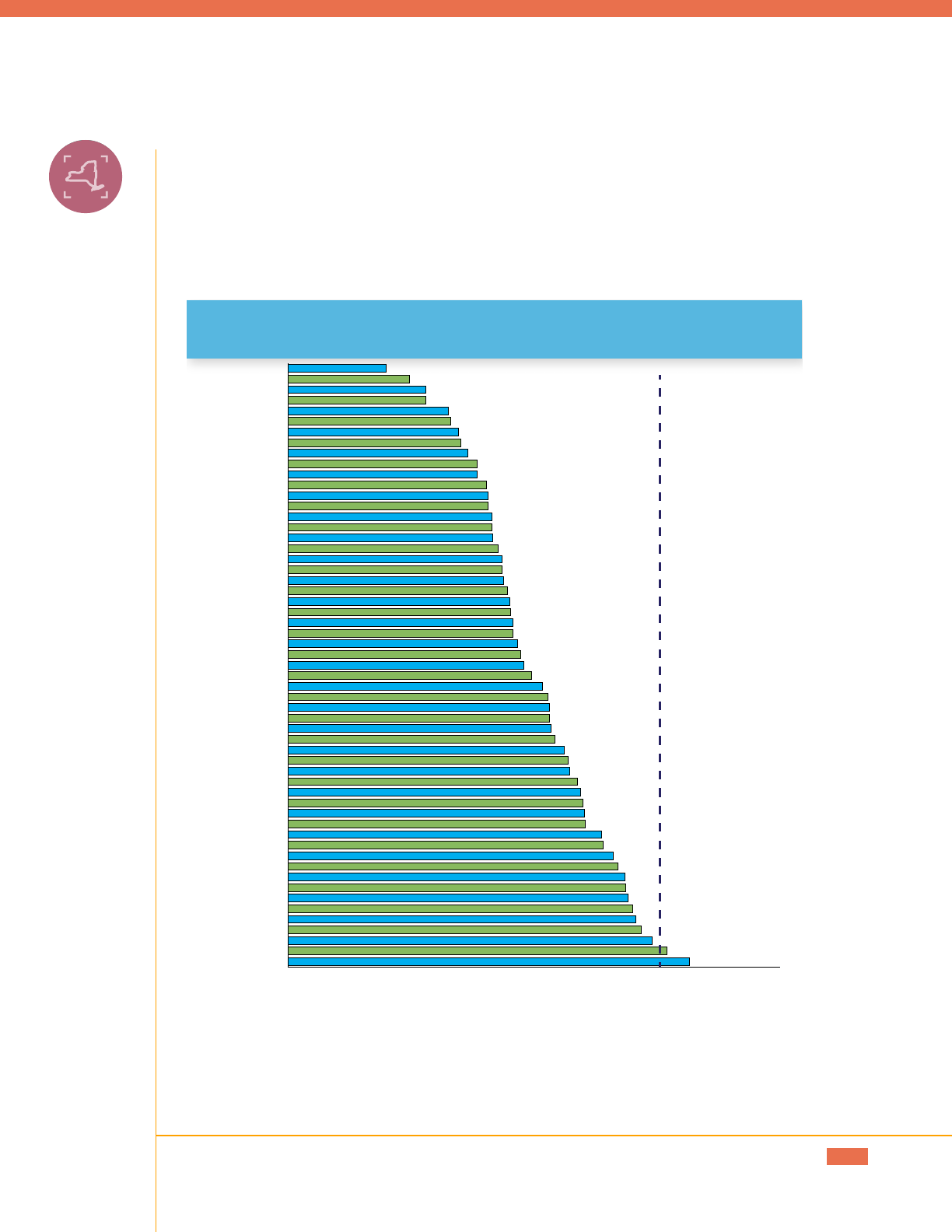
rate, Jeerson (9.9%), was approximately one-quarter as high as the county with the highest
rate, Cortland (40.8%) (see Figure 4). Only two counties have reached the State Prevention
Agenda target of 37.4% (Cortland and Niagara). Counties with the lowest vaccination coverage
tend to cluster in the Lower Hudson, Long Island, and Central regions of New York State.
FIGURE 4. HPV Vaccination Coverage in New York State Among
13-Year-Old Adolescents, by County (2020)
0% 10% 20% 30% 40% 50%
Cortland
Niagara
Chautauqua
Erie
Wyoming
Warren
Wayne
Otsego
Cayuga
Livingston
Monroe
Oswego
Genesee
Allegany
Onondaga
Orleans
Chenango
Albany
Schenectady
Ontario
Madison
Greene
Clinton
Cattaraugus
Rensselaer
Oneida
Schuyler
Chemung
Steuben
Washington
Tompkins
Seneca
Delaware
Tioga
Westchester
Saratoga
St. Lawrence
Columbia
Suffolk
Sullivan
Orange
Putnam
Montgomery
Herkimer
Fulton
Nassau
Yates
Dutchess
Broome
Ulster
Essex
Schoharie
Rockland
Franklin
Hamilton*
Lewis
Jefferson
New York State 2019–2024
Prevention Agenda Target
37.4%
Note: Data do not include New York City vaccinations. County refers to residence of the adolescent. Asterisk indicates
that the county has a sample size of less than 50.
Source: NYSHealth analysis of New York State Immunization Information System data.
11
Making Progress on HPV Vaccination in New York State

HPV Vaccination Coverage in NY (continued)
12
Making Progress on HPV Vaccination in New York State
Sizeable regional disparities are also present. The Lower Hudson and Long Island regions had
the lowest vaccination coverage (20.5% and 20.9%, respectively) among the most recent cohort
of adolescents studied (see Figure 5). These rates were substantially lower than the rate in
Western New York (35.3%), which exhibited the highest regional coverage rate. These same
regions had the highest and lowest vaccination rates for early childhood vaccination rates
(such as the Measles, Mumps, and Rubella vaccine), studied in a separate NYSHealth analysis.
FIGURE 5 . HPV Vaccination Coverage in New York State Among
13-Year-Old Adolescents, by Region
0%
10%
20%
30%
40%
202020192018
28.2%
22.6%
15.6%
22.2%
27.6%
16.6%
Vaccination Coverage
Lower Hudson
Long Island
Central
Capital
Finger Lakes
Western
New York State 2019–2024 Prevention Agenda Target
37.4%
30.1%
24.2%
18.7%
23.6%
31.8%
18.6%
31%
25%
20.9%
25.7%
35.3%
20.5%
Note: Data do not include New York City vaccinations. County or region refers to residence of the adolescent.
Source: NYSHealth analysis of New York State Immunization Information System data.
Discussion
It is encouraging that New York State has succeeded in increasing HPV vaccination coverage
in recent years. Below we examine factors that may have contributed to this improvement and
what more can be done to accelerate progress.
FACTORS INFLUENCING INCREASES IN HPV VACCINATION COVERAGE
Strong Provider Recommendation
Research shows that a strong provider recommendation is the greatest predictor of an
adolescent receiving the HPV vaccine. In fact, among New York State parents in 2019
who reported not planning to vaccinate their child against HPV in the next year, the most
commonly cited reason was that their child’s health care provider had not recommended
it.
27
Several initiatives in New York State have worked to integrate strong provider
recommendations into all visits adolescents have with their health care providers. For
example, the New York State HPV Coalition implemented a provider quality improvement
project to train practices in strategies that increase HPV vaccination coverage, including how
to communicate vaccine recommendations eectively.
28
Provider recommendations are most eective when they use evidence-based communication
strategies. For example, studies show that parents are more likely to vaccinate their children
when a provider uses a presumptive approach (e.g., “Now that your child is 11, they are due for
their vaccination to protect against HPV-related cancers”) instead of a participatory approach
(e.g., “Would you like to do the HPV vaccine today?”).
29
A bundled approach, in which providers
recommend the HPV in the “same way, same day” as other vaccinations, is also eective.
Many providers, however, have been unprepared to give strong HPV vaccination
recommendations. Some providers have shied away from discussing the HPV vaccine with
parents, given its association with sexual activity.
30
Other providers have an incomplete
understanding of the need to vaccinate adolescent boys.
31
To combat this challenge
nationally, the American Cancer Society has worked to reframe the conversation about HPV,
27
NYSHealth analysis of 2019 National Immunization Survey-Teen data. Data available from: https://www.cdc.gov/vaccines/
imz-managers/nis/datasets-teen.html.
28
New York State HPV Coalition, “New York State HPV Action Plan 2018-2023,” August 2019, http://www.nyshpv.org/wp-
content/uploads/2019/09/NEW-YORK-STATE-HPV-VACCINATION-ACTION-PLAN-3.pdf.
29
Annika M. Hofstetter et al., “Clinician-Parent Discussions about Influenza Vaccination of Children and Their Association
with Vaccine Acceptance,” Vaccine vol. 35, no. 20 (May 9, 2017): 2709–15, https://doi.org/10.1016/j.vaccine.2017.03.077.
30
Melissa B. Gilkey et al. “Quality of Physician Communication about Human Papillomavirus Vaccine: Findings from a
National Survey,” Cancer Epidemiology, Biomarkers & Prevention vol. 24, no. 11 (2015): 1673-9, https://www.ncbi.nlm.nih.
gov/pmc/articles/PMC4633386/.
31
Ibid.
13
Making Progress on HPV Vaccination in New York State
Discussion (continued)
moving focus away from how HPV is transmitted (through sexual activity) and toward what
the HPV vaccine prevents (cancer).
32
With NYSHealth funding, the American Academy of
Pediatrics, the American Cancer Society New York Chapter, and the New York State HPV
Coalition implemented quality improvement projects in 2019–2020 among providers, health
plans, and school-based health centers (SBHCs) to increase HPV vaccination in New York
State.
33
The provider quality improvement project included a provider education program
among more than 50 practices statewide to address gaps in knowledge and attitudes about
the HPV vaccine.
34
The program educated providers about the value of the HPV vaccine and
equipped them with the skills to discuss HPV vaccination with parents.
Advancements of Electronic Health Records (EHRs) and Immunization
Information Systems
With technological advancements of EHRs and immunization information systems, providers
can more easily create reports of patients due or overdue for vaccines. Sophisticated EHRs
support bidirectional information exchange, allowing providers to submit immunization
data from their EHR to NYSIIS and to request that immunization data from NYSIIS be sent to
their EHR.
35
This bidirectionality is particularly helpful for assessing the vaccination status of
patients who do not have a consistent source of primary care; providers can use NYSIIS data to
track which vaccines have been administered to their patients at other points of care. NYSIIS
and some EHR systems can also automatically send reminders to parents for upcoming and
overdue vaccines via mail, phone, or text.
Quality improvement initiatives are increasing the use of NYSIIS among providers to better
track their patients due or overdue for vaccines and generate reminders. The CDC has
designed an immunization quality improvement program, known as IQIP, to increase on-
time vaccination of children and adolescents among providers that participate in the VFC
32
Ibid.
33
New York State Health Foundation, “Improving HPV Vaccination Rates Among Adolescents in New York State,” https://
nyshealthfoundation.org/grantee/american-academy-of-pediatrics-ny-chapter-1/.
34
New York State HPV Coalition, “New York State HPV Action Plan 2018-2023,” August 2019, http://www.nyshpv.org/wp-
content/uploads/2019/09/NEW-YORK-STATE-HPV-VACCINATION-ACTION-PLAN-3.pdf.
35
Neil Murthy et al., “Progress in Childhood Vaccination Data in Immunization Information Systems — United States, 2013–
2016,” MMWR. Morbidity and Mortality Weekly Report 66, no. 43 (November 3, 2017): 1178–81, https://doi.org/10.15585/
mmwr.mm6643a4.
14
Making Progress on HPV Vaccination in New York State

Discussion (continued)
program.
36,37
Local health departments in New York State implement the IQIP program and
conduct site visits annually to one-quarter of their county’s VFC providers.
38
During these
visits, local health departments support VFC providers in leveraging NYSIIS to increase
vaccination coverage. Continued technical assistance will help providers make full use
of NYSIIS and may be particularly eective in increasing vaccination coverage among
adolescents of color, who are more likely to be seen by VFC providers.
Expanded Adolescent Self-Consent Policies
Health care providers are typically required to obtain parental consent before administering
vaccinations to minors. Providers nationwide report that this is a signicant barrier to HPV
vaccination access.
39
In some cases, parents refuse the HPV vaccine because of its association
with sexual activity. In other cases, the consent requirement is a logistical challenge, because
adolescents may present to appointments without a parent, especially in a SBHC.
In 2016, the New York State Department of Health issued regulations to permit providers to
administer the HPV vaccine to sexually active adolescents without parental consent.
40,41
This
policy has helped to increase HPV vaccination access among adolescents who otherwise
would have been unable to receive the vaccine.
Integrating HPV Vaccination into School-Based Health Centers
School-Based Health Centers are medical centers located within public schools. Run by local
hospitals, medical centers, and community organizations, SBHCs can provide students with
36
The Vaccines for Children program provides vaccines purchased by the federal government to providers to administer
to low-income children. See: Centers for Disease Control and Prevention, “Vaccines for Children Program,” February 18,
2016, https://www.cdc.gov/vaccines/programs/vfc/index.html.
37
Centers for Disease Control and Prevention, “Immunization Quality Improvement for Providers,” July 13, 2020, https://www.
cdc.gov/vaccines/programs/iqip/index.html.
38
New York State Association of County Health Officials (NYSACHO). “Update LHD IAP Work Plan (for the period starting
4/1/20).” Document obtained via email correspondence with NYSACHO.
39
Carol A. Ford et al., “Minor Consent and Delivery of Adolescent Vaccines,” The Journal of Adolescent Health :
Official Publication of the Society for Adolescent Medicine 54, no. 2 (February 2014): 183–89, https://doi.org/10.1016/j.
jadohealth.2013.07.028.
40
10 NYCRR §23.4 (2016).
41
New York State Department of Health, “Guidance for Local Health Departments (LHD) and Health Care Providers on STI
Billing and Minor’s Consent to Prevention Services and HIV-related Services,” November 2019, https://www.health.ny.gov/
diseases/communicable/std/docs/faq_billing_consent.pdf.
15
Making Progress on HPV Vaccination in New York State

Discussion (continued)
primary care, mental health services, and vaccinations. More than 260,000 students in New
York State are enrolled in a school with an SBHC.
42
SBHCs are critical sites for HPV vaccination. In addition to providing HPV vaccines, SBHCs
also conduct important work educating both students and parents about the importance of
HPV vaccination. In partnership with the New York School-Based Health Alliance, the New
York State HPV Coalition has recently worked to enhance HPV vaccinations at SBHCs. Among
other eorts, the groups authored a guide for providing SBHCs with technical assistance
on developing parental consent policies, modifying oce practices, and adopting eective
communication strategies.
43
These eorts may have contributed to recent increases in HPV
vaccination coverage among adolescents.
WHAT MORE SHOULD BE CONSIDERED TO INCREASE VACCINATION
COVERAGE AND ELIMINATE DISPARITIES?
Although the preceding eorts have contributed to increases in HPV vaccination coverage
among adolescents, more work remains to meet State targets and close disparities by gender,
race and ethnicity, and geography. The following strategies may help New York State build
upon recent gains and protect even more adolescent New Yorkers from HPV.
Require the HPV vaccine for school attendance
School mandates are the most eective compliance mechanism for ensuring that school-
age children receive their recommended vaccinations. New York State already requires that
middle school and high school students receive the Tdap (Tetanus, Diphtheria, Pertussis)
vaccine and the Meningococcal conjugate vaccine—in addition to 5–7 other vaccinations
required for younger ages.
44
Adding the HPV vaccine as a requirement for school attendance
would help to further increase vaccination coverage.
It is important to note that states and jurisdictions that require the HPV vaccine for school
attendance have had mixed success.
45
However, some of these requirements only apply to
42
New York State Department of Health, “School-Based Health Centers Fact Sheet,” May 2021, https://www.health.ny.gov/
statistics/school/skfacts.htm.
43
Jana Shaw and Michael Seserman, “NYS HPV Vaccination Guide for School-Based Health Centers,” New York State HPV
Coalition, June 2019, http://www.nyshpv.org/wp-content/uploads/2019/06/NYS-Guide-to-Increase-HPV-Vaccination-
FINAL-6.10.19.pdf.
44
New York State Department of Health, “School Vaccination Requirements,” September 2020, https://www.health.ny.gov/
prevention/immunization/schools/school_vaccines/.
45
National Conference of State Legislatures, “HPV Vaccine: State Legislation and Regulation,” https://www.ncsl.org/
16
Making Progress on HPV Vaccination in New York State

Discussion (continued)
adolescent girls and/or allow parents to opt out of the requirement.
46,47
Given that New York
State prohibits nonmedical exemptions to school vaccination requirements, adding the HPV
vaccine to school entry requirements would likely be more eective than in states that have
seen less success. Legislation introduced during the 2019–2020 New York State legislative
session would have designated the HPV vaccine series as a required school immunization for
all students, but the bill died in committee.
48
Study the role of pharmacists as adolescent vaccinators
In recent years, many states have begun expanding the types of providers who can administer
vaccinations, either by expanding a licensure’s scope of practice or through standing order
procedures.
49
Although all states grant the authority to pharmacists to vaccinate, each state
has dierent rules regarding the vaccines they can administer and the age groups they can
vaccinate. New York State is one of only two states in the United States that does not permit
pharmacists to administer the HPV vaccine.
50
In 2021, Governor Hochul signed legislation authorizing pharmacists to administer
immunizations recommended by the CDC to patients 18 years and older.
51
Although this
legislation may increase HPV vaccination access among young adults who have not yet
received the vaccine series, it will not allow pharmacists to administer the series during the
recommended ages of 11–12 years.
Recognizing the potential of pharmacists to increase childhood vaccination coverage during
the coronavirus pandemic, the U.S. Department of Health and Human Services (HHS) issued a
directive in August 2020 authorizing state-licensed pharmacists in all 50 states to administer
ACIP-recommended vaccines to children ages 3–18 years.
52
New York State should conduct
46
D.C. Code § 7-1651.04(b)
47
Virginia Department of Health, “Virginia Adolescent Vaccination Schedule 7 Years–18 Years,” https://www.vdh.virginia.gov/
content/uploads/sites/11/2021/03/VDH-Vaccine-Schedule.pdf.
48
S298B. 2019 Reg. Sess (NY 2019).
49
National Council of State Legislatures, “State Immunization Policy Overview,”https://www.ncsl.org/research/health/
immunizations-policy-issues-overview.aspx.
50
American Pharmacists Association and National Alliance of State Pharmacy Associations, “Pharmacist-Administered
Vaccines,” June 2020, https://aphanet.pharmacist.com/sites/default/files/files/practice/07-2020/pharmacist-administered-
vaccines-june-2020.pdf.
51
S4807A. 2021 Reg. Sess (NY 2021).
52
U.S. Department of Health & Human Services, “HHS Expands Access to Childhood Vaccines during COVID-19 Pandemic,”
August 19, 2020, https://www.hhs.gov/about/news/2020/08/19/hhs-expands-access-childhood-vaccines-during-covid-19-
pandemic.html.
17
Making Progress on HPV Vaccination in New York State
Discussion (continued)
an assessment of pharmacists providing adolescent and pediatric vaccinations under this
authorization to evaluate its outcomes. If the benets to vaccination coverage are large, and
the risks minimal, the evidence may point in favor of permanently authorizing pharmacists to
administer adolescent and pediatric vaccinations.
18
Making Progress on HPV Vaccination in New York State
Conclusion
From 2018 to 2020, New York State made gains in HPV vaccination coverage among 13-year-
olds. The improvement may have been inuenced by a number of factors, including eorts
to strengthen health care providers’ communication and recommendation of the vaccine to
parents of adolescents; technological advances that allow providers to better identify children
due or overdue for vaccinations and generate parent reminders; expansion of adolescent self-
consent policies; and the integration of HPV vaccines into SBHCs.
Despite this progress, New York’s overall HPV vaccination coverage rate falls short of the
State’s Prevention Agenda objectives, and it is far below the target in pockets of the State.
Disparities by race, ethnicity, gender, and geography persist despite overall increases in
vaccination coverage. New York State could explore promising strategies to establish HPV
vaccine requirements for school attendance and assess an expanded role for pharmacists
in administering the vaccine to adolescents. Such measures could ensure that the State
continues to make progress in protecting young people against the consequences of HPV.
19
Making Progress on HPV Vaccination in New York State

Methods
DATA
The data used for the analysis were obtained from NYSIIS. We are grateful to Claire McGarry,
Research Scientist at NYSIIS, for fullling the data request.
Since January 1, 2008, all health care providers in New York State are required to report
all immunizations administered to persons less than 19 years of age to the New York
State Department of Health via NYSIIS.
53
NYSIIS does not contain data for immunizations
administered in New York City, which manages its own immunization registry. See Appendix
for the denominator and vaccination coverage rate for the groups of cohorts studied (overall
and by gender, race/ethnicity, region, and county).
COHORTS STUDIED
Vaccination coverage was assessed among the three cohorts of adolescents in the following
table. Only adolescents with at least one administered vaccine (any kind) recorded in NYSIIS or
a New York State (exclusive of New York City) birth certicate are included in each cohort.
Cohort Name Coverage assessed on July 1 of
(age 13 years on this date)
Adolescents born Number of adolescents
in cohort
2018 Cohort 2018 July 2, 2004–July 1, 2005 178,332
2019 Cohort 2019 July 2, 2005–July 1, 2006 175,500
2020 Cohort 2020 July 2, 2006–July 1, 2007 17 7,961
Source: NYSHealth analysis of New York State Immunization Information System data.
CALCULATION OF RATES
For each cohort analyzed in this report, the HPV vaccination coverage rate is calculated as the
percentage of the applicable population that completed the vaccine series before the age of
13 years. The applicable population is 13-year-old adolescents within each birth cohort with a
record in NYSIIS or a New York State (exclusive of New York City) birth certicate.
53
New York State Department of Health, “New York State Immunization Information System (NYSIIS),” https://www.health.
ny.gov/prevention/immunization/information_system/.
20
Making Progress on HPV Vaccination in New York State
vaccination
coverage
x 100
adolescents ages 13 years who completed HPV series before age 13 years
all adolescents ages 13 years with ≥1 vaccine (any kind) recorded in NYSIIS
or a New York State (New York City-exclusive) birth certicate
=
Methods (continued)
Vaccination coverage analyses typically use data from an immunization information system
or census data for the denominator.
54
In this analysis, the data for the denominator is based
on NYSIIS. The State’s Prevention Agenda, however, uses census data in the denominator
to calculate adolescent HPV vaccination coverage. See Li mitations for more details on the
advantages and disadvantages of each denominator data source.
Vaccination coverage was assessed using a point-in-time assessment, as of July 1st of each
year. A point-in-time assessment is an appropriate method to track coverage rates over time,
as it allows cohorts from one assessment period to the next to be held to the same age
range.
55
CATEGORIZATIONS
For analyses by race and ethnicity, adolescents with an ethnicity of Hispanic or Latino
recorded in NYSIIS were categorized as Hispanic or Latino. Adolescents with an ethnicity of
non-Hispanic or Latino or “ethnicity unknown” were categorized as Black or African American,
white, or Asian, according to their race identied in NYSIIS. Adolescents with an ethnicity of
“ethnicity unknown” were categorized by race to maintain as much data on race as possible.
An analysis was also conducted where adolescents with an ethnicity of “ethnicity unknown”
were excluded from the analysis, and the vaccination coverage trends by race and ethnicity
were similar to those produced by the less-restrictive categorization approach. Geographic
analyses are based on the residence of the adolescent recorded within NYSIIS.
54
American Immunization Registry Association, “Analytic Guide for Assessing Vaccination Coverage Using an IIS,”
November 2015, https://repository.immregistries.org/resource/analytic-guide-for-assessing-vaccination-coverage-using-
an-iis/.
55
Ibid.
21
Making Progress on HPV Vaccination in New York State

Limitations
All ndings in this report describe vaccination coverage for New York State, exclusive of New
York City. Readers should interpret the ndings as representative of only the 57 counties
outside of New York City.
A widely used data source for immunization rate surveillance is the National Immunization
Surveys (NIS), which are telephone surveys conducted by the CDC’s National Center for
Immunization and Respiratory Diseases. However, NIS data are reported with a two-year
lag, and condence intervals for local estimates are often wide, limiting their usefulness for
vaccination program design.
56
In this analysis, NYSIIS data were used to provide a timelier analysis of vaccination coverage
trends. Rates calculated from NYSIIS data have been historically lower than rates calculated
from annual NIS data, in part because of incomplete reporting.
57
It has also been shown
that the denominator for measures based on immunization information systems may be
overestimated because of movement out of state (i.e., adolescents who move into a state
have records added to the immunization information system, whereas adolescents who move
out of that state may not be immediately removed from the system) and duplicate records.
58
The total number of 13-year-olds in New York State (exclusive of New York City) calculated by
NYSIIS is higher than the 2019 Census estimate; the 2019 NYSIIS estimate is 175,500, whereas
the 2019 Census estimates is 131,384.
59
However, aside from being timelier, another key
advantage of using the immunization information system data to analyze coverage rates is that
the same data source can be used for the denominator and the numerator. Also, a national
comparison of immunization information systems and NIS data found that immunization
information systems are becoming more complete over time, and vaccination coverage
estimates from immunization information systems are becoming increasingly close to NIS
56
Centers for Disease Control and Prevention, “Validation of an Immunization Information System Against the National
Immunization Survey and Improvement of Hepatitis B Birth Dose Coverage in New York City,” https://cdc.confex.com/cdc/
nic2008/techprogram/P15344.HTM.
57
Dina Hoefer, New York State Department of Health, “Immunization Coverage in NYS: Impact of Programmatic Activities
and Policies on 4:3:1:3:3:1:4 Rates,” https://repository.immregistries.org/files/resources/5835ade1a117b/track_d__
promoting_partnerships___assessing_outcomes_.pdf.
58
American Immunization Registry Association. “Analytic Guide for Assessing Vaccination Coverage Using an IIS,” https://
repository.immregistries.org/files/resources/5835adc2ae282/analytic_guide_for_assessing_vaccination_coverage_using_
an_iis_november_2015.pdf.
59
The Census estimate is calculated by dividing the 10–14 age group estimate by 5. Data available from: https://www2.
census.gov/programs-surveys/popest/datasets/2010-2019/counties/.
22
Making Progress on HPV Vaccination in New York State

Limitations (continued)
estimates.
60
From 2018 to 2020, 34–35% of records in NYSIIS were missing both a race and an ethnicity
categorization; these gaps may have aected the vaccination rates in the race and ethnicity
analyses. However, a nationwide study found similar disparities by race and ethnicity among
adolescents ages 13–17 years.
61
60
Murthy et al., “Progress in Childhood Vaccination Data in Immunization Information Systems — United States, 2013–2016,”
https://www.cdc.gov/mmwr/volumes/66/wr/mm6643a4.htm.
61
See Online Supplementary Table 1 within: Cassandra Pingali et al., “National, Regional, State, and Selected Local Area
Vaccination Coverage Among Adolescents Aged 13–17 Years — United States, 2020,” Centers for Disease Control and
Prevention, Morbidity and Mortality Weekly Report, vol. 70, no. 35 (2021): 8, https://www.cdc.gov/mmwr/volumes/70/wr/
pdfs/mm7035a1-H.pdf.
23
Making Progress on HPV Vaccination in New York State
2018
ADOLESCENTS BORN
JULY 2, 2004–JULY 1, 2005
2019
ADOLESCENTS BORN
JULY 2, 2005–JULY 1, 2006
2020
ADOLESCENTS BORN
JULY 2, 2006–JULY 1, 2007
Tot al Vaccination Tot al Vaccination
Tot al Vaccination
OVERALL
178,332 20.1 175,500 22.6 177,961 24.5
Gender
Female 86,276 21.8 84,855 24.1 86,418 25.9
Male 91,293 18.7 89,925 21.3 90,734 23.4
RACE/
ETHNICITY
White 72,160 22.4 69,524 25.0 70,194 27.2
Hispanic or Latino 21,407 33.6 20,995 37.9 22,042 40.3
Black or African
American
12,141 31.5 12,113 34.1 12,518 36.1
Asian 5,905 24.4 5,509 26.6 5,640 28.9
REGION
Capital 20,603 22.2 20,435 23.6 20,499 25.7
Central 24,872 22.6 24,857 24.2 25,514 25.0
Finger Lakes 18,295 28.2 18,240 30.1 18,988 31.0
Long Island 48,083 15.6 47,123 18.7 46,637 20.9
Lower Hudson 42,261 16.6 41,210 18.6 41,642 20.5
Western 21,096 27.6 20,632 31.8 21,559 35.3
COUNTY
Albany 4,321 24.3 4,525 26.2 4,412 29.4
Allegany 636 22.2 616 25.8 605 30.2
Broome 2,755 19.1 2,634 18.6 2,770 18.2
Cattaraugus 1,127 22.3 1,103 24.4 1,248 26.5
Cayuga 868 30.8 888 32.5 916 34.2
Chautauqua 1,800 30.4 1,848 35.0 1,932 37.0
Chemung 1,215 23.5 1,137 26.1 1,349 24.7
Chenango 651 27.6 640 26.1 683 29.7
Clinton 949 24.1 986 25.3 1,013 26.7
Columbia 751 21.0 751 23.8 745 21.7
Cortland 621 30.1 611 34.4 596 40.8
Delaware 482 18.3 502 21.1 558 22.8
Dutchess 4,494 14.8 4,352 17.0 4,369 19.2
Erie 12,910 27.6 12,614 31.6 13,098 35.9
Essex 453 14.6 436 17.9 410 17.3
Franklin 596 18.8 631 16.3 627 14.0
Fulton 652 13.7 642 17.6 649 20.3
Genesee 781 29.8 763 33.6 789 31.8
Greene 616 25.8 601 23.5 572 27.1
Hamilton 56 14.3 46 17.4 43 14.0
24
Making Progress on HPV Vaccination in New York State
Appendix

2018
ADOLESCENTS BORN
JULY 2, 2004–JULY 1, 2005
2019
ADOLESCENTS BORN
JULY 2, 2005–JULY 1, 2006
2020
ADOLESCENTS BORN
JULY 2, 2006–JULY 1, 2007
COUNTY
Tot al Vaccination Tot al Vaccination
Tot al Vaccination
Delaware 482 18.3 502 21.1 558 22.8
Dutchess 4,494 14.8 4,352 17.0 4,369 19.2
Erie 12,910 27.6 12,614 31.6 13,098 35.9
Essex 453 14.6 436 17.9 410 17.3
Franklin 596 18.8 631 16.3 627 14.0
Fulton 652 13.7 642 17.6 649 20.3
Genesee 781 29.8 763 33.6 789 31.8
Greene 616 25.8 601 23.5 572 27.1
Hamilton 56 14.3 46 17.4 43 14.0
Herkimer 798 20.9 792 24.2 801 20.3
Je erson 2,391 8.4 2,575 8.9 2,700 9.9
Lewis 377 9.0 421 11.2 373 12.3
Livingston 796 27.8 803 31.8 762 33.5
Madison 919 21.2 864 23.3 927 28.0
Monroe 11,087 30.3 11,220 32.0 11,605 33.0
Montgomery 875 18.2 819 18.7 870 20.7
Nassau 22,517 15.3 22,367 18.0 22,174 20.1
Niagara 2,758 29.1 2,722 34.4 2,816 38.5
Oneida 3,273 21.3 3,295 25.9 3,360 26.4
Onondaga 7,1 42 29.0 7,086 30.4 7,180 30.1
Ontario 1,464 25.8 1,462 26.8 1,494 28.4
Orange 7,376 17.4 7,421 20.4 7,302 20.8
Orleans 564 22.3 519 29.7 539 29.9
Oswego 1,581 27.5 1,623 30.4 1,599 32.0
Otsego 723 21.7 693 26.8 700 34.3
Putnam 1,508 13.7 1,445 16.7 1,437 20.7
Rensselaer 2,239 22.6 2,072 24.1 2,154 26.5
Rockland 6,827 12.3 6,572 13.3 6,833 16.3
Saratoga 3,402 20.8 3,392 20.5 3,395 22.3
25
Making Progress on HPV Vaccination in New York State
Appendix (continued)

2018
ADOLESCENTS BORN
JULY 2, 2004–JULY 1, 2005
2019
ADOLESCENTS BORN
JULY 2, 2005–JULY 1, 2006
2020
ADOLESCENTS BORN
JULY 2, 2006–JULY 1, 2007
COUNTY
Tot al Vaccination Tot al Vaccination
Tot al Vaccination
Saint Lawrence 1,458 20.6 1,459 21.9 1,482 21.9
Schenectady 2,430 26.9 2,417 27. 4 2,378 28.6
Schoharie 367 19.9 348 17.8 345 16.5
Schuyler 225 33.8 193 28.5 209 25.8
Seneca 448 19.2 441 21.8 434 22.8
Steuben 1,419 19.1 1,332 24.2 1,408 23.9
S u o l k 25,566 15.8 24,756 19.3 24,463 21.7
Sullivan 1,274 18.9 1,225 20.5 1,342 21.3
Tioga 713 14.0 669 17.0 758 22.6
Tompkins 1,325 19.2 1,300 19.9 1,369 23.3
Ulster 2,389 13.6 2,414 15.4 2,459 17.5
Warren 840 25.7 790 28.5 783 35.0
Washington 851 16.9 784 21.6 845 23.6
Wayne 1,325 30.9 1,311 31.3 1,389 34.5
Westchester 18,393 18.8 17,781 20.6 17,900 22.5
Wyoming 520 32.5 447 31.1 532 35.3
Yates 316 20.9 341 22.0 338 19.2
26
Making Progress on HPV Vaccination in New York State
Appendix (continued)

Improving the state of
New York’s health
VOICE:
212-664-7656
FAX:
646-421-6029
MAIL:
1385 Broadway,
23rd Floor
New York, NY 10018
WEB:
www.nyshealth.org
