

Bureau of Primary Health Care
Uniform Data System
Reporting Requirements for
2023 Health Center Data
PUBLIC BURDEN STATEMENT
The Uniform Data System (UDS) provides consistent information about health centers including patient characteristics, services provided, clinical processes
and health outcomes, patients’ use of services, costs, and revenues. It is the source of unduplicated data for the entire scope of services included in the grant
or designation for the calendar year. An agency may not conduct or sponsor, and a person is not required to respond to, a collection of information unless it
displays a currently valid Office of Management and Budget (OMB) control number. The OMB control number for this project is 0915-0193 and it is valid
until 04/30/2026. This information collection is mandatory under the Health Center Program authorized by section 330 of the Public Health Service (PHS)
Act (42 U.S.C. 254b
). Public reporting burden for this collection of information is estimated to average 238 hours per response, including the time for
reviewing instructions, searching existing data sources, and completing and reviewing the collection of information. Send comments regarding this burden
estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to the Health Resources and Services
Administration (HRSA) Reports Clearance Officer, 5600 Fishers Lane, Room 14N136B, Rockville, Maryland, 20857 or
paperwork@hrsa.gov.
DISCLAIMER
“This publication lists non-federal resources to provide additional information to consumers. Neither the U.S. Department of Health and Human Services
(HHS) nor the Health Resources and Services Administration (HRSA) has formally approved the non-federal resources in this manual. Listing these is not
an endorsement by HHS or HRSA.”

Letter from the Associate Administrator
Dear Health Center Program Participant:
Your success in providing affordable, accessible, and high-quality primary health care to more than 30 million
patients from medically underserved communities is a testament to your dedication to those patients. Health
centers are continuously innovating to expand access, improve care quality, increase cost effectiveness, and
advance health equity while also addressing challenges presented to patients, communities, and health care
providers in today’s dynamic and ever-changing health care environment.
The Health Resources and Services Administration (HRSA) is committed to pursuing new and innovative
technologies to support health centers in delivering high-quality, patient-centered, and integrated care. Health
information technology (health IT) is an essential tool in supporting value-based care delivery and, ultimately,
better health outcomes. The 21st Century Cures Act has been important in codifying ways for patients and
providers to access and exchange health data in safe and secure ways through advances in health IT. HRSA
appreciates health centers’ efforts to leverage these advances to support the transition toward health center
reporting of de-identified patient-level data to HRSA, also known as Uniform Data System (UDS) Patient-Level
Submission, or UDS+.
UDS+ will greatly enhance data quality and granularity, paving the path toward reducing reporting burden and
reliance on manual data entry and improving the ability of health centers and HRSA to better identify and address
the clinical needs of complex patient populations. Additionally, these data will allow for communities as well as
local, state, and federal agencies to better identify areas of strategic partnership with the Health Center Program;
inform development of targeted training and technical assistance; and advance quality improvement research to
further advance equitable access to high-quality, cost-effective care.
While health centers will submit a full UDS Report within EHBs for this calendar year 2023 reporting period, we
will also begin to accept de-identified patient-level data submissions. The 2023 UDS Manual provides
instructions for UDS Report submissions and, for the first time, includes information and resources on how to
submit de-identified patient-level data for specified tables using FHIR R4 standards.
Thank you to the health center workforce, which has risen to meet public health challenges with remarkable
resolve, while continuing to demonstrate adaptability and a willingness to evolve as we work together to improve
the quality and impact of the Health Center Program. You are the drivers of this transformation to innovate how
care is delivered to millions of medically underserved people across the country, and through UDS data, we are
able to tell this story.
Thank you,
/James Macrae/
James Macrae
Associate Administrator
Bureau of Primary Health Care


UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
5 2023 UDS MANUAL | Table of Contents
2023 Uniform Data System Manual Contents
Letter from the Associate Administrator ......... 3
2023 Uniform Data System Manual Contents . 5
Changes to the Reporting Requirements ........ 10
Introduction ...................................................... 11
About the UDS ............................................... 11
What This Manual Includes ............................ 11
General Instructions ......................................... 12
What to Submit ............................................... 12
What Is Included............................................. 12
Calendar Year Reporting ................................ 13
In-Scope Reporting ......................................... 14
Due Dates and Revisions to Reports .............. 14
How and Where to Submit Data ..................... 14
FAQ for the General Instructions ................... 17
Instructions for Tables that Report Visits, Patients,
and Providers .................................................... 19
Countable Visits ............................................. 19
Documentation ........................................... 19
Independent Professional Judgment ........... 20
Behavioral Health Group Visits ................. 20
Location of Services Provided .................... 20
Counting Multiple Visits by Category of Service
.................................................................... 21
Patient ............................................................. 21
Services and Individuals NOT Reported on the
UDS Report ................................................ 22
Provider .......................................................... 23
FAQ for the Instructions for Tables ............... 24
Instructions for Patients by ZIP Code Table . 25
Patients by ZIP Code ...................................... 25
ZIP Code of Specific Groups ..................... 25
Unknown ZIP Code .................................... 25
Ten or Fewer Patients in ZIP Code ............ 26
Instructions for Type of Insurance .................. 26
Insurance Categories .................................. 26
FAQ for Patients by ZIP Code Table ............. 27
Patients by ZIP Code Table ............................ 29
Instructions for Tables 3A and 3B .................. 30
Table 3A: Patients by Age and by Sex Assigned at
Birth ................................................................... 30
Table 3B: Demographic Characteristics ........ 31
Patie
nts by Hispanic, Latino/a, or Spanish Ethnicity
and Race (Lines 1–8) ...................................... 31
Hispanic, Latino/a, or Spanish Ethnicity .... 31
Race ............................................................ 33
Patients Best Served in a Language Other than
English (Line 12) ............................................ 34
Patients by Sexual Orientation (Lines 13–19) 34
Patients by Gender Identity (Lines 20–26) ..... 34
FAQ for Tables 3A and 3B ............................ 35
Table 3A: Patients by Age and by Sex Assigned at
Birth ................................................................ 38
Table 3B: Demographic Characteristics ......... 39
Instructions for Table 4: Selected Patient
Characteristics .................................................. 41
Income as a Percentage of Poverty Guideline, Lines
1–6 .................................................................. 41
Primary Third-Party Medical Insurance, Lines 7–12
........................................................................ 41
None/Uninsured (Line 7) ........................... 42
Medicaid (Line 8a) ..................................... 42
CHIP Medicaid (Line 8b) ........................... 42
Medicare (Line 9) ....................................... 43
Dually Eligible (Medicare and Medicaid) (Line
9a) ............................................................... 43
Other Public Insurance (Non-CHIP) (Line 10a)
.................................................................... 43
Other Public Insurance CHIP (Line 10b) ... 44
Private Insurance (Line 11) ........................ 44
Managed Care Utilization, Lines 13a–13c ..... 44
Member Months ......................................... 44
Special Populations, Lines 14–26 .................. 45

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
6 2023 UDS MANUAL | Table of Contents
Total Migratory and Seasonal Agricultural
Workers and Their Family Members, Lines 14–
16 ................................................................ 46
Total Patients Experiencing Homelessness, Lines
17–23 .......................................................... 46
Total School-Based Service Site Patients, Line
24 ................................................................ 48
Total Veterans, Line 25 .............................. 48
Total Patients Served at a Health Center Service
Delivery Site Located in or Immediately
Accessible to a Public Housing Site, Line 26..49
FAQ for Table 4 ............................................. 49
Table 4: Selected Patient Characteristics ........ 53
Table 4: Selected Patient Characteristics
(continued) ...................................................... 54
Instructions for Table 5: Staffing and Utilization
............................................................................ 55
Table 5: Staffing and Utilization .................... 55
Personnel Full-Time Equivalents (FTEs), Column
A ..................................................................... 55
Identifying Employment Type and Calculating
FTEs ........................................................... 56
Reporting FTEs on the Appropriate Line on
Table 5 ........................................................ 56
Personnel by Major Service Category ........ 57
Visits, Columns B and B2 .............................. 63
Clinic Visits, Column B ............................. 63
Virtual Visits, Column B2 .......................... 63
Visits Purchased from Non-Personnel Providers
on a Fee-For-Service Basis ......................... 64
Visit Considerations by Personnel Line ..... 65
DO NOT Report Visits or Patients for Services
Provided by the Following: ........................ 67
Patients, Column C ......................................... 67
Selected Service Detail Addendum ................ 68
Providers, Column A1 ................................ 69
Clinic Visits, Column B ............................. 69
Virtual Visits, Column B2 .......................... 69
Patients, Column C ..................................... 69
FAQ for Table 5 and Selected Service Detail
Addendum ...................................................... 69
Table 5: Staffing and Utilization .................... 74
Table 5: Staffing and Utilization (continued) . 75
Table 5: Selected Service Detail Addendum .. 76
Instructions for Table 6A: Selected Diagnoses and
Services Rendered ............................................ 77
Selected Diagnoses, Lines 1–20f.................... 77
Selected Diagnoses Visits and Patients, Columns
A and B ...................................................... 77
Selected Tests/Screenings, Lines 21–26e ....... 78
Selected Tests/Screenings Visits and Patients,
Columns A and B ....................................... 78
Dental Services, Lines 27–34 .........................
79
Den
tal Services Visits and Patients, Columns A
and B .......................................................... 79
Services Provided by Multiple Entities .......... 80
FAQ for Table 6A .......................................... 80
Table 6A: Selected Diagnoses and Services
Rendered ........................................................ 84
Selected Diagnoses ......................................... 84
Selected Services Rendered ........................... 86
Sources of Codes ............................................ 88
Instructions for Tables 6B and 7 ..................... 89
Column Logic Instructions ............................. 89
Column A (A, 2A, or 3A): Number of Patients in
the Denominator ......................................... 89
Column B (B, 2B, or 3B): Number of Records
Reviewed .................................................... 90
Column C (C or 2C) or 3F: Number of
Charts/Records Meeting the Numerator Criteria
.................................................................... 90
Criteria vs. Exceptions and Exclusions in
HITs/EHRs vs. Chart Reviews ................... 91
And vs. Or .................................................. 91
Detailed Instructions for Clinical Quality Measures
........................................................................ 91
Instructions for Table 6B: Quality of Care
Measures ........................................................... 92
Table 6B: Quality of Care Measures .............. 93

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
7 2023 UDS MANUAL | Table of Contents
Sections A and B: Demographic Characteristics of
Prenatal Care Patients ..................................... 93
Prenatal Care by Referral Only (check box)..93
Section A: Age of Prenatal Care Patients (Lines
1–6) ............................................................. 94
Section B: Early Entry into Prenatal Care (Lines
7–9), No eCQM .......................................... 94
Sections C through M: Other Quality of Care
Measures ......................................................... 96
Childhood Immunization Status (Line 10),
CMS117v11 ................................................ 96
Cervical Cancer Screening (Line 11),
CMS124v11 ................................................ 99
Breast Cancer Screening (Line 11a),
CMS125v11 .............................................. 100
Weight Assessment and Counseling for Nutrition
and Physical Activity for Children/Adolescents
(Line 12), CMS155v11 ............................. 101
Preventive Care and Screening: Body Mass
Index (BMI) Screening and Follow-Up Plan
(Line 13), CMS69v11 ............................... 102
Preventive Care and Screening: Tobacco Use:
Screening and Cessation Intervention (Line 14a),
CMS138v11 .............................................. 104
Statin Therapy for the Prevention and Treatment
of Cardiovascular Disease (Line 17a),
CMS347v6 ................................................ 106
Ischemic Vascular Disease (IVD): Use of Aspirin
or Another Antiplatelet (Line 18), CMS164v7
.................................................................. 107
Colorectal Cancer Screening (Line 19),
CMS130v11 .............................................. 108
HIV Linkage to Care (Line 20), No eCQM109
HIV Screening (Line 20a), CMS349v5 .... 111
Preventive Care and Screening: Screening for
Depression and Follow-Up Plan (Line 21),
CMS2v12 .................................................. 111
Depression Remission at Twelve Months (Line
21a), CMS159v11..................................... 113
Dental Sealants for Children between 6–9 Years
(Line 22), CMS277v0 ............................... 115
FAQ for Table 6B ......................................... 116
Table 6B: Quality of Care Measures ............ 121
Instructions for Table 7: Health Outcomes and
Disparities ....................................................... 125
Table 7: Health Outcomes and Disparities Measures
...................................................................... 125
Race and Ethnicity Reporting....................... 125
Section A: Deliveries and Birth Weight ....... 126
HIV-Positive Pregnant Patients, Top Line (Line 0)
...................................................................... 126
Deliveries Performed by Health Center Provider
(Line 2) ......................................................... 126
Deliveries and Birth Weight Data by Race and
Hispanic, Latino/a, or Spanish Ethnicity, Columns
1a–1d ............................................................ 126
Prenatal Care Patients and Referred Prenatal
Care Patients Who Delivered During the Year
(Column 1a) ............................................. 127
Birth Weight of Infants Born to Prenatal Care
Patients Who Delivered During the Year
(Columns 1b–1d) ...................................... 127
Sections B and C: Other Health Outcome and
Disparity Measures ....................................... 128
Controlling High Blood Pressure (Columns 2a–
2c), CMS165v11 ...................................... 129
Diabetes: Hemoglobin A1c (HbA1c) Poor
Control (>9.0 percent) (Columns 3a–3f),
CMS122v11 ............................................. 130
FAQ f
or Table 7 ........................................... 131
Table 7: Health Outcomes and Disparities ... 133
Instructions for Table 8A: Financial Costs .. 145
Table 8A: Financial Costs ............................ 145
Column Reporting Requirements ................. 145
Column A: Accrued Costs ........................ 145
Column B: Allocation of Facility Costs and Non-
Clinical Support Service Costs ................. 145
Column C: Total Cost After Allocation of
Facility and Non-Clinical Support Services..145
Cost Center Line Reporting Requirements .. 146
Medical Personnel Costs (Line 1) ............ 146
Medical Lab and X-Ray Costs (Line 2) ... 146
Other Direct Medical Costs (Line 3) ........ 146
Total Medical (Line 4) ............................. 147

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
8 2023 UDS MANUAL | Table of Contents
Other Clinical Services (Lines 5–10) ....... 147
Dental (Line 5) ......................................... 147
Mental Health (Line 6) ............................. 147
Substance Use Disorders (Line 7) ............ 147
Pharmacy (Not Including Pharmaceuticals) (Line
8a) ............................................................. 147
Pharmaceuticals (Line 8b) ........................ 148
Other Professional (Line 9) ...................... 148
Vision (Line 9a) ........................................ 148
Total Other Clinical (Line 10) .................. 148
Enabling (Lines 11a–11h, 11) .................. 149
Total Enabling Services (Line 11) ............ 149
Other Program-Related (Line 12) ............. 149
Quality Improvement (QI) (Line 12a) ...... 150
Total Enabling, Other Program-Related, and
Quality Improvement Services (Line 13) . 150
Facility Costs (Line 14) ............................ 150
Non-Clinical Support Services Costs (Line 15)
.................................................................. 150
Total Facility and Non-Clinical Support Services
(Line 16) ................................................... 151
Total Accrued Costs (Line 17) ................. 151
Value of Donated Facilities, Services, and
Supplies (Line 18, Column C) .................. 151
Total with Donations (Line 19) ................ 151
Column B: Facility and Non-Clinical Support
Services Allocation Instructions ................... 152
Facility ...................................................... 152
Non-Clinical Support Services ................. 152
FAQ for Table 8A ........................................ 153
Table 8A: Financial Costs ............................ 156
Instructions for Table 9D: Patient Service Revenue
.......................................................................... 158
Table 9D: Patient Service Revenue .............. 158
Rows: Payer Categories and Form of Payment158
Payer Categories ....................................... 158
Form of Payment ...................................... 160
Columns: Charges, Payments, and Adjustments
Related to Services Delivered ...................... 161
Column A: Full Charges This Period ....... 161
Column B: Amount Collected This Period..162
Columns C1–C4: Retroactive Settlements,
Receipts, or Paybacks ............................... 162
Column D: Adjustments ........................... 164
Column E: Sliding Fee Discounts ............ 164
Column F: Bad Debt Write-Off ............... 165
Tota
l Patient Service Revenue (Line 14) . 165
FAQ for Table 9D ........................................ 165
Table 9D: Patient Service Revenue .............. 168
Instructions for Table 9E: Other Revenue ... 170
Table 9E: Other Revenue ............................. 170
BPHC Grants ................................................ 170
Health Center Program Grants, Lines 1a Through
1e .............................................................. 170
Total Health Center Program (Line 1g) ... 171
Capital Development Grants (Line 1k) .... 171
COVID-19 Supplemental Funding ........... 171
Total BPHC Grants (Line 1) .................... 171
Other Federal Grants .................................... 171
Ryan White Part C—HIV Early Intervention
Grants (Line 2) ......................................... 171
Other Federal Grants (Line 3) .................. 172
Medicare and Medicaid EHR Incentive Grants
for Eligible Providers (Line 3a)................ 172
Provider Relief Fund (Line 3b) ................ 172
Total Other Federal Grants (Line 5) ......... 172
Non-Federal Grants or Contracts ................. 172
State Government Grants and Contracts (Line 6)
.................................................................. 172
State/Local Indigent Care Programs (Line 6a)
.................................................................. 173
Local Government Grants and Contracts (Line 7)
.................................................................. 173
Foundation/Private Grants and Contracts (Line 8)
.................................................................. 173
Total Non-Federal Grants and Contracts (Line 9)
.................................................................. 173
Other Revenue (Line 10) .......................... 173

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
9 2023 UDS MANUAL | Table of Contents
Total Other Revenue (Line 11) ................. 174
FAQ for Table 9E ......................................... 174
Table 9E: Other Revenues ............................ 176
Appendix A: Listing of Personnel ................. 177
Appendix B: Special Multi-Table Situations..182
Contracted Care (specialty, dental, mental health,
etc.) ............................................................... 183
Services Provided by a Volunteer Provider .. 184
Interns and Residents .................................... 184
Women, Infants, and Children (WIC) .......... 185
In-House Pharmacy or Dispensary Services for
Health Center Patients .................................. 186
In-House Pharmacy for Community (i.e., for non-
patients) ........................................................ 187
Contract Pharmacy Dispensing to Health Center
Patients, Generally Using 340B Purchased Drugs
...................................................................... 187
Donated Drugs, Including Vaccines ............. 188
Clinical Dispensing of Drugs ....................... 188
ADHC and PACE ......................................... 189
Medi-Medi/Dually Eligible .......................... 189
Certain Grant-Supported Clinical Care Programs:
BCCEDP, Title X, etc. ................................. 190
State or Local Indigent Care Programs ......... 190
Workers’ Compensation ............................... 190
Tricare, Trigon, Public Employees’ Insurance, etc.
...................................................................... 191
Contract Sites................................................ 191
The Children’s Health Insurance Program (CHIP)
...................................................................... 192
Carve-Outs .................................................... 192
Incarcerated Patients ..................................... 192
HIT/EHR Personnel and Costs ..................... 193
Issuance of Vouchers for Payment of Services..194
New Start or New Access Point (NAP) ........ 195
Relationship Between Personnel on Table 5 and
Costs on Table 8A ........................................ 195
Relationship Between Insurance on Table 4 and
Revenue on Table 9D ................................... 196
Relationship Between Prenatal Care on Table 6B
and Deliveries on Table 7 ............................. 196
Relationship Between Race and Ethnicity on Tables
3B and 7 ....................................................... 197
Appendix C: Reduced Number of Records
Reviewed for Clinical Quality Measure Reporting
.......................................................................... 199
Appendix D: Health Center Health Information
Technology (HIT) Capabilities ...................... 200
Introduction .................................................. 200
Questions ...................................................... 200
FAQ for Appendix D: Health Center HIT
Capabilities Form ......................................... 205
Appe
ndix E: Other Data Elements ............... 206
Introduction .................................................. 206
Questions ...................................................... 206
Appendix F: Workforce ................................. 208
Introduction .................................................. 208
Questions ...................................................... 208
Appendix G: De-Identified Patient-Level
Reporting ........................................................ 211
Introduction .................................................. 211
Scope of UDS+ ............................................ 211
Reporting UDS+ Data .................................. 211
Resources and Support for UDS+ Reporting 212
Appendix H: Health Center Resources ........ 214
UDS Production Timeline and Report Availability
...................................................................... 217
UDS CQMs and National Programs Crosswalk..218
Appendix I: Glossary ..................................... 220
Appendix J: Acronyms .................................. 225

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
10 2023 UDS MANUAL | Table of Contents
Changes to the Reporting Requirements
This section outlines critical reporting instruction changes made since the original 2023 calendar year release
(May 8, 2023) of this manual. Use the updated manual to prepare and submit the calendar year UDS Report.
• There are no changes at this time.
Major changes from the 2022 calendar year reporting to the 2023 calendar year reporting are included at the start
of each Table and Form instruction section and highlighted in honeycomb color for ease of locating.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
11 2023 UDS MANUAL | Introduction
Introduction
This manual describes the annual Uniform Data System (UDS) reporting requirements for all health centers that
receive federal award funds (“awardees”) under the Health Center Program authorized by section 330 of the
Public Health Service (PHS) Act (42 U.S.C. 254b
) (“section 330”), as amended (including sections 330(e), (g),
(h), and (i)), as well as for health centers considered Health Center Program look-alikes. Look-alikes DO NOT
receive regular federal funding under section 330 of the PHS Act (although they may receive funding during
public health emergencies, such as COVID-19), but meet the Health Center Program requirements for designation
under the program (42 U.S.C. 1395x(aa)(4)(A)(ii) and 42 U.S.C. 1396d(l)(2)(B)(ii)). Certain health centers
funded under the Health Resources and Services Administration’s (HRSA) Bureau of Health Workforce (BHW)
are also required to complete the UDS.
Unless otherwise noted, for the remainder of this manual the term “health center” will refer to all the entities listed
above that are required to submit a UDS Report.
ABOUT THE UDS
The UDS is a standard data set that is reported annually by each health center and, thus, provides consistent
information about health centers. This core set of information for the calendar year encompasses patient
characteristics, services provided, clinical processes and health outcomes, patients’ use of services, staffing, costs,
and revenues. It is the source of unduplicated data for the entire scope of services included in the grant or
designation for the calendar year. If the health center brings services or service delivery sites into scope of project
during the calendar year, the health center must include data from the period after the date of the scope change in
its UDS Report.
HRSA routinely reports these data and related analyses, making them available to health centers in HRSA’s
Electronic Handbooks (EHBs) and to the public through HRSA’s data.HRSA.gov website.
1
Please refer to
Appendix H: Health Center Resources for resources that may be helpful for completing the UDS Report.
WHAT THIS MANUAL INCLUDES
A gloss
ary of key terms is available in
Appendix
I.
Acronyms used throughout the UDS
Manual are defined in Appendix
J.
This manual includes reporting requirements and resources to assist with completion of the UDS Report and that
apply to the calendar year 2023 UDS Report due February 15, 2024.
Reporting requirements include the
approved UDS changes for the
calendar year. The 2023
Program
Assistance Letter (PAL)
provides an overview of major
changes.
UDS Patient-Level Submission
(UDS+) FHIR® R4 Implementation
Guide, for health centers to submit
certain UDS tables using HL7® FHIR
R4 application programming interface
(API), is described in Appendix G
.
A list of personnel by service category
and by job title who may be eligible to
produce countable “visits” for the UDS
is shown in Appendix A
.
Resources and supports to assist health
centers, including links to electronic
clinical quality measures (eCQMs), are
provided in Appendix H
.
Issues that affect multiple tables are
addressed in Appendix B
.
Reduced denominator considerations
for clinical quality measure reporting
are provided in Appendix C
.
1
In accordance with the Freedom of Information Act (Exemption 4), BPHC does not publicly share proprietary business information at the health center
level.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
12 2023 UDS MANUAL | General Instructions
General Instructions
WHAT TO SUBMIT
The UDS includes two parts that health centers submit through the EHBs:
1) All health centers use the Universal Report, which consists of the UDS tables, the Health Information
Technology (HIT) Form, the Other Data Elements Form, and the Workforce Form.
The Universal Report represents an unduplicated count of all patients served by the health center regardless of
funding source; the Grant Report represents a subset of patients reported on the Universal Report who are
served under a special population funding authority. Thus, no cell in a Grant Report may have a number
larger than the same cell in the Universal Report.
2) Health Center Program awardees that receive section 330 grants under multiple program funding authorities
(Community Health Center [CHC] [330(e)] program, Migrant Health Center [MHC] [330(g)] program,
Health Care for the Homeless [HCH] [330(h)] program, and/or Public Housing Primary Care [PHPC]
[330(i)]) also complete separate Grant Reports.
o The Grant Reports provide data comparable to the Universal Report for Tables 3A, 3B, 4, 6A, and part of
Table 5.
o Grant Reports are only completed for the portion of the program that falls within the scope of a project
funded under a particular funding authority.
o The vast majority of health centers have a CHC (330(e)) grant and to report a separate grant report would
add burden to health centers since the activity makes up a large portion of the Universal Report.
Therefore, awardees DO NOT submit a separate Grant Report for the scope of project supported under
the CHC (330(e)) program.
Report all the data for any patient who receives services under sections 330(g), (h), or (i) in the proper Grant
Report. Include all services provided to these patients regardless of the funding source.
The EHBs reporting system automatically identifies all the reports needed to meet the UDS reporting
requirements. Please contact Health Center Program Support through the BPHC Contact Form
or at 877-464-4772
if there appear to be errors.
WHAT IS INCLUDED
The UDS includes 11 tables and 3 forms that provide demographic, clinical, operational, and financial data.
Health centers must complete the following:
Table Data Reported
Universal
Report
Grant
Reports
Service Area Service Area
Service Area
Service
Area
Patients by ZIP Code Table:
Patients by ZIP Code
Patients served reported by ZIP code and by primary
third-party medical insurance source, if any
X
Not included in grant reports
Patient Profile Patient Profile
Patient Profile
Patient
Profile
Table 3A: Patients by Age and by
Sex Assigned at Birth
Patients by age and by sex assigned at birth X X
Table 3B: Demographic
Characteristics
Patients by race, ethnicity, language barriers, sexual
orientation, and gender identity
X X

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
13 2023 UDS MANUAL | General Instructions
Table Data Reported
Universal
Report
Grant
Reports
Table 4: Selected Patient
Characteristics
Patients by income (as measured by percentage of the
federal poverty guidelines [FPG]) and primary third-
party medical insurance; the number of “special
population” patients receiving services; and managed
care enrollment, if any
X X
Staffing and Utilization
Staffing and Utilization
Staffing and Utilization Staffing and Utilization
Table 5: Staffing and Utilization
The annualized full-time equivalent (FTE) of program
personnel by position, in-person and virtual visits by
provider type, and patients by service type
X
Partial
(excludes
FTE)
Table 5 Addendum: Selected
Service Detail Addendum
Mental health services provided by medical providers;
substance use disorder services provided by medical and
mental health providers
X
Not included in grant reports
Clinical
Clinical
Clinical Clinical
Table 6A: Selected Diagnoses and
Services Rendered
Visits and patients for selected medical, mental health,
substance use disorder, vision, and dental diagnoses and
services
X X
Table 6B: Quality of Care
Measures
Clinical quality-of-care measures X
Not included in grant reports
Table 7: Health Outcomes and
Disparities
Health outcome measures by race and ethnicity X
Not included in grant reports
Financial
Financial
Financial Financial
Table 8A: Financial Costs
Direct and indirect expenses by service categories
X
Not included in grant reports
Table 9D: Patient Service
Revenue
Full charges, collections, and adjustments by payer type;
sliding fee discounts; and patient bad debt write-offs
X
Not included in grant reports
Table 9E: Other Revenue
Other, non–patient service revenue
X
Not included in grant reports
Other
Other Form
Other Form Other Form
Appendix D: Health Information
Technology (HIT) Capabilities
Form
HIT capabilities, including the use of electronic health
record (EHR) information, and social risk factors
X
Not included in grant reports
Appendix E: Other Data Elements
Form
Medications for opioid use disorder (MOUD), telehealth,
and outreach and enrollment assistance
X
Not included in grant reports
Appendix F: Workforce Form
Health center workforce training and use of provider and
personnel satisfaction surveys
X
Not included in grant reports
Note: Grant reports are NOT completed for tables and forms grayed out in this table.
The UDS Support Center is available to provide training, technical assistance, and resources about the UDS data
and reporting requirements. Contact the Support Center at 1-866-UDS-HELP, [email protected], or
BPHC Contact Form.
CALENDAR YEAR REPORTING
Who Reports UDS What is Reported How to Report When to Report
• All health centers funded
or designated in whole or
in part, before October
1, 2023, including New
Access Point (NAP).
• Approved in-scope
activities from January
1 through December
31, 2023.
• Report even if no grant
funds were drawn down
for some or all programs
during the calendar year.
• Through the Electronic
Handbooks (EHBs)
starting January 1,
2024.
• Preliminary Reporting
Environment (PRE) and
offline tools are available
in Fall 2023.
• January 1 through
February 15, 2024.
UDS Reports are to be
submitted by February
15, 2024.
• UDS Report reviews are
conducted and necessary
revisions are made from
February 15 through
March 31, 2024.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
14 2023 UDS MANUAL | General Instructions
The UDS is a calendar year report. Health centers—including all those whose designation or funding begins,
either in whole or in part, after January 1—must report in-scope activities for the entire calendar year. Similarly,
health centers with a fiscal year or grant period other than January 1 to December 31 will still report on the
calendar year, NOT on their fiscal or grant year.
If the entire look-alike program became funded and converted to a 330 awardee before October 1, 2023, report
only an awardee UDS Report for the year.
Health centers whose designation or funding ends during the year should contact Health Center Program Support
via the BPHC Contact Form
or at 877-464-4772 to clarify their reporting requirements.
No UDS Report is filed if the health center was funded or designated for the first time on or after October 1 of the
calendar year.
IN-SCOPE REPORTING
All health centers must submit data that reflects all activities in the HRSA health center scope of project, as
defined in approved applications and reflected in the official Notice of Award/Designation.
For organizations that operate programs and/or service delivery sites that are out of scope, limit the reporting to
the approved scope of project only.
DUE DATES AND REVISIONS TO REPORTS
The period for submission of complete and accurate UDS Reports is January 1 through February 15, 2024, 11:59
p.m. local time.
From February 15 through March 31, 2024, a Health Center Program UDS Reviewer will review your report and,
as needed, assist you in ensuring that reported data adheres to reporting requirements. The UDS Reviewer sends
communications and data change requests through EHBs via a non-HRSA.gov email address to the health center
contact listed in the EHBs. Communicate directly with the assigned UDS Reviewer during this time to address
questions they have raised. Final, corrected submissions are due no later than March 31, 2024.
HRSA may grant a reporting exemption under extraordinary circumstances, such as the physical destruction of a
health center. Health centers must request such exemptions directly from BPHC via the BPHC Contact Form
or at
877-464-4772.
HOW AND WHERE TO SUBMIT DATA
All health centers are to submit a full UDS Report within EHBs by February 15, 2024. This will be the official
submission of record for 2023 reporting.
Beginning with the 2023 UDS reporting, in addition to an aggregate UDS Report submission within EHBs, health
centers may voluntarily submit de-identified patient-level data (UDS+) submitted using Health Level Seven
(HL7®) Fast Healthcare Interoperability Resources (FHIR®) standards version release 4 (R4) for UDS, for the
data elements on the following tables:
• Patients by ZIP Code Table
• Table 3A: Patients by Age and by Sex Assigned at Birth
• Table 3B: Demographic Characteristics
• Table 4: Selected Patient Characteristics
• Table 6A: Selected Diagnoses and Services Rendered

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
15 2023 UDS MANUAL | General Instructions
• Table 6B: Quality of Care Measures
• Table 7: Health Outcomes and Disparities
Health centers choosing to participate in this voluntary reporting will submit through (bulk) FHIR R4 APIs, using
the UDS+ FHIR R4 Implementation Guide (IG) as described in Appendix G
. To learn more about UDS+, please
refer to the FAQ for General Instructions.
Health center personnel need a username and password to log into the EHBs, which are then used to access,
complete, and submit the health center’s UDS Report. The EHBs supports the use of standard web browsers
2
and
provides electronic forms necessary to complete the Report. The Preliminary Reporting Environment (PRE)
3
provides early access to the EHBs and is available in the fall. This allows health centers to:
• enter available UDS data,
• identify potential data reporting errors, and
• provide additional preparation time to compile UDS data.
To facilitate a team-based approach, there are also offline reporting templates available within the EHBs. For
more information on these tools, visit the UDS Resources
web page.
Health centers are required to designate one person as the UDS contact. The UDS contact receives all
communications about the UDS Report. This person is responsible for ensuring that corrections to the report are
made, explanations of accurate data reported on the UDS tables are clear, and the report is submitted according to
set deadlines. Be sure the UDS contact information is updated in the EHBs in order to ensure receipt of
important UDS-related communications.
Health centers grant individual personnel “view” or “edit” privileges in the EHBs. These privileges apply to the
whole report, not just specific tables. Health centers may give edit privileges to several people, each using
separate login credentials. Health center personnel with EHBs access can work on the forms in sections, saving
interim or partial versions online as they work and returning to complete them later.
The EHBs saves user progress until the health center completes all tables, runs system checks on the data, and
makes a formal submission. The chief executive officer (CEO) or project director usually submits, but they may
delegate the authority to someone else by designating an alternate in the EHBs. At the time of submission, the
UDS requires the submitter to acknowledge that the health center reviewed and verified the accuracy and validity
of the data. Submit only completed reports into the EHBs. To ensure accuracy, the EHBs checks for potential
inconsistencies or questionable data. The system provides a summary of which tables are complete, as well as a
list of audit questions. Health center personnel must address each of the data audit findings, even if the audit
question does not appear to apply to their health center’s unique circumstances. If personnel believe the data are
correct as submitted, they should clearly explain any unique circumstances.
2
While most web browsers should work with the EHBs, it is certified to work with the browsers mentioned in the EHBs’ recommended settings, which are
available on the EHBs website.
3
Data present in the PRE on December 31 are automatically carried over to the annual UDS reporting environment, which opens January 1.
UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
16 2023 UDS MANUAL | General Instructions
Failure to submit a timely, accurate, and complete UDS Report by February 15, 2024, 11:59 p.m. (local
time) may result in a condition being placed on your grant award. Additional restrictions, including the
requirement that all drawdowns of Health Center Program grant award funds from the Payment Management
System (PMS) have the prior approval of the HRSA Division of Grants Management Operations (DGMO) and/or
limits on future funding (e.g., base adjustments), may also be placed on your grant award.
Note: Retain health center UDS reporting backup documentation and files for a minimum of 1 year or through a
date determined by the health center.
Please refer to Appendix H: Health Center Resources
for resources that may be helpful for completing the UDS
Report.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
17 2023 UDS MANUAL | General Instructions
FAQ FOR THE GENERAL INSTRUCTIONS
1. Do we report only the services provided to patients using HCH, MHC, or PHPC grant funds on the
Grant Report?
No. Include activity for all patients described in the approved HCH, MHC, or PHPC grant scope of project,
regardless of the funding source. For example, if patients experiencing homelessness receive medical services
in the 330(h)-supported homeless medical van, report this activity on the Homeless Grant Report tables. If
patients experiencing homelessness receive dental services at the clinic, where 330(h) funds are not used, this
activity would also be reported on the Homeless Grant Report tables regardless of the dental funding source.
2. When do we complete a Universal Report and when do we complete a Grant Report?
In summary, health centers that receive funds under only one BPHC Health Center Program award complete
the Universal Report and no Grant Reports (CHC only, HCH only, MHC only, or PHPC only). Health centers
funded through multiple BPHC funding authorities complete a Universal Report for the combined projects
and a separate Grant Report for activity covered by their MHC, HCH, and/or PHPC program grant(s).
Examples include the following:
• A CHC awardee that also has HCH funding completes a Universal Report for all in-scope activity and a
Grant Report for activity under the HCH program, but it does NOT complete a Grant Report for the CHC
funding.
• A CHC awardee that also has MHC and HCH funding completes a Universal Report, a Grant Report for
the HCH program, and a Grant Report for the MHC program.
• An HCH awardee that also receives PHPC funding completes a Universal Report and two Grant
Reports—one for the HCH program and one for the PHPC program.
• An HCH awardee that receives no other Health Center Program funding will file a Universal Report and
will NOT file a Grant Report.
3. We had a service delivery site that closed and is no longer in-scope. Do we report data from the service
delivery sites or services that are removed from scope of project in the UDS Report?
Yes. If services or service delivery sites are removed from your scope of project during the calendar year,
report on all activities (visits, personnel, revenue, etc.) up until the date they were acknowledged as being
removed from the change in scope (CIS).
4. We added a new service delivery site to our scope of project. What should we do to report the activity
of this new service delivery site on the UDS Report?
Health centers must submit data for all in-scope activities as reflected in the official Notice of
Award/Designation when a new service delivery site is added. If your health center added a new service
delivery site either through a CIS request or through an NAP award, you will be required to submit data for
in-scope activities based on your CIS approval date and/or NAP site implementation date.
5. What is UDS+?
The UDS Patient-Level Submission (UDS+) is a redesigned section of the UDS Report that enhances existing
patient-oriented tables (Patients by ZIP Code Table and Tables 3A, 3B, 4, 6A, 6B, and 7), reported in
aggregate at the health center level, with de-identified patient-level data. For the 2023 UDS Report
submission, patient-level data reporting is optional, but encouraged. This voluntary reporting will help health
centers and HRSA better understand challenges and successes with data submission and the impact of patient-
level reporting on final UDS reports. Once fully implemented, UDS+ aims to advance the utility of UDS data
and to reduce the annual reporting burden by aligning with interoperability standards and reporting
requirements used across the U.S. Department of Health and Human Services and health care industry.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
18 2023 UDS MANUAL | General Instructions
UDS+ data will be reported to HRSA using Fast Healthcare Interoperability Resources (FHIR®) R4, which is
a next-generation interoperability standard created by the standards development organization Health Level
Seven (HL7®). FHIR R4 is designed to enable health data, including clinical and administrative data, to be
quickly and efficiently exchanged.
The UDS+ FHIR R4 Implementation Guide (IG) defines the set of rules by which health centers can report
the UDS+ data to HRSA using de-identified patient data using FHIR R4 APIs. The UDS+ FHIR R4 IG
provides well-defined capability statements, FHIR R4 operations, FHIR R4 profiles, FHIR R4 extensions and
terminology needed to successfully implement UDS+.
Additionally, the UDS+ FHIR R4 IG will align HRSA reporting requirements with the Office of the National
Coordinator for Health Information Technology (ONC) and Centers for Medicare & Medicaid Services
(CMS) regulations to the extent possible.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
19 2023 UDS MANUAL | Instructions for Tables
Instructions for Tables that Report Visits, Patients, and
Providers
Health centers serve many individuals in different ways. NOT all individuals, encounters, and health center
personnel will count in the UDS Report. The following section defines countable visits, patients, and providers for
the UDS.
COUNTABLE VISITS
Visits determine who to count as a patient on the Patients by ZIP Code Table and Tables 3A, 3B, 4, 5, 6A, 6B,
and 7. Report visits by type of provider on Table 5 and for selected diagnoses and selected services on Table 6A.
Countable visits are encounters between a patient and a licensed or credentialed provider who exercises
independent professional judgment in providing services that are:
• documented,
• individual,
4
• in-person or virtual.
5
Count only visits that meet all these criteria.
Services must be provided by an individual classified as a “provider” for purposes of providing countable visits.
Not all health center personnel who interact with patients qualify as a provider, and not all services by a provider
are countable visits. See
Services and Individuals NOT Reported on the UDS Report. Appendix A provides a list
of health center personnel and the usual status of each as a provider or non-provider for UDS reporting purposes.
Visits provided by contractors and paid for by or billed through the health center are counted in the UDS if
they meet all other criteria. These include migrant voucher visits, as well as outpatient or inpatient specialty care
associated with an at-risk managed care contract. In these instances, if the visit is not documented in the patient’s
health record, a summary of the visit (rather than the complete record) must appear in the patient’s health record,
including all appropriate documentation and coding. Generally, at a minimum, this will include procedure and
diagnosis codes.
Below are definitions and criteria for reporting visits. Table 5 provides further clarifications. See
Clinic Visits,
Column B.
Documentation
Health centers must record the service and associated patient information, in print or electronic form, in a system
that permits ready retrieval of current data for the patient. The patient health record does not have to be complete
to meet this standard.
4
An exception is allowed for behavioral health visits, which may be conducted in a group setting.
5
Only interactive, synchronous audio and/or video telecommunication systems that permit real-time communication between a distant provider and a
patient may be considered and coded as telemedicine services. The term “telehealth” includes telemedicine services but encompasses a broader scope of
remote health care services. Telemedicine is specific to remote clinical services, whereas telehealth may include remote non-clinical services, such as
provider training, administrative meetings, and continuing medical education, in addition to clinical services.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
20 2023 UDS MANUAL | Instructions for Tables
Independent Professional Judgment
Providers must be acting on their own, not assisting another provider, when serving the patient.
Independent professional judgment is the use of the professional skills gained through formal training and
experience and unique to that provider or other similarly or more intensively trained providers.
Behavioral Health Group Visits
Behavioral health (mental health or substance use disorder) visits are the only type of visit that may be counted
when conducted in a group setting. A health center may count visits by a behavioral health provider who provides
services to a group of patients simultaneously only if the service is documented in each patient’s health record.
Examples of “group visits” include family therapy or counseling sessions, group mental health counseling, and
group substance use disorder counseling where several people receive services that are documented in each
patient’s health record.
Other considerations:
• The health center normally records applicable charges for each patient, even if another grant or contract
covers the costs.
• If only one patient is billed (for example, when a family member who is not the patient participates in a
patient’s counseling session), count the visit for only that one patient.
• When a behavioral health provider conducts services via telemedicine, the provider can be credited with a
visit only if the service is documented in the patient’s health record. The session will normally be billed to the
patient or a third party.
• DO NOT count group medical visits.
Location of Services Provided
A visit must take place in health centers’ approved service delivery sites (e.g., clinics, schools, homeless shelters,
as listed on Form 5B
) or in other locations that DO NOT meet HRSA’s site criteria but are included in the health
center’s scope of project (e.g., hospitals, nursing homes, extended care facilities, patient’s home), as referenced on
Form 5C. In addition, virtual visits may occur from other locations. See instructions for Virtual Visits.
Inpatient visit considerations:
• Only count one inpatient visit per patient per day, regardless of how many clinic providers see the patient or
how often they do so.
• Visits also include encounters with an existing patient who has been hospitalized, when health center medical
personnel “follow” the patient during the hospital stay as the provider of record or when they provide care to
the patient on behalf of the provider of record. This applies when the health center pays their medical
personnel who “follow” patients (or insurance) for the specific service.
• When a patient’s first encounter is in a hospital, in respite care, or in a similar facility that is not specifically
approved in Form 5B as a service delivery site under the scope of the Health Center Program, none of the
services for that patient are counted in the UDS.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
21 2023 UDS MANUAL | Instructions for Tables
Counting Multiple Visits by Category of Service
Multiple visits may occur when a patient has more than one visit with the health center in a day (in-person and/or
virtual).
Count only one visit per patient per service category
per provider per location in a single day, regardless of the
types or number of services provided or where they occur, as described in the table that follows.
Other considerations:
• If multiple medical providers in a single category deliver multiple services to a patient on a single day, count
only one visit, even if third-party payers may recognize these as separate billable services. This is typically
credited to the provider performing the highest level of or most care, although the health center needs to make
this determination for itself.
• Count two visits in a scenario in which services are periodically provided to a patient by two different
providers of the same service category type who are located at two different service delivery sites on the
same day. This permits patients who are in challenging environments (e.g., in parks or migrant camps) to
receive services outside the health center from a licensed or credentialed health center provider and receive
services again on the same day at the health center from a different licensed or credentialed provider.
• A virtual visit may count as a separate visit when a patient has another visit on the same day only if the
providers are different and the assigned service delivery location of each provider is different.
Maximum Number of Visits per Patient per Day per Service Category at the Same Service Delivery Site
# of Visits
Service Category
Provider Examples
1 Medical
physician, nurse practitioner, physician assistant, certified
nurse midwife, nurse
1
Dental
dentist, dental hygienist, dental therapist
1 Mental health
psychiatrist, licensed clinical psychologist, licensed clinical
social worker, psychiatric nurse practitioner, other licensed or
unlicensed mental health providers
1 Substance use disorder
alcohol and substance use disorder specialist, psychologist,
social worker
1 for each provider type
Other professional
nutritionist, podiatrist, speech therapist, acupuncturist
1
Vision
ophthalmologist, optometrist
1 for each provider type
Enabling
case manager, health educator
PATIENT
Patients are people who have at least one countable visit during the calendar year. The term “patient” applies
to everyone who receives clinic (in-person) or virtual visits, NOT just those who receive medical or dental
services.
The Universal Report includes all patients who had at least one visit during the calendar year within the scope of
project supported by the health center grant or designation.
• Report these patients and their visits on Tables 5 and 6A for each type of service (e.g., medical, dental,
enabling) received during the calendar year.
• On the Patients by ZIP Code Table, on Tables 3A and 3B, in each section of Tables 4 and 5, and for each
service on Table 6A, count each patient once and only once. This applies even if they received more than one

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
22 2023 UDS MANUAL | Instructions for Tables
service (e.g., medical, dental, enabling) or received services supported by more than one program authority
(i.e., section 330(g), section 330(h), section 330(i)).
For each Grant Report, patients reported are those who had at least one countable visit during the calendar year
within the scope of project activities supported by the specific section 330 program authority, even if the specific
service is not paid for by the grant. The number of patients reported in any cell on the Universal Report includes
all patients reported in the same cell in the Grant Report.
Services and Individuals NOT Reported on the UDS Report
Some services DO NOT count as a visit for UDS reporting, even though they are critical to the overall provision
of care to an individual or a community.
Someone who only receives one of the services described below is not a patient for purposes of UDS reporting.
If an individual receives additional services that require independent professional judgment from a health center
provider and the services are documented, they should be considered a patient of the health center.
The following situations are NOT countable visits:
Health
screenings or
outreach
services
• Do not count screenings (e.g., COVID-19, blood pressure, diabetes) as countable visits, including:
• Information sessions for prospective patients; health presentations to community groups;
information presentations about available health services at the center; services conducted at
health fairs or schools; immunization drives; services provided to groups, such as dental
varnishes or sealants provided at schools; hypertension or diabetes testing; or similar public
health efforts that frequently occur as part of community activities that involve conducting
outreach or group education.
Group
visits
• Do not count visits conducted in a group setting, except for behavioral health group visits.
• The most common non-behavioral health group visits are patient education or health
education classes (e.g., people with diabetes learning about nutrition).
Tests and
other ancillary
services
• Do not count services required to perform such tests, such as drawing blood or collecting urine,
and other ancillary services, including:
• Laboratory tests (including COVID-19, purified protein derivatives [PPDs], pregnancy, or
Hemoglobin A1c [HbA1c].
• Measuring and imaging (including blood pressure, height, weight, sonography, radiology,
mammography, retinography, or computerized axial tomography).
Dispensing or
administering
medications
• Do not count dispensing medications, including dispensing from a pharmacy or administering
medications (such as buprenorphine or warfarin).
• Do not count giving any injection (including for immunizations, vaccines, COVID-19, flu, allergy
shots, or family planning), regardless of education provided at the same time.
• Do not count providing narcotic agonists or antagonists or mixes of these, regardless of whether
the patient is assessed at the time of the dispensing and regardless of whether these medications
are dispensed regularly.
Health status
checks
• Do not count follow-up tests or checks (such as patients returning for HbA1c tests or blood
pressure checks).
• Do not count wound care (which is follow-up to the original primary care visit).
• Do not count taking health histories.
• Do not count making referrals for or following up on external referrals.
Services under the
Women, Infants, and
Children Program
• Do not count a person whose only contact with a health center is to receive services (including
nutrition) under a Women, Infants, and Children (WIC) program.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
23 2023 UDS MANUAL | Instructions for Tables
PROVIDER
A provider exercises independent professional judgment in the provision of services rendered to the patient,
assumes primary responsibility for assessing and/or treating the patient for the care provided at the visit, and
documents services in the patient’s health record.
• Only one provider receives credit for a visit, even when two or more providers are present and participate.
• If two or more providers of the same type share the services for a patient, only one provider receives credit for
a visit (see Counting Multiple Visits by Category of Service
).
• In cases where a preceptor (or attending physician) is following and supervising a licensed resident, the
resident receives credit. (See Appendix B
for further instruction on counting interns and residents.)
• When health center personnel are following a patient in the hospital, the primary health center personnel in
attendance during the visit is the provider who receives credit for the visit, even if other personnel are present.
• Except for physicians and dentists, allocate personnel by function among the major service categories based
on time dedicated to other positions.
• Report physicians according to the specialty in which they are board certified. If a physician has multiple
board certifications, report each physician under the specialty in which they are functioning. FTE and visits
for physicians with multiple board certifications should be allocated according to the specialty they are
practicing.
• Appendix A
provides a listing of personnel. Only personnel designated as a “provider” can generate countable
visits for purposes of UDS reporting.
• Table 5 provides further clarifications to these definitions. See Instructions for Table 5: Staffing and
Utilization.
• Providers may be employees of the health center, contracted personnel, or volunteers.
• Contracted providers who are paid for their time by the health center with grant funds or program income and
who are part of the scope of project, serve center patients, and document their services in the health center’s
records count as providers, and their FTE is reported.
• Contracted providers who are paid for specific visits or services with grant funds or program income and
report patient visits to the direct recipient of a BPHC or BHW grant or designation (e.g., under a migrant
voucher program or of HCH awardees with sub-awardees) are providers. The direct recipient of the BPHC or
BHW grant or designation reports these providers’ activities. Since such providers often have no time basis in
their report, no FTE would be reported for them if time data were not separately collected.
• Providers who volunteer to serve patients at the health center’s service delivery sites under the supervision of
the health center’s personnel and document their services and time in the center’s records are counted and
their FTE is reported.
• Individuals or groups who provide services under formal agreement or contract when the health center DOES
NOT pay for the visit are not credited as providing a health center visit, unless they are working at an
approved service delivery site under the supervision of the appropriate health center personnel and are
credentialed by the health center. These providers are generally providing services noted in Column III of the
grant scope of project application Form 5A
.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
24 2023 UDS MANUAL | Instructions for Tables
FAQ FOR THE INSTRUCTIONS FOR TABLES
1. What level of documentation is required for emergency, hospital, or respite services? Can we count the
visit if the record is incomplete?
A patient receiving documented emergency services counts even if some portions of the patient health record
are incomplete. Providers who see their established patients at a hospital or respite care facility and make a
note in the institutional file can satisfy this criterion by including a summary discharge or interim note
showing activities for each of the visit dates.
2. Do we credit a visit to the nurse assisting a physician?
No. A nurse assisting a physician during a physical examination by taking vital signs, recording a history, or
drawing a blood sample does not receive credit as a separate visit. Eligible medical visits usually involve one
of the “Evaluation and Management” billing codes (99202–99205 or 99211–99215) or one of the health
maintenance codes (99381–99387, 99391–99397).
3. Two different medical providers treated the patient at the health center on the same day. Can we count
both?
No. Only count one visit per service category when care is provided at the same location. For example, only
count one medical visit if an obstetrician/gynecologist (OB/GYN) provides prenatal care to a patient at the
health center and a nurse practitioner treats that same patient’s hypertension at the same location on the same
day. Other examples may include: a family physician and a pediatrician who both see a child or a dental
hygienist and a dentist who both see a patient on the same day.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
25 2023 UDS MANUAL | Instructions for ZIP Codes
Instructions for Patients by ZIP Code Table
The Patients by ZIP Code Table collects data on patients’ geographic residence by ZIP code
6
and by primary
medical insurance.
In addition to submitting this table as described below within the EHBs, health centers may voluntarily submit de-
identified patient-level report data using Health Level Seven (HL7®) Fast Healthcare Interoperability Resources
(FHIR®) R4 standards for this table.
PATIENTS BY ZIP CODE
• All health centers must report the number of patients served by ZIP code and medical insurance.
• This information enables BPHC to better identify areas served by health centers, service area overlaps, and
possible areas of unmet need.
• Patients may be mobile during the calendar year; report patients’ most recent ZIP code on file.
• ZIP code information is to be updated each calendar year.
ZIP Code of Specific Groups
For health centers serving patients without residence information, such as individuals from transient groups,
follow the instructions below:
Patients
experiencing
homelessness
• Report the service location ZIP code as a proxy when a ZIP code location is unavailable.
• If the patient receives services in a mobile health center van and has no other ZIP code, report the
ZIP code of the van’s location on the day of that visit.
• If the patient is living in permanent supportive housing or doubled up, report that location as the
ZIP code.
• Although it is appropriate from a clinical and service delivery perspective to collect the address of
a contact person to facilitate communication with the patient; DO NOT use the contact person’s
address as the patient’s address.
Patients who are
migratory
agricultural
workers
• Report the ZIP code of where the patient lived when they received care from the health center.
Migratory agricultural workers (as opposed to seasonal workers) may have both a temporary
address, where they live when working, as well as a permanent or “downstream” address.
• Report the ZIP code for the location (fixed service delivery site or mobile camp) where patients
received services, for those whose ZIP code is unavailable (e.g., living in cars or on the land).
Patients who are
foreign nationals
• Report the current ZIP codes for people from other countries who reside in the United States
either permanently or temporarily.
• Report “Other ZIP Code” in cases where patients have a permanent residence outside the country,
if they have no temporary address in the United States.
Unknown ZIP Code
Report residence in the “Unknown” category for patients whose residence is not known or for whom a proxy ZIP
code is not available.
6
The geographic residence of patients served during the calendar year comprises the health center service area and should align with the ZIP codes recorded
in the health center scope of project.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
26 2023 UDS MANUAL | Instructions for ZIP Codes
Ten or Fewer Patients in ZIP Code
To ease the burden of reporting, combine and report patients from ZIP codes with 10 or fewer patients in the
“Other ZIP Codes” category.
INSTRUCTIONS FOR TYPE OF INSURANCE
• Report primary medical insurance for all patients, regardless of the services they receive. This even applies
to patients who did not receive medical care, such as dental-only or behavioral health-only patients, as well as
patients whose medical insurance did not cover the service.
• Report on patients’ origin by their primary medical insurance.
• Report children served in school-based service sites only if they have complete clinic intake forms that show
insurance status and family/household income.
• DO NOT report children as uninsured unless they are receiving minor consent services or their family is
uninsured.
• DO NOT report patients as uninsured simply because they are receiving a service that is not covered by health
insurance.
Insurance Categories
Report the patient’s primary medical insurance covering medical care, if any, as of their last visit during the
calendar year.
Primary medical insurance is the insurance plan that the health center would typically bill first for medical
services, even if that insurance only pays for a portion of the visit.
The categories for this table are slightly different from those on Table 4; they combine Medicaid, Children’s
Health Insurance Program (CHIP), and Other Public into one category. Specific rules guide reporting:
• Report patients who have both Medicare and Medicaid
(dually eligible) as Medicare patients, because
Medicare is billed before Medicaid. The exception to the Medicare-first rule is the Medicare-enrolled patient
who is still working and insured by both an employer-based plan and Medicare. In this case, the primary
health insurance is the employer-based plan, which is billed first.
• Report Medicare administered by a private insurance company as Medicare.
• Report Medicaid and CHIP
patients enrolled in a managed care program administered by a private insurance
company as Medicaid/CHIP/Other Public.
• Report the patient by their medical insurance, even if the health center does not bill to the specified insurance.
• Report any third-party insurance that patients carry. Section 330 grant awards used to serve special
populations (e.g., MHC, HCH, PHPC) are NOT a form of medical insurance.
• Report patients who are incarcerated as Uninsured (whether they were seen in the correctional facility or at
the health center), unless Medicaid or other insurance covers them, and at the ZIP code of the jail or prison.
• In instances where patients are in residential drug programs, college dorms, military barracks, etc., report the
patient as living at the ZIP code of the residential program, dorm, or barrack and by their primary medical
insurance, NOT as Uninsured.
• Report patients whose care is subsidized by state or local government indigent care programs as Uninsured.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
27 2023 UDS MANUAL | Instructions for ZIP Codes
• Report patients who received insurance through the Health Insurance Marketplace as Private.
• Affordable Care Act subsidies (i.e., cost-sharing premium reductions and premium tax credits) DO NOT
affect insurance categories. Classify patients by their third-party insurer.
FAQ FOR PATIENTS BY ZIP CODE TABLE
1. Do we need to collect information and report on the ZIP code of all our patients?
Yes. Although health centers report residence by ZIP code for all patients, some centers may draw patients
from many ZIP codes outside of their normal service area. To ease the burden of reporting, consolidate ZIP
codes with 10 or fewer patients in the “Other” category.
2. Do we need to collect information and report on the primary medical insurance of all our patients?
Yes. Although the ZIP code of a patient may be Unknown, medical insurance information must be obtained
for every individual counted as a patient.
3. If a patient did not receive medical care, do we still need their medical insurance information? What
about dental patients?
Yes. This information is about patients’ primary medical insurance resources, not billing. Obtain medical
insurance information for all patients, even dental-only patients. For example, if a patient received only
mental health services, still determine whether they have primary medical insurance and report it.
4. How do we report patients by insurance when we DO NOT bill that form of insurance?
All patients must be asked for their primary medical insurance, although it may be explained to them that this
is required for planning purposes and that their insurance will not be billed. Report the patient by their
primary medical insurance, even in those instances that the health center does not or cannot bill to that
insurance. Include, for example, patients enrolled in managed care Medicaid but assigned to another primary
care provider, or patients with private insurance for which the health center’s providers have not been
credentialed.
5. How do we report patients by insurance who have their care subsidized by an indigent care program?
Report patients as Uninsured when their care is subsidized by a state or local government indigent care
program. Examples include New Jersey’s Uncompensated Care Program, New York’s Public Goods Pool
Funding, and Colorado’s Indigent Care Program.
6. Does the number of patients reported by ZIP code need to equal the total number of unduplicated
patients reported on Tables 3A, 3B, and 4?
Yes. Several tables and sections must match:
• The total number of patients reported by ZIP code (including Unknown and Other) on the Patients by ZIP
Code Table must equal the number of total unduplicated patients reported on Table 3A and sections of
Tables 3B and 4.
• The insurance totals reported on the Patients by ZIP Code Table must equal insurance reported on Table
4. Specifically:
o The total for Patients by ZIP Code Table Column B (Uninsured) must equal Table 4, Line 7, Columns
A + B.
o The total for Patients by ZIP Code Table Column C (Medicaid/CHIP/Other Public) must equal the
sum of Table 4, Line 8, Columns A + B and Line 10, Columns A + B.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
28 2023 UDS MANUAL | Instructions for ZIP Codes
o The total for Patients by ZIP Code Table Column D (Medicare) must equal Table 4, Line 9, Columns
A + B.
o The total for Patients by ZIP Code Table Column E (Private) must equal Table 4, Line 11, Columns
A + B.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
29 2023 UDS MANUAL | Instructions for ZIP Codes
PATIENTS BY ZIP CODE TABLE
Calendar Year: January 1, 2023, through December 31, 2023
ZIP Code
(a)
None/
Uninsured
(b)
Medicaid/
CHIP/Other Public
(c)
Medicare
(d)
Private
(e)
Total
Patients (f)
[Blank for demonstration]
[Blank for demonstration]
[Blank for demonstration]
[Blank for demonstration]
[Blank for demonstration]
[Blank for demonstration]
[Blank for demonstration]
[Blank for demonstration]
[Blank for demonstration]
[Blank for demonstration]
[Blank for demonstration]
[Blank for demonstration]
Other ZIP Codes
[Blank for demonstration]
[Blank for demonstration]
[Blank for demonstration]
[Blank for demonstration]
[Blank for demonstration]
Unknown Residence
[Blank for demonstration]
[Blank for demonstration]
[Blank for demonstration]
[Blank for demonstration]
[Blank for demonstration]
Total
[Blank for demonstration]
[Blank for demonstration]
[Blank for demonstration]
[Blank for demonstration]
[Blank for demonstration]
Note: The actual online output from the EHBs will display ZIP codes entered by the health center in Column A.
Patients by ZIP Code Table Cross-Table Considerations:
• Patien
ts by ZIP Code Table and Tables 3A, 3B, and 4 describe the same patients and the totals must be equal.
• The number of patients by insurance source reported on the Patients by ZIP Code Table must be consistent
with the number of patients by insurance category reported on Table 4.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
30 2023 UDS MANUAL | Instructions for Tables 3A and 3B
Instructions for Tables 3A and 3B
Tables 3A and 3B collect demographic data (age, sex, race, ethnicity, language, sexual orientation, and gender
identity) for patients who accessed services during the calendar year. This information must be collected from
patients initially as part of the patient registration or intake process and updated or confirmed annually thereafter.
Table 3A: Patients by Age and by Sex Assigned at Birth
Table 3A provides an unduplicated count of each patient’s age and sex assigned at birth.
In addition to submitting this table as described below within the EHBs, health centers may voluntarily submit de-
identified patient-level report data using Health Level Seven (HL7®) Fast Healthcare Interoperability Resources
(FHIR®) R4 standards for this table.
• Report the number of patients by appropriate categories for age and sex assigned at birth.
• Use the individual’s age on December 31, 2023.
• Report patients according to their sex assigned at birth or sex reported on their birth certificate.
• Report the date of birth and sex listed on the birth certificate for all patients. There is no “Unknown” category
on this table.
Note: On the non-prenatal portions of Tables 6B and 7, age is defined differently by measure. Thus, the numbers
on Table 3A may not be the same as those on Tables 6B and 7 even if all the patients at a health center were
medical patients, though they will usually be similar.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
31 2023 UDS MANUAL | Instructions for Tables 3A and 3B
Table 3B: Demographic Characteristics
Table 3B provides an unduplicated count of patients by demographic characteristics.
• In addition to submitting this table as described below within the EHBs, health centers may voluntarily
submit de-identified patient-level report data using Health Level Seven (HL7®) Fast Healthcare.
Interoperability Resources (FHIR®) R4 standards for this table.
• This table has been updated to include sub-categories for Asian and Other Pacific Islander, as well as broader
selection for ethnicity by including further Hispanic, Latino/a, or Spanish origin sub-categories.
Report the number of patients by their self-identified race, ethnicity, language preference, sexual orientation, and
gender identity.
PATIENTS BY HISPANIC, LATINO/A, OR SPANISH ETHNICITY AND RACE (LINES 1–8)
Table 3B displays the race and ethnicity of the patient population in a matrix format. This allows for reporting on
the racial and ethnic identification of all patients.
Hispanic, Latino/a, or Spanish Ethnicity
Table 3B collects information on whether or not patients consider themselves to be of Hispanic, Latino/a, or
Spanish ethnicity, regardless of their race.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
32 2023 UDS MANUAL | Instructions for Tables 3A and 3B
Column A
(Hispanic, Latino/a, or Spanish
Origin)
Column B
(Not Hispanic, Latino/a, or Spanish
Origin)
Column C
(Unreported/Chose Not to Disclose
Ethnicity)
• Report the number of patients of
Mexican, including Mexican
American and Chicano/a (Column
a1), Puerto Rican (Column a2),
Cuban (Column a3), another
Spanish culture or origin (Column
a4), or Hispanic, Latino/a, or
Spanish origin combined (Column
a5), broken out by their racial
identification. Include in this count
Hispanic, Latino/a, or Spanish
origin patients born in the United
States.
• Report patients who are of
Hispanic, Latino/a, or Spanish
origin but for whom granularity of
ethnicity is not known, as well as
patients who select more than one
ethnicity, in Column a5 (e.g.,
Mexican and Puerto Rican).
• Report patients who self-report as
being of Hispanic, Latino/a, or
Spanish ethnicity but DO NOT
separately select a race on Line 7,
as “Unreported/Chose not to
disclose race.” Health centers
should not default these patients to
any other category.
• DO NOT include patients from
Portugal, Brazil, or Haiti whose
ethnicity is not otherwise tied to the
Spanish language.
• Report the number of patients who
indicate that they are NOT of
Hispanic, Latino/a, or Spanish
origin.
• If a patient self-reported a race but
has not made a selection for the
Hispanic/Not Hispanic, Latino/a, or
Spanish origin question, presume
that the patient is NOT of Hispanic,
Latino/a, or Spanish origin.
• Report on Line 7 only those
patients who left the entire race and
Hispanic, Latino/a, or Spanish
ethnicity part of the intake form
blank or those who indicated that
they choose not to disclose these
data. Only one cell is available in
this column.
Note: Column C is grayed out on
all race lines except for the
“Unreported/Chose not to disclose
race” line.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
33 2023 UDS MANUAL | Instructions for Tables 3A and 3B
Race
All patients must be classified in one of the racial categories.
• Report patients in one of 16 race categories:
o Line 1, Asian, as Asian Indian (Line 1a), Chinese (Line 1b), Filipino (Line 1c), Japanese (Line 1d),
Korean (Line 1e), Vietnamese (Line 1f), or Other Asian (Line 1g)
o Line 2, Native Hawaiian/Other Pacific Islander, as Native Hawaiian (Line 2a), Other Pacific Islander
(Line 2b), Guamanian or Chamorro (Line 2c), or Samoan (Line 2d)
o Line 3, Black/African American
o Line 4, American Indian/Alaska Native
o Line 5, White
o Line 6, More than one race
o Line 7, Unreported/Chose not to disclose race
• Patients sometimes categorized as “Asian/Asian American/Pacific Islander” in other systems are reported on
the UDS in one of five distinct categories:
o Line 1, Asian: Patients having ancestry in any of the original peoples of Asia, Southeast Asia, or the
Indian subcontinent including, for example, Cambodia, China, India, Japan, Korea, Malaysia, Pakistan,
the Philippine Islands, Indonesia, Thailand, or Vietnam. Include in the Other Asian category patients who
are Asian, but for whom the granularity of their race is not known.
o Line 2a, Native Hawaiian: Patients having ancestry in any of the original peoples of Hawai’i.
o Line 2b, Other Pacific Islander: Patients having ancestry in any of the original peoples of Tonga, Palau,
Chuuk, Yap, Kosrae, Ebeye, Pohnpei, or other Pacific Islands in Melanesia or Oceana. Include in the
Other Pacific Islander category patients who are of other Pacific islands, but for whom the granularity of
their race is not known.
o Line 2c, Guamanian or Chamorro: Patients having ancestry in any of the original peoples of the
Northern Mariana Islands, Guam, Saipan, Tinian, Rota, or other Mariana Islands in Micronesia.
o Line 2d, Samoan: Patients having ancestry in any of the original peoples of the Samoan Islands, Savai’i,
Manono, Upolu, Tutuila, Pola Island, Aunu’u, or other Samoan Islands in American Samoa or Polynesia.
• Report patients who trace their ancestry to any of the original peoples of North, South, and Central America
and who maintain tribal affiliation or community attachment on Line 4, American Indian/Alaska Native.
• Line 6, More than one race: Use this line only if your system captures multiple races (but not a race and an
ethnicity) and the patient has chosen two or more races. This is usually done with an intake form that lists the
races and tells the patient to “check one or more” or “check all that apply.” “More than one race” must not
appear as a selection option on your intake form.
o Report patients who select multiple races in this category only, including patients who are of more than
one of the races listed on the sub lines 1a–1g (Asian) or 2a–2d (Native Hawaiian/Other Pacific Islander).
DO NOT report these patients in other categories.
o DO NOT use “More than one race” for Hispanic, Latino/a, or Spanish people who DO NOT select a race.
Report these patients on Line 7 (Unreported/Chose not to disclose), as noted above.
• Report patients who self-report their race but DO NOT indicate if they are Hispanic, Latino/a, or Spanish
origin in Column B as not of Hispanic, Latino/a, or Spanish origin on the appropriate race line.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
34 2023 UDS MANUAL | Instructions for Tables 3A and 3B
PATIENTS BEST SERVED IN A LANGUAGE OTHER THAN ENGLISH (LINE 12)
This section of Table 3B identifies the patients who may have linguistic barriers to care.
• Report on Line 12 the number of patients who are best served in a language other than English, including
those who are best served in sign language.
• Include those patients who were served in a second language by a bilingual provider and those who may have
brought their own interpreter.
• Include patients who are best served in a language other than English, even in areas where a language other
than English is the dominant language, such as Puerto Rico or the Pacific Islands.
PATIENTS BY SEXUAL ORIENTATION (LINES 13–19)
Sexual orientation is how an individual describes their emotional and sexual attraction to others.
Health centers are encouraged to establish routine data collection systems to support patient-centered, high-quality
care for patients of all sexual orientations. As with all demographic data, this information is self-reported by
patients (or by their caregivers if the patient cannot answer the questions themselves).
Collection of sexual orientation data from patients younger than 18 years of age is not mandated, but the
opportunity to report this information must be provided to all patients regardless of age.
Furthermore, patients have the choice not to disclose their sexual orientation. When sexual orientation
information is not collected or this section of the registration form is left blank, report the patient on Table 3B as
“Unknown” on Line 18a. Patients may change how they identify themselves over time. The following
descriptions may assist with data collection.
• Line 13, Lesbian or Gay: Report patients who are emotionally and sexually attracted to people of their own
gender.
• Line 14, Heterosexual (or straight): Report patients who are emotionally and sexually attracted to people of
a different gender.
• Line 15, Bisexual: Report patients who are emotionally and sexually attracted to people of their own gender
and people of other genders.
• Line 16, Other: Report patients who identify themselves as queer, asexual, pansexual, or another sexual
orientation not captured in Lines 13–15 above or Lines 17–18a below.
• Line 17, Don’t know: Report patients who self-report that they DO NOT know their sexual orientation.
• Line 18, Chose not to disclose: Report patients who chose not to disclose their sexual orientation.
• Line 18a, Unknown: Report patients for whom the health center does not know the sexual orientation (i.e.,
the health center did not implement systems to permit patients to state their sexual orientation or the patient
left this section blank).
• Line 19, Total Patients: Sum of Lines 13 through 18a.
PATIENTS BY GENDER IDENTITY (LINES 20–26)
Gender identity is the internal sense of gender. An individual may be male, female, a combination of male and
female, or another gender that may not be congruent with a patient’s sex assigned at birth.
This section helps to characterize populations served by health centers. Note that the gender identity reported on
Table 3B is the patient’s current gender identity. A patient’s sex assigned at birth is reported on Table 3A.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
35 2023 UDS MANUAL | Instructions for Tables 3A and 3B
As with all demographic data, this information is self-reported by patients (or by their caregivers if the patient
cannot answer the questions themselves). Collection of gender identity data from patients younger than 18 years
of age is not mandated, but the opportunity to provide this information must be provided to all patients regardless
of age.
Furthermore, patients have the choice not to disclose their gender identity. When gender identity information is
not collected or this section of the registration form is left blank, report the patient on Table 3B as “Unknown” on
Line 25a. Report sex assigned at birth on Table 3A. DO NOT use sex assigned at birth to identify the gender
of patients. The following descriptions may assist with data collection, but it is important to note that terminology
is evolving and patients may change how they identify themselves over time.
• Line 20, Male: Report patients who identify themselves as a man/male.
• Line 21, Female: Report patients who identify themselves as a woman/female.
• Line 22, Transgender Man/Transgender Male/Transmasculine: Report transgender patients who describe
their gender identity as man/male or a person who was assigned female sex at birth and identifies with
masculinity. (Some may just use the term “man.”)
• Line 23, Transgender Woman/Transgender Female/Transfeminine: Report transgender patients who
describe their gender identity as woman/female or a person who was assigned male sex at birth and identifies
with femininity. (Some may just use the term “woman.”)
• Line 24, Other: Report patients who DO NOT think that one of the four categories above adequately
describes them. Include patients who identify themselves as genderqueer or non-binary.
• Line 25, Chose not to disclose: Report patients who chose not to disclose their gender.
• Line 25a, Unknown: Report patients for whom the health center does not know the gender identity (i.e., the
health center did not implement systems to permit patients to state their gender identity or the patient left this
section blank).
• Line 26, Total Patients: Sum of Lines 20 through 25a.
FAQ FOR TABLES 3A AND 3B
1. Our health center collects different race and ethnicity data than required by the UDS. Why are the
data collected at this level?
The UDS classifications are consistent with those used by the Census Bureau and HHS as per the October
2011 guidance titled “
U.S. Department of Health and Human Services Implementation Guidance on Data
Collection Standards for Race, Ethnicity, Sex, Primary Language, and Disability Status” issued by OMB.
These standards govern the categories used to collect and present federal data on race and ethnicity. OMB
requires a minimum of five categories (White, Black or African American, American Indian or Alaska
Native, Asian, and Native Hawaiian or Other Pacific Islander) for race. HHS data standards, used for the
reporting of race and ethnicity for Table 3B, are based on the disaggregation of the OMB standard.
2. Do we have to report the race and Hispanic, Latino/a, or Spanish ethnicity of all our patients?
Yes. The UDS requires the classification of race and ethnicity information to assess health disparities across
sub-populations. Health centers whose data systems DO NOT support such reporting must enhance their
systems to permit the required level of reporting, rather than using the “Unreported/Chose not to disclose”
categories. If a patient self-identifies as of Hispanic, Latino/a, or Spanish origin with no distinction within the
sub-categories listed (Mexican, Mexican American, Chicano/a, Puerto Rican, Cuban, another Spanish origin),

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
36 2023 UDS MANUAL | Instructions for Tables 3A and 3B
report the patient in Column a5. Also report patients who report more than one ethnicity (e.g., Hispanic and
other Spanish origin) in Column a5.
3. How are patients of Hispanic, Latino/a, or Spanish ethnicity reported?
Race and ethnicity data appear in a matrix on Table 3B. Patients who in other systems might be reported as
Hispanic or Latino/a independent of race are reported in Column A (in one of the detail columns a1–a4) of
Table 3B of the UDS as of Hispanic, Latino/a, or Spanish origin and reported on Lines 1–7 based on their
race. If Hispanic, Latino/a, or Spanish ethnicity is the only identification recorded in the center’s patient files,
report these patients in Column A on Line 7 as having an “unreported” racial identification, and update your
data system to permit the collection of both race and ethnicity for future reporting.
4. Can we have a choice on our registration form of “more than one race”?
No. To count patients as being of “more than one race,” they must have the option of checking two or more
boxes under race and must have indeed checked more than one.
5. How are patients who receive different types of services or use more than one of our health center’s
service delivery sites reported? For example, how do we report a patient who receives both medical and
dental services or a patient who receives primary care from one service delivery site but gets prenatal
care at another?
The Patients by ZIP Code Table and Tables 3A, 3B, and 4 each provide an unduplicated patient count. Count
each individual who has at least one visit reported on Table 5 only once on the Patients by ZIP Code Table
and Tables 3A, 3B, and 4, regardless of the type or number of services they receive or where they receive
them. We define visits in detail in the Instructions for Tables that Report Visits, Patients, and Providers
section. Note the following:
• DO NOT count individuals who receive WIC services and no other services at the health center as
patients on Table 3A or 3B (or anywhere in the UDS).
• DO NOT count individuals who only receive imaging or lab services or whose only service was an
immunization or screening test as patients on Table 3A or 3B (or anywhere in the UDS).
• DO NOT count individuals who only receive health status checks and health screenings as patients on
Table 3A or 3B (or anywhere in the UDS).
6. Should the totals on Tables 3A and 3B be equal to UDS totals reported on other tables or sections?
Yes.
The sum of Table 3A, Line 39, Columns A and B (total patients by age and by sex assigned at birth) must
equal:
• Patients by ZIP Code Table total;
• Table 3B, Line 8, Column D (total patients by Hispanic, Latino/a, or Spanish ethnicity and race);
• Table 3B, Line 19 (total patients by sexual orientation);
• Table 3B, Line 26 (total patients by gender identity);
• Table 4, Line 6 (total patients by income); and
• Table 4, Line 12, Columns A and B (total patients by insurance status).
The sum of Table 3A, Lines 1–18, Columns A and B (total patients age 0–17 years) must equal:
UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
37 2023 UDS MANUAL | Instructions for Tables 3A and 3B
• Table 4, Line 12, Column A (total patients age 0–17 years).
The sum of Table 3A, Lines 19–38, Columns A and B (total patients age 18 and older) must equal:
• Table 4, Line 12, Column B (total patients age 18 and older).
7. I have multiple, separate data systems. How do I include their data on these tables?
It is the health center’s responsibility to ensure there is no duplication of data. Count patients only once,
regardless of the number of different types of services they receive. This may require the downloading and
merging of data from each system to eliminate duplicates or checking them manually. This can be a time-
consuming and potentially expensive process and should start as soon as the year ends to ensure sufficient
time for completion prior to the submission due date.
8. What do we do if we did not collect sexual orientation and/or gender identity elements?
All health centers are required to include these data elements in the registration or intake forms or during a
visit. If you did not implement the gathering of sexual orientation and/or gender identity data, report patients
on Table 3B as “Unknown” on Line 18a, sexual orientation, and Line 25a, gender identity.
DO NOT use sex at birth reported on Table 3A to complete gender identity on Table 3B.
9. Does the UDS require health care providers to ask minors for sexual orientation and gender identity
data?
The collection of sexual orientation and gender identity data is not required for minors. The information
should be included in the system and in the corresponding lines if a patient chooses to self-report their sexual
orientation and gender identity. If this information is unavailable for minors, report the patient on the
“Unknown” lines (18a and 25a).
10. Will parents or guardians be able to access their child’s response to a UDS sexual orientation and
gender identity inquiry?
There are specific provisions about protecting confidentiality of minors for patient visits related to sexual
health. Generally, there are “minor consent” laws that permit treatment to be provided to and data collected
from minors without their parent’s knowledge or approval. Contact your state Primary Care Association for
state-specific rules and regulations.
11. How are the categories for sexual orientation and gender identity defined?
The UDS classifications are based on the guidance provided in the
2015 Edition Health Information
Technology (Health IT) Certification Criteria, 2015 Edition Base Electronic Health Record (EHR) Definition,
and ONC Health IT Certification Program Modifications.
12. Do we exclude a patient who died during the year from the UDS Report?
No. If a patient was seen during the calendar year prior to their death, include the patient and their visits in all
applicable areas of the UDS Report, including their demographics, services, and clinical care details, as
applicable.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
38 2023 UDS MANUAL | Instructions for Tables 3A and 3B
TABLE 3A: PATIENTS BY AGE AND BY SEX ASSIGNED AT BIRTH
Calendar Year: January 1, 2023, through December 31, 2023
Line Age Groups
Male Patients
(a)
Female Patients
(b)
1
Under age 1
<blank for demonstration>
<blank for demonstration>
2
Age 1
<blank for demonstration>
<blank for demonstration>
3
Age 2
<blank for demonstration>
<blank for demonstration>
4
Age 3
<blank for demonstration>
<blank for demonstration>
5
Age 4
<blank for demonstration>
<blank for demonstration>
6
Age 5
<blank for demonstration>
<blank for demonstration>
7
Age 6
<blank for demonstration>
<blank for demonstration>
8
Age 7
<blank for demonstration>
<blank for demonstration>
9
Age 8
<blank for demonstration>
<blank for demonstration>
10
Age 9
<blank for demonstration>
<blank for demonstration>
11
Age 10
<blank for demonstration>
<blank for demonstration>
12
Age 11
<blank for demonstration>
<blank for demonstration>
13
Age 12
<blank for demonstration>
<blank for demonstration>
14
Age 13
<blank for demonstration>
<blank for demonstration>
15
Age 14
<blank for demonstration>
<blank for demonstration>
16
Age 15
<blank for demonstration>
<blank for demonstration>
17
Age 16
<blank for demonstration>
<blank for demonstration>
18
Age 17
<blank for demonstration>
<blank for demonstration>
19
Age 18
<blank for demonstration>
<blank for demonstration>
20
Age 19
<blank for demonstration>
<blank for demonstration>
21
Age 20
<blank for demonstration>
<blank for demonstration>
22
Age 21
<blank for demonstration>
<blank for demonstration>
23
Age 22
<blank for demonstration>
<blank for demonstration>
24
Age 23
<blank for demonstration>
<blank for demonstration>
25
Age 24
<blank for demonstration>
<blank for demonstration>
26
Ages 25–29
<blank for demonstration>
<blank for demonstration>
27
Ages 30–34
<blank for demonstration>
<blank for demonstration>
28
Ages 35–39
<blank for demonstration>
<blank for demonstration>
29
Ages 40–44
<blank for demonstration>
<blank for demonstration>
30
Ages 45–49
<blank for demonstration>
<blank for demonstration>
31
Ages 50–54
<blank for demonstration>
<blank for demonstration>
32
Ages 55–59
<blank for demonstration>
<blank for demonstration>
33
Ages 60–64
<blank for demonstration>
<blank for demonstration>
34
Ages 65–69
<blank for demonstration>
<blank for demonstration>
35
Ages 70–74
<blank for demonstration>
<blank for demonstration>
36
Ages 75–79
<blank for demonstration>
<blank for demonstration>
37
Ages 80–84
<blank for demonstration>
<blank for demonstration>
38
Age 85 and over
<blank for demonstration>
<blank for demonstration>
39
Total Patients
(Sum of Lines 1–38)
<blank for demonstration>
<blank for demonstration>
Table 3A Cross-Table Considerations:
• Table 3A, Line 39 = Table 3B, Line 8, Column D = Table 3B, Lines 19 and 26 = total patients on the Patients
by ZIP Code Table = Table 4, Lines 6 and 12.
• If you submit Grant Reports, the total number of patients reported on each grant table must be less than or
equal to the corresponding number on the Universal Report for each cell.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
39 2023 UDS MANUAL | Instructions for Tables 3A and 3B
TABLE 3B: DEMOGRAPHIC CHARACTERISTICS
Calendar Year: January 1, 2023, through December 31, 2023
blank
Patients by Race and
Hispanic. Latino/a, or
Spanish Ethnicity
blank
blank blank blank
Line Patients by Race
Yes,
Mexican,
Mexican
American,
Chicano/a
(a1)
Yes,
Puerto
Rican
(a2)
Yes,
Cuban
(a3)
Yes,
Another
Hispanic,
Latino/a, or
Spanish
Origin
(a4)
Yes,
Hispanic,
Latino/a,
Spanish
Origin,
Combined
(a5)
Total Hispanic,
Latino/a, or
Spanish Origin
(a) (Sum
Columns a1 +
a2 + a3 + a4 +
a5)
Not
Hispanic,
Latino/a,
or
Spanish
Origin
(b)
Unreported
/ Chose Not
to Disclose
Ethnicity
(c)
Total
(d)
(Sum
Columns
a+b+c)
1a
Asian Indian
<blank for
demonstration>
<blank for
demonstration>
<cell not reported>
<blank for
demonstration>
1b
Chinese
1c
Filipino
1d
Japanese
1e
Korean
1f
Vietnamese
1g
Other Asian
1
Total Asian (Sum Lines
1a+1b+1c+1d+1e+1f+1g)
2a
Native Hawaiian
<blank for
demonstration>
<blank for
demonstration>
<cell not reported>
<blank for
demonstration>
2b
Other Pacific Islander
<blank for
demonstration>
<blank for
demonstration>
<cell not reported>
<blank for
demonstration>
2c
Guamanian or Chamorro
2d
Samoan
2
Total Native
Hawaiian/Other Pacific
Islander
(Sum Lines 2a+2b+2c+2d)
<blank for
demonstration>
<blank for
demonstration>
<cell not reported>
<blank for
demonstration>
3
Black/African American
<blank for
demonstration>
<blank for
demonstration>
<cell not reported>
<blank for
demonstration>
4
American Indian/Alaska
Native
<blank for
demonstration>
<blank for
demonstration>
<cell not reported>
<blank for
demonstration>
5
White
<blank for
demonstration>
<blank for
demonstration>
<cell not reported>
<blank for
demonstration>
6
More than one race
<blank for
demonstration>
<blank for
demonstration>
<cell not reported>
<blank for
demonstration>
7
Unreported/Chose not to
disclose race
<blank for
demonstration>
<blank for
demonstration>
<blank for
demonstration>
<blank for
demonstration>
8
Total Patients
(Sum of Lines 1 + 2 + 3 to
7)
<blank for
demonstration>
<blank for
demonstration>
<blank for
demonstration>
<blank for
demonstration>

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
40 2023 UDS MANUAL | Instructions for Tables 3A and 3B
Line Patients Best Served in a Language Other than English
Number
(a)
12
Patients Best Served in a Language Other than English
<blank for demonstration>
Line Patients by Sexual Orientation
Number
(a)
d
ivider
Line Patients by Gender Identity
Number
(a)
13 Lesbian or Gay
<blank >
divider
20 Male
<blank>
14 Heterosexual (or straight)
<blank >
divider
21 Female
<blank >
15 Bisexual
<blank >
divider
22
Transgender Man/Transgender
Male/Transmasculine
<blank >
16 Other
<blank >
divider
23
Transgender Woman/Transgender
Female/Transfeminine
<blank >
17 Don’t know
<blank >
divider
24 Other
<blank >
18 Chose not to disclose
<blank >
divider
25 Chose not to disclose
<blank >
18a Unknown
<blank >
25a Unknown
<blank >
19
Total Patients
(Sum of Lines 13 to 18a)
<blank >
divider
26
Total Patients
(Sum of Lines 20 to 25a)
<blank>
Table 3B Cross-Table Considerations:
• Table 3B, Lines 8, 19, and 26 = Table 3A, Line 39 = Patients by ZIP Code Table = Table 4, Lines 6 and 12.
• Tables 3B and 7 both report patients by race and Hispanic, Latino/a, or Spanish ethnicity. The data sources for
identifying race and ethnicity for the two tables should be the same, and the number of patients reported on
Table 7 by race and ethnicity cannot exceed the number of patients in the same category on Table 3B.
• If you submit Grant Reports, the total number of patients reported on each grant table must be less than or
equal to the corresponding number on the Universal Report for each cell.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
41 2023 UDS MANUAL | Instructions for Table 4
Instructions for Table 4: Selected Patient Characteristics
Table 4 collects descriptive data on selected characteristics of health center patients.
In addition to submitting this table as described below within the EHBs, health centers may voluntarily submit de-
identified patient-level report data using Health Level Seven (HL7®) Fast Healthcare Interoperability Resources
(FHIR®) R4 standards for this table.
INCOME AS A PERCENTAGE OF POVERTY GUIDELINE, LINES 1–6
The report should include the most current income data for all patients (not only from patients eligible for a
sliding fee discount), which must have been collected at or within 12 months of the last calendar year visit.
Determine a patient’s income relative to the 2023 federal poverty guidelines (FPG)
.
• Report patients by income, as defined by the health center’s board policy consistent with the Health Center
Program Compliance Manual. Children, with the exception of emancipated minors or those presenting for
minor consent services, should be classified under their parents’ or guardians’ income.
• Report patients whose information was not collected at or within 12 months of their last visit in the calendar
year on Line 5 as “Unknown.”
• Self-declaration of income from patients is acceptable as long as that is consistent with the health center’s
board-approved policies and procedures for collecting these data. This is particularly important for those
patients whose wages are paid in cash and who have no other means of proving their income. If income
information consistent with the health center’s board policy is lacking, report the patient as having
“Unknown” income.
• DO NOT allocate patients with “Unknown” income to the other income groups.
• DO NOT classify a patient who is experiencing homelessness, is a migratory agricultural worker, or is on
Medicaid as having income below the FPG based on these factors alone.
PRIMARY THIRD-PARTY MEDICAL INSURANCE, LINES 7–12
This portion of the table provides data on patients classified by their age and primary source of insurance for
medical care. DO NOT report other forms of insurance, such as dental, mental health, or vision coverage. Note
that there is NO “Unknown” insurance classification on this table. Also note that states often rename federal
insurance programs, such as CHIP and Medicaid. Health centers are to collect medical insurance information each
calendar year from all patients to maximize third-party payments.
• Patient primary medical insurance is classified into seven types, as shown on the following pages.
• In rare instances, a patient may have insurance that the health center cannot or does not bill. Even in these
instances, report the patient as being insured and report the type of insurance.
• Report the primary medical insurance patients had at the time of their last visit regardless of whether that
insurance was billed or paid for any or all of the visit services.
• Patients are divided into two age groups: 0–17 (Column A) and 18 and older (Column B) based on their age
on December 31, 2023 (consistent with ages reported on Table 3A).
• DO NOT report public programs that reimburse for selected services, such as the Early and Periodic
Screening, Diagnosis, and Treatment (EPSDT) program; Breast and Cervical Cancer Early Detection Program
(BCCEDP); or Title X, as a patient’s primary medical insurance.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
42 2023 UDS MANUAL | Instructions for Table 4
Note: However, report the revenue from public programs that reimburse for selected services as Other Public
payers on Table 9D.
None/Uninsured (Line 7)
Report patients who did NOT have medical insurance at the time of their last visit on Line 7. This may include
patients who were insured earlier in the year, as well as patients whose visit was paid for by a third-party source
that was not insurance, such as EPSDT, BCCEDP, Title X, or some state or local safety net or indigent care
programs.
• Report a minor receiving services with parental consent under the family’s insurance.
• Report children seen in a school-based service site under their parent’s health insurance. This information
must be obtained if they are to be included in the UDS Report. Report emancipated minors or patients seeking
minor consent services permitted in the state, such as family planning or mental health services, as Uninsured
if they DO NOT have access to the parent’s information.
• Presume a patient with Medicaid, Private, or Other Public dental insurance to have the same kind of medical
insurance. If a dental patient does not have dental insurance, you may NOT assume that they are uninsured
for medical care. Instead, obtain this information from the patient.
• Patients served in correctional facilities may be classified as Uninsured unless they have documentation of
insurance, such as Medicaid or Medicare, in which case report them on that insurance line.
• Obtain the coverage information of patients in facilities (other than correctional), such as residential drug
programs, college dorms, and military barracks. DO NOT assume them to be uninsured.
• DO NOT report patients as Uninsured if they have medical insurance that did not pay for their visit.
Medicaid (Line 8a)
Report patients covered by state-run programs operating under the guidelines of Titles XIX and XXI (as
appropriate) of the Social Security Act.
• Include Medicaid programs known by state-specific names (e.g., California’s “Medi-Cal” program).
• Include patients covered by “state-only” programs covering individuals who are ineligible for federal
matching funds (e.g., undocumented children, pregnant patients) and paid through Medicaid, if they cannot
otherwise be identified as having another insurance.
• Report patients enrolled in both Medicaid and Medicare on Lines 9 (Medicare) and 9a (Dually Eligible), but
not on Line 8a.
• Report patients who are enrolled in Medicaid but receive services through a private managed care plan that
contracts with the state Medicaid agency on Line 8a, not as privately insured (Line 11). This also applies in
states that have a Medicaid waiver permitting Medicaid funds to be used to purchase private insurance for
services.
CHIP Medicaid (Line 8b)
Report patients covered by the Children’s Health Insurance Program (CHIP) Reauthorization Act and provided
through the state’s Medicaid program.
• In states that use Medicaid to handle the CHIP program, it is sometimes difficult or impossible to distinguish
between “Medicaid” and “CHIP Medicaid.” In other states, the distinction is readily apparent (e.g., they have
different cards). Even where it is not obvious, CHIP patients may still be identifiable from a “plan” code or

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
43 2023 UDS MANUAL | Instructions for Table 4
some other embedded code in the membership number. This may also vary from county to county within a
state. Obtain information on coding practice from the state and/or county.
• If there is no way to distinguish between Medicaid and CHIP administered through Medicaid, classify all
covered patients as Medicaid (Line 8a).
Medicare (Line 9)
Report patients covered by the federal insurance program for the aged, blind, and disabled (Title XVIII of the
Social Security Act).
• Report patients who have Medicare and Medicaid (“dually eligible”) on Line 9. In addition, report as Dually
Eligible on Line 9a.
• Report patients who have Medicare and a private (“Medigap”) insurance on Line 9. DO NOT include them as
Dually Eligible on Line 9a.
• Report patients enrolled in “Medicare Advantage” products on Line 9, even though their services were
covered by a private insurance company.
• Report Medicare-enrolled patients who are still working and are insured by both an employer-based plan and
Medicare as Private Insurance on Line 11, because the employer-based insurance plan is billed first. DO NOT
include them as Dually Eligible on Line 9a.
Dually Eligible (Medicare and Medicaid) (Line 9a)
Report patients with both Medicare and Medicaid insurance.
• Report patients who are dually eligible on Line 9a and include them on Line 9. This line is a subset of Line 9
(Medicare).
• Report patients who are enrolled in Medicare Advantage Special Needs Plan as Dually Eligible on Line 9a.
• DO NOT include Medicare gap “Medigap” (supplemental insurance plan) enrollees on Line 9a. Report
patients who buy Medicare gap insurance as Medicare patients, on Line 9.
Other Public Insurance (Non-CHIP) (Line 10a)
Report state and/or local government programs, such as Massachusetts’ CommonHealth plans, that provide a
broad set of benefits for eligible individuals. Include any public-paid or subsidized private insurance not reported
elsewhere on Table 4.
• Report Medicaid expansion programs (such as state premium assistance programs) using Medicaid funds to
help patients purchase their insurance through exchanges as Medicaid (Line 8a) if it is possible to identify
them. Otherwise, report them as Private Insurance (Line 11).
• DO NOT report any CHIP, Medicaid, or Medicare patients on Line 10a.
• DO NOT report uninsured individuals whose visit may be covered by a public source with limited benefits,
such as Title X, EPSDT, BCCEDP, AIDS Drug Assistance Program providing pharmaceutical coverage for
patients with human immunodeficiency virus (HIV), etc.
Not
e: Public programs that reimburse for selected services are, however, considered Other Public payers on
Table 9D.
• DO NOT include patients covered by workers’ compensation (which is liability insurance for the employer—
not health insurance for the patient).

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
44 2023 UDS MANUAL | Instructions for Table 4
• DO NOT include patients who have insurance through federal or state insurance exchanges, regardless of the
extent to which their premium cost is subsidized (in whole or in part). Report them as Private Insurance (Line
11).
Other Public Insurance CHIP (Line 10b)
In states where CHIP is contracted through a private third-party payer, report patients on the Other Public
Insurance CHIP line.
• Report CHIP programs that are run through the private sector, often administered through health maintenance
organizations (HMOs). Coverage may appear to be a private insurance plan (such as Blue Cross/Blue Shield)
but is funded through CHIP and is to be counted on Line 10b.
• Report CHIP patients who are on plans administered by Medicaid coordinated care organizations (CCOs).
• DO NOT report CHIP as Private Insurance.
Private Insurance (Line 11)
Report patients with health insurance provided by private (commercial) and not-for-profit companies.
• Individuals may obtain insurance through employers or on their own.
• Include patients who purchase insurance through the federal or state exchanges.
• In states using Medicaid expansion to support the purchase of insurance through exchanges, report patients
covered under these plans on Line 8a (Medicaid). Report patients who are not identifiable as Medicaid
patients on Line 11 (Private Insurance).
• Private insurance includes insurance purchased for public employees or retirees, such as Tricare, Trigon, or
the Federal Employees Benefits Program.
MANAGED CARE UTILIZATION, LINES 13A–13C
This part of Table 4 provides data on managed care enrollment during the calendar year and specifically reports
on patient member months in health center contracted comprehensive medical managed care plans.
• If patients are enrolled in a managed care program that permits them to receive care from any number of
providers, including providers other than the health center and its providers, this is NOT to be reported as
managed care in the UDS, and NO member months are reported.
• DO NOT report in this section enrollees in primary care case management (PCCM) programs, the Centers for
Medicare & Medicaid Services (CMS) patient-centered medical home (PCMH) demonstration grants, or other
third-party plans that pay a monthly fee (often as low as $5 to $10 per member per month) to manage patient
care.
• DO NOT include managed care enrollees whose capitation or enrollment is limited to behavioral health or
dental services only. (However, an enrollee who has medical and dental is counted.)
Member Months
A member month is defined as one individual enrolled in a managed care plan for one month. For example, an
individual who is a member of a plan for a full year generates 12 member months; a family of five enrolled for 6
months generates 30 member months (5 individuals × 6 months = 30 member months).

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
45 2023 UDS MANUAL | Instructions for Table 4
Member month information is most often obtained from monthly enrollment lists generally supplied by managed
care companies to their providers. Health centers should always save these documents. In the event they have not
been saved, health centers should request duplicates early to permit timely filing of the UDS Report.
Note: It is possible for an individual to be enrolled in a managed care plan, assigned to a health center, and yet not
seen during the calendar year. The member months for such individuals are still to be reported in this section.
This is the only place on the UDS tables where an individual may be reported who is not being counted as a
patient.
Capitated Member Months (Line 13a)
Report the total capitated member months by source of payment. This is derived by adding the total enrollment
reported from each capitated plan for each month.
• A patient is in a capitated plan if the contract between the health center and the HMO, accountable care
organization (ACO), or other similar plan stipulates that, for a flat payment per month, the health center will
provide the patient all the services on a negotiated list. (Oregon programs should include enrollees in CCOs
on this line.)
• This usually includes, at a minimum, all medical office visits.
• Payments are received (and reported on Table 9D) regardless of whether any service is rendered to the patient
in that month. The capitated member months reported on Line 13a relate to the net capitated revenue reported
on Table 9D, Lines 2a, 5a, 8a, and/or 11a.
Fee-for-Service Member Months (Line 13b)
Report the total fee-for-service member months by source of payment.
• A fee-for-service member month is defined as one patient being assigned to a health center or health center
service delivery provider for one month, during which time the patient may receive contractually defined
basic primary care services only from the health center but for whom the services are paid on a fee-for-service
basis.
• There is a relationship between the fee-for-service member months reported on Line 13b and the revenue
reported on Table 9D on Lines 2b, 5b, 8b, and/or 11b.
• It is common for patients to have their primary care covered by capitation but other services (e.g., behavioral
health or pharmacy) paid separately on a fee-for-service basis as a “carve-out
” in addition to the capitation.
• DO NOT include member months for individuals who receive “carved-out” services under a fee-for-service
arrangement on Line 13b if those individuals have already been counted for the same month as a capitated
member on Line 13a.
SPECIAL POPULATIONS, LINES 14–26
This section asks for a count of patients from special populations, including migratory and seasonal agricultural
workers and their family members, patients who are experiencing homelessness, patients who are served by
school-based service sites, patients who are veterans, and patients who are served at a health center located in or
immediately accessible to a public housing site. Awardees who receive funding from section 330(g) (MHC) and
section 330(h) (HCH) must provide additional information on their agricultural employment and/or housing
characteristics.
• All health centers report these populations, regardless of whether they directly receive special population
funding.
UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
46 2023 UDS MANUAL | Instructions for Table 4
• Migratory or seasonal agricultural workers’ status must be verified at least every 2 years by MHC awardees.
• Housing status must be collected by HCH awardees at the first visit of the year when the patient was
identified to be experiencing homelessness. Further details are provided in the
Total Patients Experiencing
Homelessness, Lines 17–23 section.
• The special populations detailed below are not mutually exclusive. Patients can be reported in more than one
category, as appropriate (e.g., a patient can be reported as both a veteran and experiencing homelessness).
Total Migratory and Seasonal Agricultural Workers and Their Family Members, Lines
14–16
Total Agricultural Workers or Their Family Members, Line 16: Report the number of patients seen during
the calendar year who were either migratory or seasonal agricultural workers, family members of migratory or
seasonal agricultural workers, or aged or disabled former migratory agricultural workers (as described in the
statute section 330(g)(1)(B)). All health centers must report on this line, though for some the number may be zero.
Only health centers that receive section 330(g) (MHC) funding provide separate totals for migratory and seasonal
agricultural workers on Lines 14 and 15. For section 330(g) awardees, the sum of Lines 14 + 15 = Line 16.
• For either migratory or seasonal agricultural workers, report patients who meet the definition of agriculture as
farming in all its branches, as defined by the Office of Management and Budget (OMB)-developed
North
American Industry Classification System (NAICS), and include seasonal workers included in codes 111 and
112 and all sub-codes therein, including sub-codes 1151 and 1152.
Instructions for reporting migratory and seasonal agricultural workers:
• Migratory Agricultural Workers, Line 14: Report patients whose principal employment is in agriculture
and who establish a temporary home for the purposes of such employment as a migratory agricultural worker,
as defined by section 330(g) of the PHS Act. Migratory agricultural workers are usually hired laborers who
are paid piecework, hourly, or daily wages. Include patients who had such work as their principal employment
within 24 months of their last visit during the calendar year, as well as their family members who have also
used the center. The family members may or may not move with the worker or establish a temporary home.
Note: Agricultural workers who leave a community to work elsewhere are classified as migratory workers
when served in their home community, as are those who migrate to a community to work there.
o Include aged and disabled former migratory agricultural workers, as defined in section 330(g)(1)(B), and
their family members. Aged and disabled former agricultural workers include those who were previously
migratory agricultural workers but who no longer work in agriculture because of age or disability.
• Seasonal Agricultural Workers, Line 15: Report patients whose principal employment is in agriculture on a
seasonal basis (e.g., picking fruit during the limited months of a picking season), but who DO NOT establish
a temporary home for purposes of such employment. Seasonal agricultural workers are usually hired laborers
who are paid piecework, hourly, or daily wages. Include patients who have been so employed within 24
months of their last visit during the calendar year, as well as their family members who are patients of the
health center.
Note: Seasonal agricultural workers may be employed throughout the year for multiple crop seasons and as a
result might work full-time.
Total Patients Experiencing Homelessness, Lines 17–23
Total Homeless, Line 23: Report the total number of patients known to have experienced homelessness at the
time of any service provided during the calendar year, even if their housing situation changed during the year.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
47 2023 UDS MANUAL | Instructions for Table 4
Include patients on this line who experienced homelessness at any time during the year and were seen by the
health center for services. All health centers must report on this line, though for some the number may be zero.
Only health centers receiving section 330(h) (HCH) funding provide separate totals for patients by housing
location on Lines 17 through 22. For section 330(h) awardees, the sum of Lines 17 through 22 = Line 23.
• Report patients who lack housing. Include patients whose primary residence during the night is a supervised
public or private facility that provides temporary living accommodations. Include patients who reside in
transitional housing or permanent supportive housing.
• Children and youth at risk of homelessness, homeless veterans, and veterans at risk of homelessness may be
included.
7
HCH awardees will provide detail on patients experiencing homelessness by the type of shelter arrangement the
patients had when they were first encountered for a visit during the calendar year while experiencing
homelessness.
Experiencing homelessness includes patients who at any point during the calendar year experienced homelessness
or were at risk of homelessness for up to 12 months after they were last documented to experience homelessness.
Housing status is based on the housing arrangement at the first visit during the calendar year when the patient is
identified as experiencing homelessness.
The following applies when categorizing patients for Lines 17 through 22:
• Report the patient’s shelter arrangement as of the first visit during the calendar year when the patient was
identified as experiencing homelessness. The shelter arrangement is reported as where the patient was
housed the prior night.
• Report patients who spent the prior night incarcerated, in an institutional treatment program (e.g., mental
health, substance use disorder), or in a hospital based on where they intend to spend the night after their
visit/release. If they DO NOT know, report their shelter arrangement as Street, on Line 20.
• Shelter, Line 17: Report patients who are living in an organized shelter for individuals experiencing
homelessness. Shelters that generally provide meals and a place to sleep are regarded as temporary and often
limit the number of days or the hours of the day that a resident may stay at the shelter.
• Transitional Housing, Line 18: Transitional housing units are generally small units (six people is common)
where people transition from a shelter and are provided extended, but temporary, housing stays (generally
between 6 months and 2 years) in a service-rich environment. Transitional housing provides a greater level of
independence than traditional shelters and may require the resident to pay some or all of the rent, participate
in the maintenance of the facility, and/or cook their own meals. Report only those patients who are
transitioning from a homeless environment. DO NOT include those who are transitioning from jail or those
residing in or transitioning from an institutional treatment program, the military, schools, or other institutions.
• Doubled Up, Line 19: Report patients who are living with others. The arrangement is considered to be
temporary and unstable, though a patient may live in a succession of such arrangements over a protracted
period. DO NOT include the individual who invites a patient experiencing homelessness to stay in their home
for the night. DO NOT include a co-tenant rental as doubled up.
• Street, Line 20: Report in this category patients who are living outdoors, in a vehicle, in an encampment, in
makeshift housing/shelter, or in other places generally not deemed safe or fit for human occupancy.
7
Health centers may use criteria as defined by the U.S. Department of Housing and Urban Development (HUD) to assist in defining “children and youth at
risk of homelessness, homeless veterans, and veterans at risk of homelessness.”

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
48 2023 UDS MANUAL | Instructions for Table 4
• Permanent Supportive Housing,
8
Line 21a: Permanent supportive housing usually is in service-rich
environments, does not have time limits, and may be restricted to people with some type of disabling
condition.
• Other, Line 21: Report patients who were housed when first seen during the year and were no longer
homeless, but who were still eligible for the program because they experienced homelessness during the
previous 12 months. Under section 330(h), a health center may continue to provide services for up to 12
months after last documentation as experiencing homelessness to patients whom the health center has
previously served but are no longer experiencing homelessness as a result of becoming a resident in
permanent housing. Include them in this category. Also include patients who reside in single-room-occupancy
(SRO) hotels or motels and patients who reside in other day-to-day paid housing or other housing programs
that are intended for people experiencing homelessness.
• Unknown, Line 22: Report patients known to be experiencing homelessness whose housing arrangements are
unknown.
• DO NOT report patients currently residing in a jail or an institutional treatment program as homeless until
they are released to the street with no housing arrangement.
• DO NOT report patients who are part of the foster system program and are placed with a family, group home,
or in some other arrangement as homeless.
Total School-Based Service Site Patients, Line 24
All health centers that identified a school-based service site in their scope of project (as documented on Form 5B)
are to report the total number of patients who received health care services at the approved school service delivery
site(s). Include patients who received countable visits within any of the service categories (medical, mental health,
etc.) when conducted at an approved school-based service site. All patient characteristic details are to be collected
and reported.
• Report patients served at in-scope school-based service sites located on school grounds, limited to preschool,
kindergarten, and primary through secondary schools (exclude colleges and universities), that provide on-site
health services.
• Services are targeted to the students at the school but may also be provided to siblings or parents and may
occasionally include patients residing in the immediate vicinity of the school.
• DO NOT include, as patients, students who only receive screening services or mass treatment, such as
vaccinations or fluoride treatments, at a school.
Total Veterans, Line 25
All health centers are to report the total number of patients who served in the active military, naval, or air service,
which includes full-time service in the Air Force, Army, Coast Guard, Marines, Navy, Space Force, or as a
commissioned officer of the Public Health Service or National Oceanic and Atmospheric Administration. In
addition, include patients who served in the National Guard or Reserves on active duty status.
Include this question in the patient information/intake form at each service delivery site.
• Report only those who affirmatively indicate they previously served in these branches of the military or
armed forces.
8
Health centers may use criteria as defined by HUD to assist in defining permanent supportive housing.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
49 2023 UDS MANUAL | Instructions for Table 4
• DO NOT report patients who do not respond, regardless of other indicators.
• DO NOT report veterans of other nations’ militaries, even if they served in wars in which the United States
was also involved.
• DO NOT report military members who served on active duty (full-time status in their military capacity) at the
time of their last visit during the year.
Total Patients Served at a Health Center Service Delivery Site Located in or
Immediately Accessible to a Public Housing Site, Line 26
All health centers are to report all patients seen at a service delivery site located in or immediately accessible
to public housing, regardless of whether the patients are residents of public housing or the health center receives
funding under section 330(i) (PHPC).
• Report patients on this line if they are served at health center service delivery sites that meet the statutory
definition for the PHPC program (located in or immediately accessible to public housing).
• Report all patients seen at the health center service delivery site if it is located in or immediately accessible to
agency-developed, -owned, or -assisted low-income housing, including mixed-finance projects.
• This is the only field in the UDS Report that requires you to provide a count of all patients based on the
health center service delivery site’s proximity to public housing.
• DO NOT consider Section 8 housing units that receive no public housing agency support other than Section 8
housing vouchers as public housing.
Note: No
t all patients served at service delivery sites located in or immediately accessible to public housing
are themselves residents of public housing, but they are to be included in the count.
FAQ FOR TABLE 4
1. Do we determine a patient’s income relative to the FPG based on the location of the health center or
based on the residence of the patient?
Use the FPG based on the location of the health center. All states (except Alaska and Hawaii) and the U.S.
territories use the same standard poverty guidelines. For patients being served in Alaska or Hawaii, use the
FPG established for those locations.
2. Patients who are experiencing homelessness or who are agricultural workers generally DO NOT have
income verification. Can we report them as having income at 100% and below poverty?
No. You can report them as having “Unknown” income, but not as having income below poverty unless you
verify this at least annually. However, subject to your health center’s financial policies and procedures, you
may document their income in your system based on their verbal attestation of their income.
3. If a patient is seen only for dental care, do we report the patient’s dental insurance on Lines 7–12?
No. Table 4 reports only patients’ medical coverage. All health centers must collect medical coverage
information from all patients, even if they have not been provided medical services.
Note: If a patient’s medical insurance is not known, but they have Medicaid, Private, or Other Public dental
insurance at the time of their last visit, you may assume they have the same kind of medical insurance. If they
DO NOT have dental insurance at the time of their last visit, you may NOT assume they are uninsured for
medical care. You must determine whether they have medical insurance.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
50 2023 UDS MANUAL | Instructions for Table 4
4. Our state is using Medicaid expansion provisions to assist patients with buying private insurance.
Should we count them as Medicaid or Private?
If patients are Medicaid expansion patients, report them as Medicaid, Line 8a (this may require looking for
specific plan numbers or other identifying characteristics in patients’ insurance enrollment). If you are unable
to identify Medicaid expansion patients, report them as Private, Line 11.
5. We serve students at a school-based service site. They often DO NOT know what insurance they have,
if any, and they have no information on their family’s/household’s income. Can we report them as
having income at 100% and below poverty and Uninsured?
No. Y
ou may not report them as having income below poverty and Uninsured. Obtain insurance information
from the parents or guardians of students served at school-based service sites, unless they are exclusively
receiving minor consent services. Minor consent services are defined by state law and are generally limited to
a very specific range of services, such as those related to contraception, sexually transmitted diseases, and
mental health. Not all states provide for them. For all other services, children will require parental consent,
and the consent form should include income and insurance information.
Note: Subject to the health center’s policies and procedures, it is acceptable to ask for this information and to
assure parents that you will not bill the insurance without their knowledge. If you DO NOT obtain parental
consent, report the child as having “Unknown” income. The patient’s health insurance is required, even if it is
not billed.
6. Do we classify patients in the insurance section as Uninsured if their medical insurance did not pay for
the visit?
No. Always report patients based on their primary medical care insurance, even if the insurance did not pay or
you are unable to bill for the service. Some examples follow:
• Report a patient with Medicare who was seen for a dental visit that was not paid for by Medicare as
having Medicare for this table.
• Report a patient with private insurance who had not reached their deductible as a Private Insurance
patient.
7. Should the number of patients by income and by insurance source equal the total number of
unduplicated patients reported on Tables 3A and 3B and the Patients by ZIP Code Table?
Yes.
8. Is it possible to have more members in one month (average) than total patients in an insurance
category?
It is possible for the number of member months for any one payer (e.g., Medicaid) to exceed 12 times the
number of patients reported on the corresponding insurance line, especially when patients are enrolled in the
managed care plan but they did not come to the health center during the calendar year. As a rule, there is a
relationship between the member months reported on Lines 13a and 13b and the insured patients reported on
Lines 7 through 11.
9. If we do not receive direct funding under the HCH, MHC, or PHPC programs, do we need to report
the total number of special population patients served?

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
51 2023 UDS MANUAL | Instructions for Table 4
Yes. Even health centers that DO NOT receive grant funding for special populations are required to complete
the following:
• Line 16 (the total number of patients seen during the calendar year who were agricultural workers or their
family members),
• Line 23 (total number of patients known to have experienced homelessness at any time of the year and
received services during the calendar year),
• Line 24 (patients of a school-based service site),
• Line 25 (veterans), and
• Line 26 (total number of patients served at a health center located in or immediately accessible to a public
housing site).
The details on Lines 17–22 are grayed out if you did not receive HCH funding—only enter the total on Line
23.
The details on Lines 14 and 15 are grayed out if you did not receive MHC funding—only enter the total on
Line 16.
10. What timing determines a patient’s homeless status and shelter arrangement?
For all health centers (regardless of HCH funding status), include the total number of patients who
experienced homelessness at any point during the year and received services during the year on Line 23.
For awardees that receive HCH funding, continue to count patients seen who are no longer experiencing
homelessness due to becoming residents of permanent housing for 12 months after their last visit as homeless.
For awardees that receive HCH funding, report all patients experiencing homelessness by their shelter
arrangement on Lines 17–22.
Asking health centers to report patients experiencing homelessness by their sheltering arrangements as of
their first visit during the calendar year is intended to help health centers determine to which shelter
arrangement they should report a patient if shelter status changes during the year.
11. Who should be reported as Patients Served at a Health Center Located in or Immediately Accessible to
a Public Housing Site on Line 26?
Report the total number of patients who were served at any health center service delivery site that you
consider (based on the health center’s determination if any service delivery locations meet the statutory
definition for PHPC) to be located in or immediately accessible to public housing, regardless of whether or
not the health center receives funding under section 330(i) (PHPC), and regardless of whether or not patients
resided in public housing. This is a site-based count, and the patient’s address or residence in public housing
is not to be considered.
12. Are patients who were dishonorably discharged or released considered a veteran?
No. Only patients who were discharged or released under conditions other than dishonorable are considered a
veteran.
13. Do the totals need to equal other sections or tables?
The following totals must be equal across tables and sections:
• Patients by ZIP Code Table, Column B must equal Table 4, Line 7, Columns A and B.
• Patients by ZIP Code Table, Column C must equal Table 4, Lines 8 and 10, Columns A and B.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
52 2023 UDS MANUAL | Instructions for Table 4
• Patients by ZIP Code Table, Column D must equal Table 4, Line 9, Columns A and B.
• Patients by ZIP Code Table, Column E must equal Table 4, Line 11, Columns A and B.
• The sum of Table 3A, Line 39, Columns A and B (total patients by age and gender) must equal Table 3B,
Line 8, Column D (total patients by race and Hispanic, Latino/a, or Spanish ethnicity); Table 3B, Line 19
(total patients by sexual orientation); Table 3B, Line 26 (total patients by gender identity); Table 4, Line 6
(total patients by income); and Table 4, Line 12, Columns A and B (total patients by medical insurance
status).
• The sum of Table 3A, Lines 1–18, Columns A and B (total patients age 0–17 years) must equal Table 4,
Line 12, Column A (total patients age 0–17 years).
• The sum of Table 3A, Lines 19–38, Columns A and B (total patients age 18 and older) must equal Table
4, Line 12, Column B (total patients age 18 and older).
• The sum of Table 3A, Line 39, Columns A and B (total patients by age and gender) must equal Table 4,
Line 12, Columns A and B (total patients by insurance status).
The same is true for each of the Grant Reports submitted.
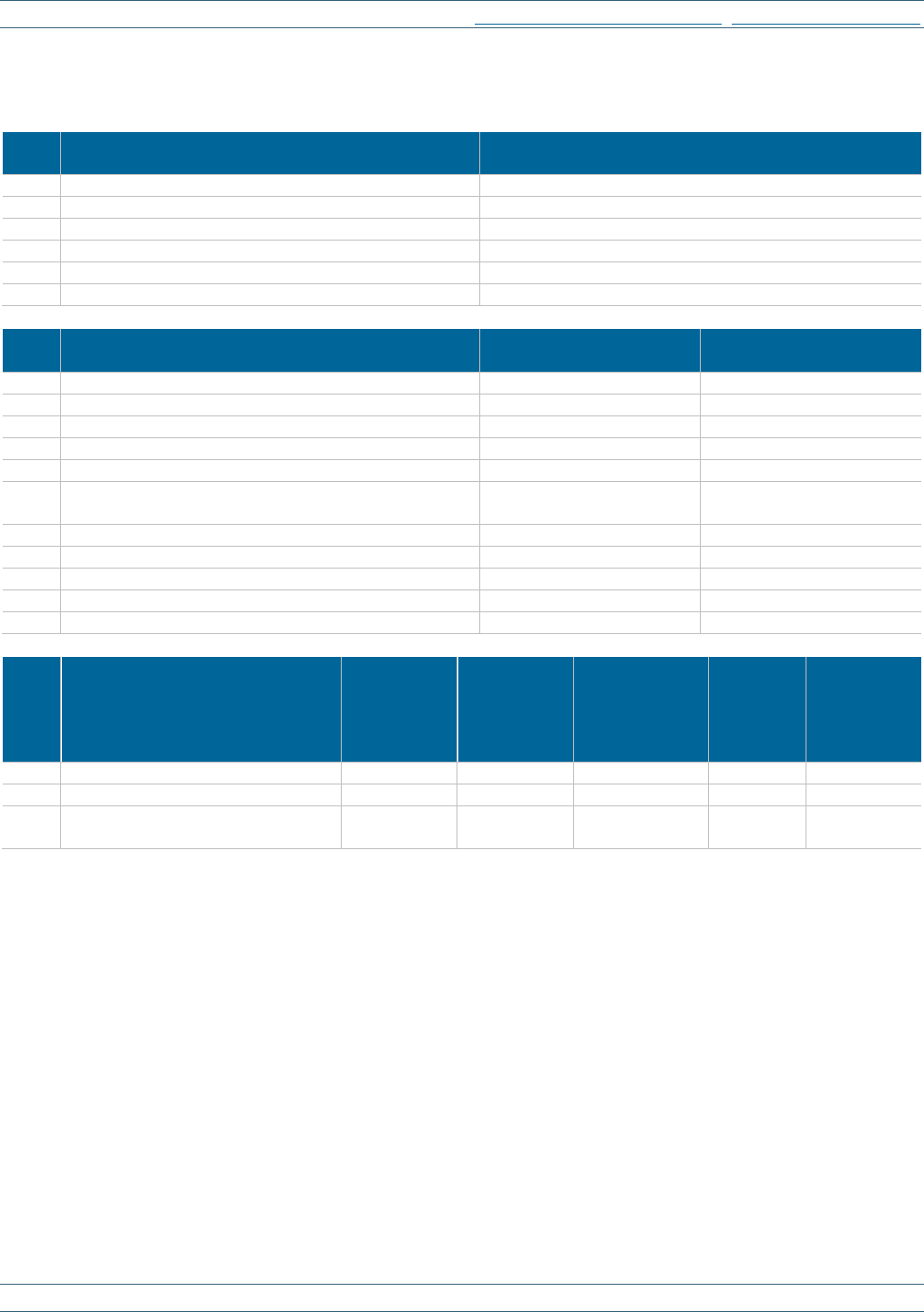
UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
53 2023 UDS MANUAL | Instructions for Table 4
TABLE 4: SELECTED PATIENT CHARACTERISTICS
Calendar Year: January 1, 2023, through December 31, 2023
Line Income as Percentage of Poverty Guideline
Number of Patients
(a)
1
100% and below
<blank for demonstration>
2
101–150%
<blank for demonstration>
3
151–200%
<blank for demonstration>
4
Over 200%
<blank for demonstration>
5
Unknown
<blank for demonstration>
6
TOTAL (Sum of Lines 1–5)
<blank for demonstration>
Line Primary Third-Party Medical Insurance
0–17 years old
(a)
18 and older
(b)
7
None/Uninsured
<blank for demonstration>
<blank for demonstration>
8a
Medicaid (Title XIX)
<blank for demonstration>
<blank for demonstration>
8b
CHIP Medicaid
<blank for demonstration>
<blank for demonstration>
8
Total Medicaid (Line 8a + 8b)
<blank for demonstration>
<blank for demonstration>
9a
Dually Eligible (Medicare and Medicaid)
<blank for demonstration>
<blank for demonstration>
9
Medicare (Inclusive of dually eligible and other Title
XVIII beneficiaries)
<blank for demonstration>
<blank for demonstration>
10a
Other Public Insurance (Non-CHIP) (specify___)
<blank for demonstration>
<blank for demonstration>
10b
Other Public Insurance CHIP
<blank for demonstration>
<blank for demonstration>
10
Total Public Insurance (Line 10a + 10b)
<blank for demonstration>
<blank for demonstration>
11
Private Insurance
<blank for demonstration>
<blank for demonstration>
12
TOTAL (Sum of Lines 7 + 8 + 9 +10 +11)
<blank for demonstration>
<blank for demonstration>
Line Managed Care Utilization
Medicaid
(a)
Medicare
(b)
Other Public
Including
Non-Medicaid
CHIP
(c)
Private
(d)
TOTAL
(e)
13a
Capitated Member Months
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
13b
Fee-for-service Member Months
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
13c
Total Member Months
(Sum of Lines 13a + 13b)
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
54 2023 UDS MANUAL | Instructions for Table 4
TABLE 4: SELECTED PATIENT CHARACTERISTICS (CONTINUED)
Calendar Year: January 1, 2023, through December 31, 2023
Line Special Populations
Number of Patients
(a)
14
Migratory (330g awardees only)
<blank for demonstration>
15
Seasonal (330g awardees only)
<blank for demonstration>
16
Total Agricultural Workers or Their Family Members
(All health centers report this line)
<blank for demonstration>
17
Homeless Shelter (330h awardees only)
<blank for demonstration>
18
Transitional (330h awardees only)
<blank for demonstration>
19
Doubling Up (330h awardees only)
<blank for demonstration>
20
Street (330h awardees only)
<blank for demonstration>
21a
Permanent Supportive Housing (330h awardees only)
21
Other (330h awardees only)
<blank for demonstration>
22
Unknown (330h awardees only)
<blank for demonstration>
23
Total Homeless (All health centers report this line)
<blank for demonstration>
24
Total School-Based Service Site Patients
(All health centers report this line)
<blank for demonstration>
25
Total Veterans (All health centers report this line)
<blank for demonstration>
26
Total Patients Served at a Health Center Located In or Immediately
Accessible to a Public Housing Site
(All health centers report this line)
<blank for demonstration>
Table 4 Cross-Table Considerations:
• The total patients reported by insurance type must match on Table 4 (Lines 7–12) and the Patients by ZIP
Code Table. For example, total Medicare patients on Table 4 (Line 9) must match the total of the Medicare
Column D on the Patients by ZIP Code Table.
• Charges and collections by payer on Table 9D relates to insurance enrollment on Table 4. For example,
dividing Medicaid revenue on Table 9D, Line 3, Column B by Total Medicaid Patients on Table 4, Line 8
equals the average collection per Medicaid patient.
• Reporting of managed care revenue on Table 9D relates to member months on Table 4. Dividing managed
care capitation revenue by member months equals average capitation per member per month (PMPM). For
example, dividing Medicaid capitated revenue (Table 9D, Line 2a, Column B − (c1 + c2 + c3 − c4)) by
Table 4, Line 13a, Column A equals Medicaid PMPM.
• If you submit Grant Reports, the total number of patients reported on the grant table(s) must be less than or
equal to the corresponding number on the Universal Report for each cell.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
55 2023 UDS MANUAL | Instructions for Table 5
Instructions for Table 5: Staffing and Utilization
Table 5 and the Selected Service Detail Addendum collect data on services provided to patients during the
calendar year.
Four lines have been added to provide more detailed data on pharmacy personnel.
TABLE 5: STAFFING AND UTILIZATION
This table provides a profile of health center personnel (Column A), the number of clinic (in-person) visits they
render (Column B), the number of virtual visits they render (Column B2), and the number of unduplicated
patients served in each service category (Column C).
Service categories that may reflect visits and patients include:
• Medical
• Dental
• Mental health
• Substance use disorder
• Other professional
• Vision
• Enabling
The patient count will often involve duplication across service categories (e.g., a patient may be reported in both
medical and dental patient counts), though it is always unduplicated within service categories (e.g., regardless of
number of medical visits or types of medical providers seen, the patient is only counted once as a medical
patient). This is unlike the Patients by ZIP Code Table and Tables 3A, 3B, and 4, where an unduplicated count of
patients across all service categories is reported.
The major staffing service categories on Table 5 are consistent with cost categories used for financial reporting
and provide adequate detail on personnel categories for program planning and evaluation purposes.
Personnel full-time equivalents (FTEs) in Column A is reported only on the Universal Report table, not the Grant
Report tables. Grant Reports provide data on patients served in whole or in part with section 330(h) (HCH),
section 330(g) (MHC), and/or section 330(i) (PHPC) funding and the visits they had during the year. This
includes all visits supported with either grant or non-grant funds.
PERSONNEL FULL-TIME EQUIVALENTS (FTES), COLUMN A
Table 5 includes personnel FTE for all individuals who work in programs and activities that are within Form 5B
of the health center’s scope of project for all service delivery sites included in the UDS. Report all personnel in
terms of annualized FTEs.
• Report FTEs of all personnel supporting health center operations defined by the scope of project in Column
A. Personnel may provide services on behalf of the health center under many different arrangements,
including but not limited to salaried full-time, salaried part-time, hourly wages,
National Health Service
Corps (NHSC) assignment, under contract (paid based on hours worked or FTE), interns, residents,
preceptors, or donated time (volunteers).

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
56 2023 UDS MANUAL | Instructions for Table 5
• DO NOT report FTEs for individuals who are paid by the health center on a fee-for-service basis in the FTE
column, because their work is not based on time and there is no basis for determining their hours. Visits with
providers paid through this arrangement are still reported in Column B or B2 and the patients who received
those services are reported in Column C.
Identifying Employment Type and Calculating FTEs
The following describes the basis for determining someone’s employment type for purposes of reporting on FTEs:
• One full-time equivalent (FTE = 1.00) describes personnel who worked the equivalent of full-time for one full
year. Each health center defines the number of hours for “full-time” work and may define it differently for
different positions.
• The FTE is based on employment contracts for providers and other personnel.
• In some health centers, different positions have different definitions of full time. Positions with different time
expectations should be calculated on whatever they have as a base for that position. Some positions, per
employment contracts, consider working 36 hours per week full time and would be considered 1.00 FTE. In
this case, an 18-hour-per-week personnel would be considered 0.50 FTE regardless of whether other
personnel in other positions work 40-hour weeks.
• The FTE of personnel receiving full-time benefits for the full year would be considered full-time = 1.00 FTE.
• Hourly personnel with no or reduced benefits who work more than full-time (i.e., overtime) will have an FTE
greater than 1.00.
• For personnel who do not receive all of the paid time off of full-time personnel (i.e., vacation, holidays, and
sick benefits), the effective FTE is calculated by dividing worked hours by adjusted full-time hours (full-time
hours minus paid time off hours that full-time personnel receive).
Reporting FTEs on the Appropriate Line on Table 5
Allocate all personnel time by function among the major service categories listed. DO NOT parse out the
components of an encounter. The nurse who handles a referral after a visit as a part of that visit would not be
allocated out of nursing. The nurse who collects vitals on a patient, who is then placed in the exam room, and later
provides instructions on wound care, for example, would not have a portion of the time counted as health
education—it is all a part of nursing.
Report an individual who is employed as a full-time provider for a full year as 1.00 FTE regardless of the number
of direct patient care hours they provide. Providers who have released time to compensate for on-call hours, have
weekly administrative sessions when they DO NOT see patients, or receive paid leave for continuing education or
other reasons are still considered full-time per their employment contract. Similarly, DO NOT count providers
who are routinely required to work more than 40 hours per week as more than 1.00 FTE.
Note: Count loan-repayment recipients as full-time. Note that the FQHC Medicare intermediary has different
definitions for full-time providers; these are NOT to be used for UDS reporting.
The time spent by providers performing tasks in what could be considered non-direct-service clinical activities,
such as charting, reviewing labs, filling or renewing prescriptions, returning phone calls, arranging for referrals,
participating in quality improvement (QI) activities, supervising, etc., is all considered part of their overall
medical care services time and should not be separately reported in a non-clinical support category.
The one exception to this rule is when a chief medical officer/medical director is engaged in non-clinical activities
at the corporate level (e.g., attending board of directors or senior management meetings, advocating for the
health center before the city council or Congress, writing grant applications, participating in labor negotiations,

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
57 2023 UDS MANUAL | Instructions for Table 5
negotiating fees with insurance companies), in which case time can be allocated to the non-clinical support
services category. This does not, however, include non-clinical activities in the medical area, such as supervising
the clinical personnel, chairing or attending clinical meetings, developing clinical schedules, or writing clinical
protocols.
Example FTE calculations are provided in the FAQ for Table 5 and Selected Service Detail Addendum
.
Personnel by Major Service Category
Personnel are distributed into categories that reflect the types of services they provide as independent providers.
Whenever possible, the contents of major service categories have been defined to be consistent with definitions
used by Medicare. The following summarizes the personnel categories; a more detailed, though not exhaustive,
list appears in Appendix A
.
Medical Care Services (Lines 1–15)
Physicians, nurse practitioners (NPs), physician assistants (PAs), and certified nurse midwives (CNMs) who are a
primary source of medical care delivery, as permitted under their license, are included as medical providers.
Supporting medical personnel include nurses and other medical, medical laboratory, and medical X-ray personnel.
• Physicians (Lines 1–7)
o Report physicians on Lines 1–7 consistent with their licensure. Physicians with dual boarding may be
allocated into two lines, such as internal medicine and pediatrics, based on time spent or patients seen, but
both provider FTE and visits must be allocated.
o Report licensed interns and residents on the line for the specialty designation they are working toward and
credit them with their own visits. (Thus, count a family practice intern as a family physician on Line 1.)
o DO NOT report psychiatrists, ophthalmologists, pathologists, or radiologists here. They are separately
reported on Lines 20a, 22a, 13, and 14, respectively.
o DO NOT report naturopaths, acupuncturists, community and behavioral health aides/practitioners, or
chiropractors on these lines. Report these providers on Line 22 (Other Professionals).
• Nurse Practitioners (Line 9a)
o Report NPs, advanced practice registered nurses (APRNs), and advanced practice nurses (APNs) on Line
9a.
o DO NOT report psychiatric NPs (included on Line 20b, Other Licensed Mental Health Providers) or
CNMs, (reported on Line 10) on this line.
• Physician Assistants (Line 9b)
o Report PAs on Line 9b.
o DO NOT include psychiatric PAs here (included on Line 20b, Other Licensed Mental Health Providers).
• Certified Nurse Midwives (Line 10)
o Report CNMs on Line 10.
• Nurses (Line 11)
o Report licensed registered nurses, licensed practical and vocational nurses, home health and visiting
nurses, clinical nurse specialists, and public health nurses.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
58 2023 UDS MANUAL | Instructions for Table 5
• Other Medical Personnel (Line 12)
o Report medical assistants, nurses’ aides, and all other personnel, including unlicensed interns or residents,
providing services in conjunction with services provided by a physician, NP, PA, CNM, or nurse.
o DO NOT report non-medical personnel here.
DO NOT report personnel dedicated to QI or HIT/EHR informatics here. Report them on Line 29b,
Quality Improvement Personnel.
DO NOT report patient health records or patient support personnel here. Report them on Line 32,
Patient Support Personnel.
• Laboratory Personnel (Line 13)
o Report pathologists, medical technologists, laboratory technicians and assistants, and phlebotomists.
o Some or all of nurses’ time may be in this category if they have dedicated times that they are assigned to
this responsibility.
o DO NOT report the time of a physician (except a pathologist) here.
• X-ray Personnel (Line 14)
o Report radiologists, X-ray technologists, and X-ray technicians.
o DO NOT include physician time (except radiologists) here, even if they were taking or reading X-rays or
performing sonograms.
Dental Services (Lines 16–19)
• Dentists (Line 16)
o Report general practitioners, oral surgeons, periodontists, and endodontists providing prevention,
assessment, or treatment of a dental problem, including restoration.
• Dental Hygienists (Line 17)
o Report licensed dental hygienists.
• Dental Therapists (Line 17a)
o Several states and American Indian or Alaska Native communities license dental therapists.
o Report personnel on this line only if they have a state license or tribal designation as such.
• Other Dental Personnel (Line 18)
o Report dental assistants, advanced dental assistants, aides, and technicians.
Behavioral Health Services
The term “behavioral health” is synonymous with the prevention or treatment of mental health and substance use
disorders. All visits, providers, and patients classified by health centers as “behavioral health” must be parsed into
mental health or substance use disorders. Centers may choose to identify all behavioral health services as Mental
Health Services if there is no way to reasonably split these services.
Mental Health Services (Lines 20a–20c)
Mental health services include psychiatric, psychological, psychosocial, or crisis intervention services.
• Psychiatrists (Line 20a)

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
59 2023 UDS MANUAL | Instructions for Table 5
• Licensed Clinical Psychologists (Line 20a1)
• Licensed Clinical Social Workers (Line 20a2)
• Other Licensed Mental Health Providers (Line 20b)
o Report other licensed mental health providers, including psychiatric social workers, psychiatric NPs,
family therapists, and other licensed master’s degree–prepared providers.
• Other Mental Health Personnel (Line 20c)
o Report unlicensed personnel and support personnel, including “certified” personnel, who provide
counseling or treatment, or who support mental health providers.
o Unlicensed interns or residents in any of the professions listed on Lines 20a through 20b are reported on
Line 20c, unless they possess a separate license under which they are practicing. Thus, a licensed clinical
social worker (LCSW) doing a psychology internship may be reported on Line 20a2 until they receive a
license to practice as a psychologist.
Substance Use Disorder Services (Line 21)
• Report personnel who provide substance use disorder services, including substance use disorder social
workers, psychiatric nurses, psychiatric social workers, mental health nurses, clinical psychologists, clinical
social workers, alcohol and drug abuse counselors, family therapists, and other individuals providing
substance use disorder counseling and/or treatment services.
• Neither licenses nor credentials are required by the UDS for substance use disorder personnel. Substance use
disorder providers are credentialed according to the health center’s standards.
• Report medical providers treating patients with substance use diagnoses in the medical services category on
Lines 1 through 10, NOT as substance use disorder providers. Additional information about substance use
disorder treatment by medical providers is collected in the Selected Service Detail Addendum
to this table.
• DO NOT report physicians, NPs, PAs, CNMs, or Certified Registered Nurse Anesthetists (CRNAs) who
completed the one-time training on substance use disorder treatment required under the Medication Access
and Training Expansion Act and have a current Drug Enforcement Administration (DEA) registration that
includes Schedule III authority to provide medications for opioid use disorder (MOUD) here. Report MOUD
providers on Lines 1–10 (if medical), Line 20a for psychiatrists, or Line 20b for psychiatric NPs. Additional
information about MOUD services is collected in Appendix E, Other Data Elements
.
Other Professional Health Services (Line 22)
Other professional personnel may provide an array of services and care important to primary and other care
delivery that support or complement the services of other providers.
• Report personnel who provide other professional health services. Some common professions include
occupational, speech, and physical therapists; registered dieticians; nutritionists; podiatrists; naturopaths;
chiropractors; acupuncturists; and community and behavioral health aides and practitioners. A more complete
list is included in Appendix A
.
• These professionals are generally credentialed and privileged by the health center’s governing board to act in
accordance with their approved job descriptions.
• DO NOT report other professionals working in the WIC programs here. Report WIC nutritionists and other
professionals working in WIC programs on Line 29a, Other Programs and Services Personnel.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
60 2023 UDS MANUAL | Instructions for Table 5
Vision Services (Lines 22a–22d)
Report providers who perform eye exams for detection, care, treatment, and prevention of vision problems,
including those that relate to chronic diseases such as diabetes, hypertension, thyroid disease, and arthritis, or for
the prescription of corrective lenses.
• Ophthalmologists (Line 22a)
o Report MDs specializing in the provision of medical and surgical eye care.
• Optometrists (Line 22b)
o Report doctors of optometry (OD) who provide routine eye care services.
• Other Vision Care Personnel (Line 22c)
o Report ophthalmologist and optometric assistants, aides, and technicians.
Pharmacy Services (Lines 23a–23d)
• Report personnel supporting pharmaceutical services.
• DO NOT report the time (or cost) of personnel spending all or part of their time in assisting patients to apply
for free drugs from pharmaceutical companies through pharmacy assistance programs (PAPs) here. Report
them on Line 27a, Eligibility Assistance Workers. If personnel work as a pharmacy assistant, for example,
and also provide PAP enrollment assistance, allocate time spent in each category.
• DO NOT include time for individuals who work at a 340B contract pharmacy, since they are paid fee-for-
service, and not based on time.
• DO NOT report personnel who manage pharmacy 340B contracts here. Report them on Line 30a as non-
clinical support personnel.
• Pharmacists (Line 23a)
o Report pharmacists supporting pharmaceutical services, such as dispensing medications prescribed by
health care providers, providing pertinent drug information to health care teams and providers, and
informing patients about proper usage of medications and side effects.
• Clinical Pharmacists (Line 23b)
o Report licensed clinical pharmacists, including board certified specialties (e.g., board certified
pharmacotherapy specialist, ambulatory care) on Line 23b. DO NOT allocate to other clinical or non-
clinical lines.
• Pharmacy Technicians (Line 23c)
o Report fully licensed pharmacy technicians.
• Other Pharmacy Personnel (Line 23d)
o Report pharmacist assistants and other supporting pharmaceutical services.
Enabling Services (Lines 24–29)
• Case Managers (Line 24)
o Report personnel who assist patients in the management of their health and social needs, including
assessment of patient medical and/or social service needs; establishment of service plans; and
maintenance of referral, tracking, and follow-up systems.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
61 2023 UDS MANUAL | Instructions for Table 5
o Include personnel who are trained as—and specifically called—case managers, as well as individuals
called care coordinators, referral coordinators, and other local titles.
o Case managers may provide health education and/or eligibility assistance in the course of their case
management functions. DO NOT parse out this time unless the personnel have dedicated time to other
enabling service categories.
• Health Education Specialists (Line 25)
o Report patient and community health educators with or without specific degrees.
• Outreach Workers (Line 26)
o Report personnel conducting case finding, education, or other services designed to identify potential
patients or clients and/or facilitate access or referral of potential health center patients to available health
center services.
• Transportation Workers (Line 27)
o Report personnel who provide transportation for patients (e.g., van drivers) or arrange for transportation
(e.g., for bus or taxi vouchers), including personnel who arrange for local transportation or longer-
distance transportation to major cities in extremely remote clinic locations.
• Eligibility Assistance Workers (Line 27a)
o Report personnel (e.g., patient navigators, certified assisters, eligibility workers) who provide assistance
in securing access to available health, social service, pharmacy, and other assistance programs, including
Medicaid, Medicare, WIC, Supplemental Security Income (SSI), food stamps through the Supplemental
Nutrition Assistance Program (SNAP), Temporary Assistance for Needy Families (TANF), PAPs, and
related assistance programs, as well as personnel hired under the HRSA Outreach and Enrollment grants.
• Interpretation Personnel (Line 27b)
o Report personnel whose full-time or dedicated time is devoted to translation and/or interpretation
services.
o DO NOT include the portion of the time a nurse, medical assistant, or other support personnel providing
interpretation, translation, or bilingual services during their other activities.
• Community Health Workers (Line 27c)
o Report lay members of communities who work in association with the local health care system in both
urban and rural environments and usually share ethnicity, language, socioeconomic status, and/or life
experiences with the community members they serve. Personnel may be called community health
workers, community health advisors, lay health advocates, promotoras, community health representatives,
peer health promoters, or peer health educators.
o They may perform some or all of the tasks of other enabling services workers. If some of their time is
dedicated to these other functions, report them on those lines.
o DO NOT include personnel better classified under other service categories, such as Other Medical
Personnel (Line 12) or Other Dental Personnel (Line 18).
• Personnel Performing Other Enabling Service Activities (Line 28)
o Report all other personnel performing enabling services not described above. Complete the “specify” field
to describe the personnel positions.
o If a service does not fit the strict descriptions for Lines 24 through 27c, its inclusion on Line 28 must
include a clear detailed statement of what is being reported.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
62 2023 UDS MANUAL | Instructions for Table 5
o DO NOT use enabling services, especially Other Enabling Services (Line 28), as a catchall, all-inclusive
category for services that are not included on other lines. Often, such services belong on Line 29a (Other
Programs and Related Services Personnel) or are services that are not separately reported on the UDS.
o Check such services with the UDS Support Center prior to submission.
Other Programs and Related Services Personnel (Line 29a)
Some health centers operate programs that (although within their scope of project and often important to the
overall health of their patients) are not directly a part of the listed medical, dental, behavioral, or other
professional health services (also referred to as “umbrella agencies”).
• Report personnel for these programs, such as WIC programs, job training programs, Head Start or Early Head
Start programs, shelters, housing programs, child care, frail elderly support programs, adult day health care
(ADHC) programs, fitness or exercise programs, public/retail pharmacies, etc., on this line. Complete the
“specify” field to describe the personnel positions.
Quality Improvement Personnel (Line 29b)
Although QI is a part of virtually all clinical and administrative positions, some individuals have specific
responsibility for the design and oversight of QI systems.
• Report individuals that spend all or a substantial portion of their time dedicated to these activities. They may
have clinical, information technology (IT), or research backgrounds, and may include QI nurses, data
specialists, statisticians, and designers of HIT (including EHRs and electronic medical records [EMRs]).
• Report personnel who support HIT to the extent that they are working with the QI system on Line 29b.
• Continue to report personnel who document services in the HIT in the appropriate service category, not here.
• DO NOT include on this line the time of providers, such as physicians or dentists, who are also involved in
the QI process. Their time is to remain on the service category lines.
Non-Clinical Support Services (Lines 30a–32)
• Management and Support Personnel (Line 30a)
o Report the management team, including the CEO, chief financial officer (CFO), chief information officer
(CIO), chief medical officer (CMO), chief operations officer (COO), and human resources (HR) director,
as well as other non-clinical support and office support personnel.
o For medical directors or other personnel whose time is split between clinical and non-clinical activities,
report here only that portion of their FTE corresponding to the corporate management function. (See
limits on non-clinical time under Personnel Full-Time Equivalents
.)
• Fiscal and Billing Personnel (Line 30b)
o Report personnel performing accounting and billing functions in support of health center operations for
services performed within the scope of project.
o DO NOT include the CFO here. Report the CFO on Line 30a, Management and Support Personnel.
• IT Personnel (Line 30c)
o Report information systems technical personnel who maintain and operate the computing systems that
support functions performed within the scope of project.
o Report IT personnel managing the hardware and software of an HIT (including EHR/EMR) system on
Line 30c.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
63 2023 UDS MANUAL | Instructions for Table 5
o Report IT personnel performing data entry as well as providing training and technical assistance functions
as part of the other medical personnel or appropriate service category for which they perform these
functions.
o DO NOT report IT personnel designing medical forms and conducting analysis of HIT data here. Report
as part of the QI functions on Line 29b.
• Facility Personnel (Line 31)
o Report personnel with facility support and maintenance responsibilities, including custodians,
housekeeping personnel, groundskeepers, security personnel, and other maintenance personnel. If facility
functions are contracted (e.g., janitorial services), DO NOT include an FTE; but report the contracted
costs on Line 14 on Table 8A.
• Patient Services Support Personnel (Line 32)
o Report intake personnel, front desk personnel, and patient health records personnel.
Note: The non-clinical category for this report is more comprehensive than that used in some other program
definitions and includes all such personnel working in a health center, whether an individual’s salary was
supported by the BPHC grant or other funds included in the scope of project. Where appropriate, and when
identifiable, report personnel included in a health center’s federally approved budget indirect cost rate here.
VISITS, COLUMNS B AND B2
Report only clinic (in-person) and virtual visits that meet the countable visit definitions, as described in the
Instructions for Tables that Report Visits, Patients, and Providers
section of the UDS Manual.
Report Clinic Visits (Column B) and Virtual Visits (Column B2). These are mutually exclusive, and total visits
are calculated by adding Columns B and B2.
Clinic Visits, Column B
• Report any documented in-person encounter between a patient and a licensed or credentialed provider who
exercises their independent professional judgment in the provision of services to the patient at that time as a
visit in Column B.
• Report all such visits that occurred during the calendar year rendered by salaried, contracted, or volunteer
providers. Report visits on the same line as the provider who conducted the visit. Most visits reported in
Column B will be provided by personnel identified in Column A.
• Visits purchased from contracted providers on a fee-for-service basis should also be reported, even though the
FTE of the provider is not reported.
Note: DO N
OT report encounters that are screenings, tests, or vaccines (such as for COVID-19) as visits. Only
report encounters that meet the full definition as a visit.
Virtual Visits, Column B2
• Report any documented virtual (telemedicine) encounter between a patient and a licensed or credentialed
provider who exercises their independent professional judgment in the provision of services to the patient at
that time as a visit in Column B2.
• Report all such visits that occurred during the calendar year rendered by salaried, contracted, or volunteer
personnel. Report visits on the same line as the provider who conducted the visit. Most visits reported in
Column B2 will be provided by personnel identified in Column A.
• Virtual visits purchased from contracted providers on a fee-for-service basis should also be reported.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
64 2023 UDS MANUAL | Instructions for Table 5
Note: Telemedicine is a growing model of care delivery. It is important to remember that payer, state, and federal
telehealth definitions, regulations, and billing requirements regarding the acceptable modes of care delivery, types
of providers, informed consent, and location of the patient and/or provider are not applicable in determining
virtual patient visits for UDS reporting.
Virtual Visit Considerations
• Virtual visit reporting should be consistent with the health center’s scope of project.
• Virtual visits must meet the countable visit
definition.
• All reporting requirements regarding multiple visits in the same service category in the same day apply,
except that two different providers based out of two different in-scope service delivery sites may be reported
as two visits.
• Report virtual visits where:
o The health center provider provided care to a patient who was elsewhere (i.e., not physically at the health
center).
o The health center patient received services through telemedicine by a non–health center provider paid for
by the health center or by a volunteer provider who was at the health center.
o The provider was not physically present at the health center when providing care to the patient, who was
in a separate location. The provider must have had remote access to the patient’s health record at the time
of the visit to review it and record their activities.
o Interactive, synchronous audio or audio-video telecommunication systems that permit real-time
communication between the provider and the patient were used.
o Services are coded and charged as telehealth services, even if a third-party payer does not recognize or
pay for such services. Generally, these charges would be similar to a comparable clinic (in-person) visit
charge.
Note:
Use codes that will result in accurate identification of virtual visits. These include telehealth-specific codes
with the CPT or Healthcare Common Procedure Coding System (HCPCS) codes such as G0071, G0406-G0408,
G0425-G0427, G2025, modifier “.95,” or Place of Service code “02” to identify virtual visits.
• DO NOT report:
o as a virtual visit situations in which the health center does not pay for virtual services provided by a non–
health center provider (referral).
o other modes of telemedicine services (e.g., store and forward, remote patient monitoring, mobile health)
or provider-to-provider consultations.
o a separate clinic (in-person) visit at the originating clinic.
Visits Purchased from Non-Personnel Providers on a Fee-For-Service Basis
Report these visits in Column B (clinic) or B2 (virtual) even though no corresponding FTEs are included in
Column A. To count, the visit must meet the following criteria:
• the service was provided to a patient of the health center by a provider who is not part of the health center’s
personnel (neither salaried, volunteer, nor contracted on the basis of time worked) although they meet the
center’s credentialing policies,
• the service was paid for in full by the health center, and

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
65 2023 UDS MANUAL | Instructions for Table 5
• the service otherwise met the definition of a visit.
DO NOT include unpaid referrals, referrals where a third party (e.g., the patient’s insurance company) will make
the payment directly to the provider, or referrals where only nominal amounts, including facility fees, are paid
although the negotiated payment may be less than the provider’s “usual, customary, and reasonable” (UCR) rates.
Visit Considerations by Personnel Line
Nurses, Line 11
• Services may be provided under standing orders of a medical provider, under specific instructions from a
previous visit, or under the general supervision of a physician, NP, PA, or CNM who has no direct encounter
with the patient during the visit. These services must meet the requirement of exercising independent
professional judgment.
• Report nurse visits that meet all visit criteria. See instructions for Countable Visits
. Most patient services
provided by a nurse DO NOT meet the full visit criteria.
• Report triage services provided by nurses and visiting nurse services when a nurse sees patients independently
in the patients’ homes to evaluate their condition(s).
• Report visits charged and coded as CPT 99211 only when all components of visit requirements were met.
• DO NOT report a service if it is a follow-up or completion of services from another visit (e.g., nurse calls to
check up on how a patient is doing after a visit, nurse checks wound or removes sutures, nurse provides
vaccines), even if it occurs at a later date.
• DO NOT report encounters with a nurse where the primary purpose is to conduct a lab test, give an injection,
or dispense or administer a drug, regardless of the level of observation needed, as a visit.
• Most states prohibit a licensed vocational nurse or licensed practical nurse from exercising independent
professional judgment; DO NOT count visits for them.
Dentists, dental hygienists, and dental therapists, Lines 16, 17, and 17a
• Report only one visit per patient per day, regardless of the number of dental providers who provide services
(e.g., dentist and dental hygienist both see the patient) or the volume of service (i.e., number of procedures)
provided.
• DO NOT report the application of dental varnishes, fluoride treatments, or dental screenings, absent other
comprehensive dental services, as a visit.
• DO NOT report as a dental visit medical providers who examine a patient’s dentition or provide fluoride
treatments.
• DO NOT report as a dental visit a phone call between the patient and provider for a check up on a completed
procedure or service.
• DO NOT credit services of dental students or anyone other than a licensed dental provider with dental visits,
even if these individuals are working under the supervision of a licensed dental provider.
• Exception: Report the visits of a supervising dentist’s student (i.e., the dentist is overseeing dental students
enrolled in a graduate education program leading to a license as a dentist) as long as the supervising dentist:
o has no other responsibilities, including the supervision of other personnel, at the time services are
furnished by the students;
o has primary responsibility for the patients;

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
66 2023 UDS MANUAL | Instructions for Table 5
o reviews the care furnished by the students during or immediately after each visit; and
o documents the extent of their participation in the review and direction of the services furnished to each
patient.
Other mental health, Line 20c
• Report visits with unlicensed mental health personnel regardless of any billing practices at the center. DO
NOT report their visits elsewhere.
Substance use disorder, Line 21
• In programs that include the regular use of narcotic agonists or antagonists or other medications on a regular
basis (daily, every three days, weekly, etc.), report only the individualized or group counseling services as
visits.
• DO NOT report the counseling by medical or psychiatric providers of patients to determine or diagnose their
medical needs, including medication assistance and substance use disorder visits. Report as medical or
psychiatry visits based on the provider of these services.
• DO NOT report the dispensing of drugs, regardless of the level of oversight that occurs during that activity.
Other professional, Line 22
• Report visits by other professional health service providers included in Appendix A
.
• Describe these services in a clear, detailed statement using the “specify” box.
• Check the reporting of other professional services with the UDS Support Center or UDS Reviewer.
Vision services, Lines 22a–22d
• DO NOT report the services of students or anyone other than a licensed vision service provider as vision
services visits.
• DO NOT report retinography (imaging of the retina), whether performed by a licensed vision service provider
or anyone else, as a visit unless accompanied by a comprehensive vision exam.
• DO NOT report fitting glasses as a visit, regardless of who performs the fitting.
Pharmacy, Line 23
• Pharmacy personnel are not considered providers on the UDS (see Appendix A
), and therefore visits are NOT
reported.
• Some states license clinical pharmacists whose scope of practice may include ordering labs and reviewing and
altering medications or dosages. Despite this expanded scope of practice, DO NOT report clinical pharmacist
encounters with patients as visits.
Case managers, Line 24
• Case management visits must be documented in the patient’s health record.
• When a case manager serves an entire family (e.g., helping with housing or Medicaid eligibility), report only
one visit, generally for an adult member of the family, regardless of documentation in other charts.
• Case management is rarely the only type of service provided to a patient during the year.
• Case managers often contact third parties in the provision of their services. DO NOT count these encounters.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
67 2023 UDS MANUAL | Instructions for Table 5
Health education, Line 25
• Report only services provided one-on-one with the patient.
• Health education is provided to support the delivery of other health care services and is rarely the only type of
service provided to a patient during the year.
• DO NOT report group or community education classes or visits.
DO NOT Report Visits or Patients for Services Provided by the Following:
• Other Medical Personnel, Line 12
• Laboratory Personnel, Line 13
• X-ray Personnel, Line 14
• Other Dental Personnel, Line 18
• Other Vision Care Personnel, Line 22c
• Pharmacy Personnel, Line 23
• Outreach Workers, Line 26
• Transportation Personnel, Line 27
• Eligibility Assistance Workers, Line 27a
• Interpretation Personnel, Line 27b
• Community Health Workers, Line 27c
• Other Enabling Services, Line 28
• Other Programs and Services, Line 29a
• Quality Improvement Personnel, Line 29b
• Management and Support Personnel, Line 30a
• Fiscal and Billing Personnel, Line 30b
• IT Personnel, Line 30c
• Facility Personnel, Line 31
• Patient Support Personnel, Line 32
Additionally, some encounters cannot be reported as countable visits regardless of who provides them. Please
review the Services and Individuals NOT Reported on the UDS Report
section for specifics.
Note: Columns B and B2 are grayed out on the lines listed above.
PATIENTS, COLUMN C
A patient is an individual who has at least one countable visit during the calendar year. For further details, see the
Instructions for Tables that Report Visits, Patients, and Providers
section.
• Report an unduplicated patient count in Column C for each of the seven categories of services shown below
for which patients had visits reported in Columns B or B2 during the calendar year.
o Medical services (Line 15)
o Dental services (Line 19)
o Mental health services (Line 20)
o Substance use disorder services (Line 21)
o Vision services (Line 22d)
o Other professional services (Line 22)
o Enabling services (Line 29)

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
68 2023 UDS MANUAL | Instructions for Table 5
• Report an individual only once as a patient in each service category (e.g., medical, dental) under which they
received services, regardless of the number of visits they had or the different providers they saw during the
year.
• Because patients must have at least one countable visit, the number of patients cannot exceed the number of
visits.
• Patients reported on Table 5 must be included as patients on the demographics tables: Patients by ZIP Code
Table and Tables 3A, 3B, and 4.
• DO NOT report individuals who only receive services for which no visits are generated (e.g., laboratory,
imaging, pharmacy, transportation, and outreach).
Note: Column C is grayed out on the detail lines within service categories.
SELECTED SERVICE DETAIL ADDENDUM
The Selected Service Detail Addendum to Table 5 provides data on integrated primary care and behavioral health
treatment services. Integrated behavioral health reported in the addendum includes:
• mental health services provided by medical providers during medical visits,
• substance use disorder services provided by medical providers during medical visits, and
• substance use disorder services provided by mental health providers during mental health visits.
The addendum is reported on the Universal Report only.
The information reported in the Selected Service Detail Addendum only reflects medical providers and their
mental health services and medical or mental health providers and their substance use disorder treatment services
that are NOT already being reported in the mental health and/or substance use disorder sections on the
main part of Table 5. The sum of mental health and substance use disorder services visits reported in the main
part of Table 5 and the addendum to Table 5 provide a combined count of mental health and substance use
disorder services provided.
The Selected Service Detail Addendum is divided into two service categories: mental health and substance use
disorder detail.
• The Mental Health Services Detail (by type of medical provider), Lines 20a01–20a04, is a subset of medical
visits and patients reported on Lines 1–10 in the main section of Table 5.
• The Substance Use Disorder Detail (by type of medical provider), Lines 21a–21d, is a subset of medical visits
and patients reported on Lines 1–10 in the main section of Table 5.
• The Substance Use Disorder Detail (by type of mental health provider), Lines 21e–21h, is a subset of mental
health visits and patients reported on Lines 20a–20b in the main section of Table 5.
All visits reported in the addendum will also be included in the main part of Table 5 as either medical or mental
health visits. Some visits provided by medical providers may include both mental health and substance use
disorder treatment and will be counted in each section of the addendum, in addition to being counted as a medical
visit in the main part of Table 5.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
69 2023 UDS MANUAL | Instructions for Table 5
Note: To identify visits where a mental health or substance use disorder treatment service may have been
rendered, include at a minimum all visits in which the reported providers coded ICD-10 codes specified on Table
6A, Lines 18 through 19a for substance use disorder treatment provided as part of a mental health or medical
visit and Lines 20a through 20d for mental health treatment provided as part of a medical visit.
Providers, Column A1
• Report the number of individual providers (not FTE) by type who provided mental health and/or substance
use disorder services. Medical providers can be counted once in each section if they provide both mental
health and substance use disorder services.
• If the provider is a contract provider paid by visit or service, DO NOT count an FTE on the main part of Table
5, but count the provider in the addendum.
Clinic Visits, Column B
• Report the number of clinic (in-person) visits, by provider type, where the service in whole or in part included
treatment for mental health (on Lines 20a01 through 20a04) or substance use disorder services (on Lines 21a
through 21h).
Virtual Visits, Column B2
• Report the number of virtual visits, by provider type, where the service in whole or in part included treatment
for mental health (on Lines 20a01 through 20a04) or substance use disorder services (on Lines 21a through
21h).
Patients, Column C
• Report the number of patients seen for a clinic (in-person) or virtual mental health or substance use disorder
service by provider(s) in the given line.
• Report patients (and their visits) for each type of provider listed who were seen during the year for these
services. This may result in the same patient appearing on more than one line in the addendum.
FAQ FOR TABLE 5 AND SELECTED SERVICE DETAIL ADDENDUM
1. How do we determine FTE?
Use employment contracts to determine FTE. For example, a physician hired as full-time personnel who, per
their employment contract, is only required to work four 9-hour sessions (36 hours) per week, is considered
full-time.
2. Our physicians work 35-hour weeks. Do we report as 0.875 (35 divided by 40) FTE?
No. Count them as 1.00 FTE. BPHC does not require 40-hour workweeks. Use whatever workweek time is
considered full-time at your organization. For example, some organizations use 2,080 hours, others use 1,820,
and others may have other standards for determining what is full-time.
3. Do we calculate FTE for personnel with no or reduced benefits the same way we do for personnel
receiving full benefits?
No. If personnel receive no or reduced benefits, calculate FTE based on paid hours. For example, in a health
center that has a 40-hour workweek (2,080 hours/year), an individual who works 20 hours per week all year
(i.e., 50% time) is reported as 0.50 FTE; an individual who works full-time for 4 months out of the year is

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
70 2023 UDS MANUAL | Instructions for Table 5
reported as 0.33 FTE (4 months ÷ 12 months). If an individual with no benefits works 2,200 hours out of
2,080 full-time hours, report as 1.06 FTE.
4. How do I report the FTEs for a provider who regularly sees patients 75% of the time and covers after-
hours call for the remaining 25% of their salary?
Report personnel who are hired as full-time providers as 1.00 FTE regardless of the number of direct patient
care hours they provide. Count as 1.00 FTE providers hired as full-time who have released time to
compensate for on-call hours, who have released time to compensate for hours spent on clinical committees,
or who receive leave for continuing education or other activities.
DO NOT adjust for the time spent by a physician (for example) while not in contact with the patient, such as
charting, reviewing labs, filling prescriptions, returning phone calls, or arranging for referrals. These tasks are
considered part of their time as a physician. The exception to this rule is when a medical director or chief
medical officer is engaged in non-clinical activities at the corporate level, in which case time is allocated to
the non-clinical category. This does not, however, include non-clinical activities in the medical area, such as
chairing or attending meetings, supervising personnel, writing clinical protocols, designing formularies,
setting hours, or approving specialty referrals.
5. Our nurses perform services that cross service categories. Do we allocate the FTE and visit activity
accordingly?
That depends on if their time is distinctly allocated by function among the major service categories. If, for
example, a full-time nurse provides direct medical services and provides some patient education while seeing
the patient for medical care, they would be counted as 1.00 FTE on Line 11 (Nurses). If that nurse provided
case management services during 10 dedicated hours per week and provided medical care services for the
other 30 hours per week, the time would be allocated as 0.25 FTE case manager (Line 24) and 0.75 FTE nurse
(Line 11). Another example includes a nurse who dedicates 20 hours to medical care and 20 hours to
providing health education each week would split their 1.00 FTE, with 0.50 FTE as a medical nurse and 0.50
FTE as a health educator.
6. If I report costs for case management services on Table 8A, do I have to report case managers on
Table 5?
If a health center reports costs for case management services, one would expect to see case managers reported
on Table 5, unless the service was contracted with no personnel time specifically identified. Similarly, if there
are personnel on Table 5, one would expect costs on Table 8A unless personnel are volunteers. Some services
DO NOT involve personnel. Spending funds on bus tokens, for example, would involve transportation costs
on Table 8A, but no personnel on Table 5.
7. How are contracted personnel and their activities reported on Table 5?
If the contracted personnel are paid based on time worked (for example, one day per week), report the FTE on
Table 5, Column A, and report the visits and patients receiving services from this provider. (See Appendix B
for a more complete discussion of calculating the FTE of these providers.) If the contracted personnel are paid
on a fee-for-service basis, DO NOT report FTE on Table 5, Column A, but report the visits and patients. This
may require additional explanation in your UDS Report to clarify why visits and patients are reported, but no
FTE.
8. How should activity be reported on Table 5 for behavioral health providers who provide both mental
health and substance use disorder services?
Some health centers have integrated the positions of mental health provider and substance use disorder
provider into a single position, which they call a behavioral health provider. In this instance, the health center

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
71 2023 UDS MANUAL | Instructions for Table 5
has two choices. The first is to assert that substance use disorder problems are mental health problems and
classify its behavioral health personnel as mental health personnel on Lines 20a, 20a1, 20a2, 20b, or 20c.
Another method is to carefully record the time and activities of these dual function providers. In this case,
identify each visit as either a mental health visit or a substance use disorder visit so the patients and visits can
be correctly classified. In addition, keep track of providers’ time so that FTEs on Table 5 (and associated
costs on Table 8A) can be accurately allocated and recorded to the appropriate line.
9. If a psychiatric NP provides mental health and substance use disorder services to the same patient
during a visit, how should we count this?
Report the visit under mental health in the main part of Table 5. DO NOT count the visits as one of each type.
In the addendum, separately report the substance use disorder service provided by the mental health personnel
during the visits. Classify the provider and costs (on Table 8A) as mental health.
10. Do I count the time of volunteer providers, interns, or residents?
Yes. Volunteers, interns, and residents are licensed practitioners, and their time is counted like that of any
other practitioner. Note, however, that some may work shorter days because they are in educational sessions,
may have more vacation time or other time off than other practitioners, or, in the case of volunteers, DO NOT
have vacations or holidays. This would make them less than full-time. See the more complete discussion of
counting volunteers, interns, and residents in Appendix B
.
11. We contract with many licensed physicians to read our test results: an ophthalmologist reads the
retinal photos that our medical assistant takes, a radiologist over-reads the X-rays that our X-ray tech
takes, the outside laboratory’s pathologist provides the test results from their machines, and a
consulting cardiologist confirms findings of our electrocardiograms (EKGs). Should we report them as
personnel, and do we report what they do as visits?
Report the costs for tests on Table 8A.
DO NOT report these activities, which are important to the provision of comprehensive care to patients, as
visits.
Tests are NOT counted as visits anywhere in the UDS.
DO NOT report the time (FTE) of any individual who is working on a contract basis when the payment is not
for their time worked but, rather, for the activity that they perform.
Under some circumstances, the EHBs may identify a system edit (costs with no personnel) that you will need
to explain.
12. Where do we report community health workers that we employ?
Report personnel with responsibility as community health workers on Line 27c, as described in the
Enabling
Services section. If, however, you are using this term to describe someone who is performing the tasks
normally associated with a medical assistant, an outreach worker, or another job title, count them in the
corresponding category.
13. Where do we report medical providers whose only activity at a visit is providing MOUD?
MOUD provided by a medical provider is to be counted as medical. Report this activity on the line of the
credentialed personnel providing this treatment (physicians are counted in medical [Lines 1–8], even if they

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
72 2023 UDS MANUAL | Instructions for Table 5
only provide substance use disorder services at the visit). Additionally, report the activity in the substance use
disorder section of the addendum (physicians are counted on Line 21a of the addendum).
DO NOT count them on the substance use disorder line of the main part of Table 5.
14. How do I count participants in a group session?
Only group treatment sessions for substance use disorders, mental health, or behavioral health may be
counted. The visit must be recorded in each participant’s chart. Each patient charted in a group session must
be billed and the service must be paid consistent with health center policy by either the patient, insurance, or
another contract maintained by the health center. If some patients or visits are billed and others are not, count
only those that are billed.
DO NOT count a group encounter with a patient that is not recorded in a patient health record. DO NOT
report group medical visits or group health education visits. Although in some instances they may be billable,
the UDS specifically does not count these as visits.
15. Are virtual/telemedicine visits only permitted after a clinic (in-person) visit at the health center?
No, although virtual visits may occur after a clinic (in-person) visit. If the first or only visit is a countable
virtual visit, the health center must register the patient and collect and report all relevant demographic,
service, clinical, and financial data on the UDS tables.
16. Should the total number of patients reported on Table 3A be equal to the sum of the several types of
service patients on the main part of Table 5?
Not unless you provide only one type of service to a patient. On Table 5, report patients for each type of
service received. For example, count a patient who receives both medical and dental services once as a
medical patient on Line 15 and once as a dental patient on Line 19.
17. Should a patient who received only a medication refill for a mental health condition be counted on the
addendum of Table 5?
No. If medication refills were the only services provided, the service will NOT be considered a visit, and the
patient and service will NOT be counted on the main part of Table 5 or the addendum to Table 5. Only count
services that fully meet the countable visit
definition.
The addendum is intended to capture treatment services for mental health (by medical providers) and
substance use (by medical and mental health providers). DO NOT include services that only provide mental
health or substance use disorder screenings, medication delivery or refills, patient education, referral, or case
management.
18. Which provider types and what activity are included in the addendum?
Medical providers who provide mental health or substance use treatment are included in the addendum.
Mental health providers who provide substance use treatment are also included in the addendum. Examples of
provider activity reported in the addendum include:
• A physician who sees a patient for treatment of depression.
• An NP who is seeing a patient for diabetes and who is also treating them for signs of anxiety.
• A PA providing MOUD services to a patient with opioid use disorder.


UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
74 2023 UDS MANUAL | Instructions for Table 5
TABLE 5: STAFFING AND UTILIZATION
Calendar Year: January 1, 2023, through December 31, 2023
Line Personnel by Major Service Category FTEs (a)
Clinic Visits
(b)
Virtual
Visits (b2)
Patients (c)
1
Family Physicians
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<cell not reported>
2
General Practitioners
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<cell not reported>
3
Internists
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<cell not reported>
4
Obstetrician/Gynecologists
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<cell not reported>
5
Pediatricians
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<cell not reported>
7
Other Specialty Physicians
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<cell not reported>
8
Total Physicians (Lines 1–7)
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<cell not reported>
9a
Nurse Practitioners
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<cell not reported>
9b
Physician Assistants
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<cell not reported>
10
Certified Nurse Midwives
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<cell not reported>
10a
Total NPs, PAs, and CNMs (Lines 9a–10)
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<cell not reported>
11
Nurses
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<cell not reported>
12
Other Medical Personnel
<blank for demonstration>
<cell not reported>
<cell not reported>
<cell not reported>
13
Laboratory Personnel
<blank for demonstration>
<cell not reported>
<cell not reported>
<cell not reported>
14
X-ray Personnel
<blank for demonstration>
<cell not reported>
<cell not reported>
<cell not reported>
15
Total Medical Care Services (Lines 8 + 10a–
14)
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
16
Dentists
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<cell not reported>
17
Dental Hygienists
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<cell not reported>
17a
Dental Therapists
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<cell not reported>
18
Other Dental Personnel
<blank for demonstration>
<cell not reported>
<cell not reported>
<cell not reported>
19
Total Dental Services (Lines 16–18)
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
20a
Psychiatrists
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<cell not reported>
20a1
Licensed Clinical Psychologists
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<cell not reported>
20a2
Licensed Clinical Social Workers
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<cell not reported>
20b
Other Licensed Mental Health Providers
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<cell not reported>
20c
Other Mental Health Personnel
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<cell not reported>
20
Total Mental Health Services (Lines 20a–c)
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
21
Substance Use Disorder Services
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
22
Other Professional Services (specify___)
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
75 2023 UDS MANUAL | Instructions for Table 5
TABLE 5: STAFFING AND UTILIZATION (CONTINUED)
Calendar Year: January 1, 2023, through December 31, 2023
Line Personnel by Major Service Category FTEs (a)
Clinic Visits
(b)
Virtual
Visits (b2)
Patients (c)
22a
Ophthalmologists
<blank for
demonstration>
<blank for demonstration>
<blank for
demonstration>
<cell not reported>
22b
Optometrists
<blank for demonstration>
<blank for demonstration>
<blank for
demonstration>
<cell not reported>
22c
Other Vision Care Personnel
<blank for demonstration>
<cell not reported>
<cell not reported>
<cell not reported>
22d
Total Vision Services (Lines 22a–c)
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
23a
Pharmacists
23b
Clinical Pharmacists
23c
Pharmacy Technicians
23d
Other Pharmacy Personnel
23
Pharmacy Personnel (Lines 23a–d)
<blank for demonstration>
<cell not reported>
<cell not reported>
<cell not reported>
24
Case Managers
<blank for demonstration>
<blank for
demonstration>
<blank for
demonstration>
<cell not reported>
25
Health Education Specialists
<blank for demonstration>
<blank for
demonstration>
<blank for
demonstration>
<cell not reported>
26
Outreach Workers
<blank for demonstration>
<cell not reported>
<cell not reported>
<cell not reported>
27
Transportation Personnel
<blank for demonstration>
<cell not reported>
<cell not reported>
<cell not reported>
27a
Eligibility Assistance Workers
<blank for demonstration>
<cell not reported>
<cell not reported>
<cell not reported>
27b
Interpretation Personnel
<blank for demonstration>
<cell not reported>
<cell not reported>
<cell not reported>
27c
Community Health Workers
<blank for demonstration>
<cell not reported>
<cell not reported>
<cell not reported>
28
Other Enabling Services (specify___)
<blank for demonstration>
<cell not reported>
<cell not reported>
<cell not reported>
29
Total Enabling Services (Lines 24–28)
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
29a
Other Programs and Services (specify___)
<blank for demonstration>
<cell not reported>
<cell not reported>
<cell not reported>
29b
Quality Improvement Personnel
<blank for demonstration>
<cell not reported>
<cell not reported>
<cell not reported>
30a
Management and Support Personnel
<blank for demonstration>
<cell not reported>
<cell not reported>
<cell not reported>
30b
Fiscal and Billing Personnel
<blank for demonstration>
<cell not reported>
<cell not reported>
<cell not reported>
30c
IT Personnel
<blank for demonstration>
<cell not reported>
<cell not reported>
<cell not reported>
31
Facility Personnel
<blank for demonstration>
<cell not reported>
<cell not reported>
<cell not reported>
32
Patient Support Personnel
<blank for demonstration>
<cell not reported>
<cell not reported>
<cell not reported>
33
Total Facility and Non-Clinical Support
Personnel (Lines 30a–32)
<blank for demonstration>
<cell not reported>
<cell not reported>
<cell not reported>
34
Grand Total (Lines
15+19+20+21+22+22d+23+29+29a+29b+33)
<blank for demonstration>
<blank for
demonstration>
<blank for
demonstration>
<cell not reported>

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
76 2023 UDS MANUAL | Instructions for Table 5
TABLE 5: SELECTED SERVICE DETAIL ADDENDUM
Calendar Year: January 1, 2023, through December 31, 2023
Line
Personnel by Major Service Category:
Mental Health Service Detail
Personnel
(a1)
Clinic Visits
(b)
Virtual
Visits (b2)
Patients (c)
20a01
Physicians (other than Psychiatrists)
<blank for
demonstration>
<blank for demonstration>
<blank for
demonstration>
<blank for
demonstration>
20a02
Nurse Practitioners
<blank for
demonstration>
<blank for demonstration>
<blank for
demonstration>
<blank for
demonstration>
20a03
Physician Assistants
<blank for
demonstration>
<blank for demonstration>
<blank for
demonstration>
<blank for
demonstration>
20a04
Certified Nurse Midwives
<blank for
demonstration>
<blank for demonstration>
<blank for
demonstration>
<blank for
demonstration>
Line
Personnel by Major Service Category:
Substance Use Disorder Detail
Personnel
(a1)
Clinic Visits
(b)
Virtual
Visits (b2)
Patients (c)
21a
Physicians (other than Psychiatrists)
<blank for
demonstration>
<blank for demonstration>
<blank for
demonstration>
<blank for
demonstration>
21b
Nurse Practitioners (Medical)
<blank for
demonstration>
<blank for demonstration>
<blank for
demonstration>
<blank for
demonstration>
21c
Physician Assistants
<blank for
demonstration>
<blank for demonstration>
<blank for
demonstration>
<blank for
demonstration>
21d
Certified Nurse Midwives
<blank for
demonstration>
<blank for demonstration>
<blank for
demonstration>
<blank for
demonstration>
21e
Psychiatrists
<blank for
demonstration>
<blank for demonstration>
<blank for
demonstration>
<blank for
demonstration>
21f
Licensed Clinical Psychologists
<blank for
demonstration>
<blank for demonstration>
<blank for
demonstration>
<blank for
demonstration>
21g
Licensed Clinical Social Workers
<blank for
demonstration>
<blank for demonstration>
<blank for
demonstration>
<blank for
demonstration>
21h
Other Licensed Mental Health Providers
<blank for
demonstration>
<blank for demonstration>
<blank for
demonstration>
<blank for
demonstration>
Table 5 and Addendum Cross-Table Considerations:
• Total patients on Table 5, Column C, should be greater than the total number of patients on Table 3A (unless
only one type of service is offered at the health center or patients receive only one kind of service).
• Patients with medical visits on Table 5 are generally eligible for inclusion in eCQMs reported on Tables 6B
and 7.
• The personnel on Table 5 is routinely compared to the costs on Table 8A. See the crosswalk of comparable
fields in Appendix B
.
• Billable visits reported on Table 5 should relate to patient charges reported on Table 9D.
• If you submit Grant Reports, the total number of patients and visits reported on the grant table must be less
than or equal to the corresponding number on the Universal Report for each cell.
• Table 6A activity reported for substance use disorder and mental health treatment are compared to the Table 5
addendum and the main part of Table 5 mental health and substance use lines.
• Visits and patients reported on the Table 5 Selected Service Detail Addendum must also be included in the
main part of Table 5, medical plus mental health lines.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
77 2023 UDS MANUAL | Instructions for Table 6A
Instructions for Table 6A: Selected Diagnoses and Services
Rendered
This table collects data on selected diagnoses and selected services rendered to health center patients. The data
source for this table is your billing system, lab reports, and/or other information captured in your HIT systems or
EHRs.
Table 6A does not reflect the full range of diagnoses and services rendered by a health center. The selected
diagnoses and services represent those that are prevalent among Health Center Program patients, have been
regarded as sentinel indicators of access to primary care, and/or are of special interest to HRSA.
Several notable changes have been made to Table 6A, as outlined below:
• Some diagnosis and service codes have been updated. All changes are included in the table and outlined in the
“Table 6A Code Changes” file found on the UDS Clinical Care Resources webpage.
• A new line has been added to report childhood developmental screenings and evaluation services.
• Value sets from the Value Set Authority Center (VSAC) have been added to diagnosis and service codes,
where available.
• In addition to submitting this table as described below within the EHBs, health centers may voluntarily
submit de-identified patient-level report data using Health Level Seven (HL7®) Fast Healthcare
Interoperability Resources (FHIR®) R4 standards for this table.
SELECTED DIAGNOSES, LINES 1–20F
Lines 1 through 20f present the name and applicable ICD-10-CM and value set codes for the diagnosis or
diagnostic range/group. Wherever possible, diagnoses have been grouped into code ranges.
• Report all visits (both clinic [in-person] and virtual) and patients where the provider-assigned diagnostic code
is included in the range/group of ICD-10-CM and value set codes shown in the given line.
• Report only diagnoses that were determined as part of documented, countable visits with licensed or
credentialed medical, dental, mental health, substance use disorder, or vision providers.
• Report all diagnoses rendered at a specific visit. However, DO NOT count “active diagnoses” present at the
time of a visit or laboratory test result, but not addressed during the visit.
• Use age at time of visit for diagnoses with specified age ranges.
• DO NOT report a diagnosis visit by another professional or enabling service provider.
• DO NOT report a diagnosis when it is on the problem list but not diagnosed or treated during the visit.
Selected Diagnoses Visits and Patients, Columns A and B
Column A, Number of Visits by Diagnosis Regardless of Primacy
• Report the total number of visits (clinic [in-person] and virtual) during the calendar year where the indicated
diagnosis, regardless of primacy, is diagnosed or treated and listed in the HIT/EHR or visit/billing record.
• Report on Lines 1 through 20f each included diagnosis made at a visit, regardless of the number of diagnoses
listed for the visit. For example, count a patient visit with a diagnosis of hypertension and a diagnosis of
diabetes once on Line 9 and once on Line 11.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
78 2023 UDS MANUAL | Instructions for Table 6A
Column B, Number of Patients with Diagnosis
• Report each patient who had one or more visits (clinic [in-person] and/or virtual) during the calendar year that
were reported in the corresponding cell in Column A.
• Report a patient only once on any given line, regardless of the number of visits made for that specific
diagnosis or family of diagnoses. For example, if a patient received treatment at a single visit for both anxiety
disorder and obsessive-compulsive disorder, they will be counted once on Line 20b, Anxiety Disorders.
SELECTED TESTS/SCREENINGS, LINES 21–26E
Lines 21 through 26e present the name and applicable ICD-10-CM diagnostic, HCPCS, CPT procedure codes,
and/or value sets for selected tests, screenings, and preventive services. On several lines, CPT codes, HCPCS,
value sets, and ICD-10-CM codes are provided. Use either the CPT codes or HCPCS or the ICD-10-CM codes
or the value sets for any specific visit, NOT all code types.
• Report all tests, screenings, or procedures meeting the selection criteria that are provided to a health center
patient prior to, in preparation for, as a part of, or as follow-up to a countable visit.
• Only report tests or procedures (e.g., mammograms, X-rays, tomography) that are:
o performed by the health center, or
o not performed by the health center, but paid for by the health center, or
o not performed by the health center or paid for by the health center, but whose results are returned to the
health center provider to evaluate and provide to the patient.
• During a visit with the provider, selected screenings or tests may be ordered. Report only completed services
(NOT orders) in this section even if they were done at a later date.
• Use age at time of visit for diagnoses and tests with specified age ranges indicated.
Note: ICD-10-CM codes for some services (such as mammography and Pap tests) are listed to ensure capture of
procedures that are done by the health center but may be coded with a different CPT code for state reimbursement
under Title X or BCCEDP. In some instances, payers (especially governmental payers) and labs ask health centers
to use different codes for services. In these instances, health centers should internally map these codes to the
specified list for reporting purposes.
Note: The ICD-10-CM codes, CPT, and RxNORM codes listed in the FAQ
for Pre-Exposure Prophylaxis (PrEP),
Line 21e, DO NOT alone represent patient health records of PrEP prescribed to patients for the purposes of
preventing HIV. Limit the reporting of Line 21e to patients with an active prescription of PrEP based on a
patient’s risk for HIV exposure AND limited to emtricitabine/tenofovir disoproxil fumarate (FTC/TDF) or
emtricitabine/tenofovir alafenamide (FTC/TAF) or cabotegravir for the purposes of preventing HIV.
Selected Tests/Screenings Visits and Patients, Columns A and B
Column A, Number of Visits
• Report the total number of visits (clinic [in-person] and/or virtual) for which one or more of the listed
diagnostic tests, screenings, and/or preventive services were provided during the year. Services may have
been provided at the time of a visit, before a visit, or after a visit.
• Codes for these services may be diagnostic (ICD-10-CM) codes or procedure (CPT or HCPCS) codes or
value sets.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
79 2023 UDS MANUAL | Instructions for Table 6A
• During a single visit, more than one test, screening, or preventive service may be provided. Report each on
the applicable line. If they are on the same line, report only one visit.
Column B, Number of Patients
• Report patients who had a visit (clinic [in-person] and/or virtual) during the calendar year for which one or
more of the selected diagnostic tests, screenings, and/or preventive services listed on Lines 21–26e were
provided.
• Report patients who received more than one type of service during a single visit on each applicable line. For
example, if a patient had a Pap test and contraceptive management during the same visit, this patient would be
counted on both Lines 23 and 25.
• Report a patient only once per service, regardless of the number of times a patient receives a given service.
For example, an infant who has an immunization at each of several well-child visits in the year has each visit
reported in Column A but is counted only once in Column B.
Note: I
nclude follow-up services related to a countable visit. For example, if a provider asks that a patient return
in 30 days for a flu shot, when that patient presents, the shot is counted because it is legally considered to be a part
of the initial visit. DO NOT report a service for an individual who is not a health center patient who comes in just
for a flu shot during a health center–run flu clinic and without a specific referral from a prior visit.
DENTAL SERVICES, LINES 27–34
Lines 27 through 34 present the name and applicable American Dental Association (ADA) procedure and CPT
codes for selected dental services. These services (with the exception of fluoride treatment, which may also be
provided by medical providers) may be performed only by a dental provider who is reported on Lines 16–17a on
Table 5 or by an in-scope dental contractor paid by the health center. Wherever appropriate, services have been
grouped into code ranges. For these lines, the concept of a “primary” code is neither relevant nor used. All
services are reported.
Dental Services Visits and Patients, Columns A and B
Column A, Number of Visits
• Report the total number of visits (clinic [in-person] and/or virtual) for which one or more of the listed
diagnostic tests, screenings, and/or dental services were provided during the year. Services may be at the time
of a visit, before a visit, or after a visit.
• During one visit, more than one test, screening, or dental service may be provided. Report each procedure,
screening, or test on each separate, applicable line. If they are on the same line, report only one visit. For
example, if a patient had more than one tooth filled during a visit, report only one visit for restorative services
(Line 32), NOT one visit per tooth.
Column B, Number of Patients
• Report patients who had at least one visit with a dental professional during the calendar year for each of the
selected dental services listed.
• Only report services that are provided at or as follow-up to countable visits (e.g., a comprehensive oral exam).
• Report a patient who had two teeth repaired and sealants applied during a single visit once on Line 30 and
once on Line 32.
• DO NOT report services provided by personnel other than licensed dentists, dental hygienists, dental
therapists, or personnel working under their direct supervision, unless the service is fluoride treatment
provided at a medical visit.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
80 2023 UDS MANUAL | Instructions for Table 6A
• DO NOT report fluoride treatments or varnishes that are applied outside of a comprehensive treatment plan,
including when provided as part of a community service at schools, on this table or as a visit on Table 5.
SERVICES PROVIDED BY MULTIPLE ENTITIES
Be particularly careful when multiple entities are involved with a service. Use the following rules and general
examples to guide reporting:
• Report the service if a health center provider orders and performs the service. For example, count a rapid
HbA1c test ordered by a health center provider and performed in the health center lab.
• If the health center provider orders a test (e.g., HIV test) and the sample is collected at the health center and
then sent to a reference lab for processing, report the test regardless of whether the test is paid for by the
patient, the patient’s insurance company,
9
a government entity, or the health center.
• Report a test when the health center provider asks a patient to get that test from a third party and the health
center provider receives and reviews the test results with the patient, regardless of who pays for the service.
For example, report mammograms performed by a third-party provider that a health center contracts with and
for which the health center reviews the result with the patient.
• DO NOT report vaccinations performed by a health department when patients are referred to a city or county
health department and the health center does not pay for the service, including referrals where a third party
(e.g., the patient’s insurance company) will make the payment.
• DO NOT report a test or service that a provider asks the patient to get from a third-party provider (e.g., an
HIV test referred to a Ryan White program) that does not bill the health center, including referrals where a
third party (e.g., the patient’s insurance company) will make the payment if the test or service results are
reviewed and acted on by the third-party provider. For example, DO NOT count mammograms performed by
the county health department for which the county will follow up with the patient directly and the health
center did not pay for the service. (These are generally noted in Column III: Formal Written Referral
Arrangement [Health center DOES NOT pay] of Form 5A: Services Provided
).
FAQ FOR TABLE 6A
1. If a case manager or health educator serves a patient who, for example, has diabetes, we often report
that diagnostic code for the visit. Should we report this on Table 6A?
No. Report on Table 6A only visits with medical, dental, mental health, substance use disorder, and vision
providers who are diagnosing according to their own field.
2. The instructions for this table call for diagnoses and services at visits. If we provide the service but it is
not counted as a visit (such as an immunization given at a health fair), should it be reported on this
table?
Report the visit if a service is provided because of a prescription or plan from an earlier counted visit, such as
if a provider asks a patient to come back in four months for a mammogram.
DO NOT report services given at health fairs to an individual who is not a health center patient, regardless of
who provides the service or the level of documentation that is done, such as an HIV test at a health fair.
9
Billing rules require that the charge for a lab test ordered by a provider be sent directly to a third party (including Medicaid and Medicare) and not to the
provider or the health center.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
81 2023 UDS MANUAL | Instructions for Table 6A
3. Some diagnostic and/or procedure codes in our system are different from the codes listed. What do we
do?
It is possible that information for Table 6A is not available using the codes shown because of idiosyncrasies
in state or clinic billing systems. Generally, these involve situations where (a) the state uses unique billing
codes other than the normal CPT code for state billing purposes (e.g., EPSDT) or (b) internal or state
confidentiality rules mask certain diagnostic data. The following table provides examples of problems and
solutions:
Line
Problem
Potential Solution
1
HIV diagnoses are kept confidential, and
alternative diagnostic codes are used.
Include the alternative codes used at your center on these lines as
well.
23
Pap tests are charged to a state BCCEDP
using a special code.
Add these special codes to the other codes listed.
26
Well-child visits are charged to the state
EPSDT program using a special code
(often starting with W, X, Y, or Z).
Add these special codes to the other codes listed and count all
such visits. DO NOT count EPSDT follow-up visits in this
category.
4. The instructions specifically say that the source of information for Table 6A is “billing systems or
HITs.” There are some services for which we DO NOT bill and/or for which there are no visits in our
system. What do we do?
Although health centers are only required to report data derived from billing systems or HITs, the reported
data may understate services in the circumstances described below. In today’s HITs/EHRs, diagnoses and/or
services should be captured in one of the templates available. To more accurately reflect the level of service,
use other codes in the system to enable the tracking.
DO NOT report referrals for which you DO NOT pay or evaluate results and provide back to the patient (e.g.,
sending patients to the county health department for mammograms).
Line
Problem
Potential Solution
21
HIV test samples are collected by us but
processed and paid for by the state and DO
NOT show on the visit form or in the billing
system.
• Preferred: Use the correct code, but report a zero charge.
• Alternative: Use documented completed lab results returned
to the health center.
Multiple
Tests (HIV tests, Pap tests, etc.) are ordered
and samples collected by us. We send
samples to a reference lab for processing, but
the lab bills Medicaid or Medicare directly.
• Preferred: Use the correct code, but report a zero charge.
• Alternative: Use documented completed lab results returned
to the health center.
22
Mammograms are paid for by us but are
conducted by a contractor and DO NOT
show in the billing system for individual
patients.
• Preferred: Use the correct code, with associated charge.
• Alternative: Use the bills from the independent contractor to
identify the mammograms conducted and the patients who
received them and report these numbers.
23
Pap tests are processed and paid for by the
state and DO NOT show on the visit form or
in the billing system.
• Preferred: Use the correct code, but report a zero charge.
• Alternative: Use documented completed lab results returned
to the health center.
24
Flu shots and other vaccinations are NOT
counted because the vaccines are obtained at
no cost to the health center.
• Preferred: Use the correct code, but report a zero charge.
25
Contraceptive management is funded under
Title X or a state family planning program
and does not have a Z30- diagnosis attached
to it.
• Preferred: Add a “dummy code” you can map to the Z30-
code.
• Alternative: Code with both the Z30- and the state-mandated
code, but suppress printing of the Z30- code. Take care not
to count the same visit twice.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
82 2023 UDS MANUAL | Instructions for Table 6A
5. Are we required to report all diagnoses and services rendered during a visit?
Yes and no. No, because there are many diagnoses that may be used but not collected on Table 6A. Yes,
because documentation and reporting of all diagnoses (not just primary diagnosis) and services rendered
during all UDS-countable visits are required. It is important that you appropriately document the breadth of
comprehensive services delivered during each visit, including behavioral health services provided during a
medical visit (e.g., Screening, Brief Intervention, and Referral to Treatment [SBIRT] and/or treatment and
counseling for mental health and substance use disorders).
6. What happens if the CPT, HCPCS, or ICD-10-CM codes change again?
The codes are reviewed and updated annually by the UDS Support Center personnel. If you think a CPT,
ICD, HCPCS, or ADA code for a measure is not reflected in the list or has changed, contact the UDS Support
Center at 1-866-UDS HELP, or udshelp330@bphcdata.net, or BPHC Contact Form
. Personnel will review
the code(s) with BPHC and incorporate approved changes to codes in the manual for future reporting.
7. Are there ICD-10-CM codes for PrEP management?
It is critical that health centers limit the reporting of Line 21e to patients prescribed PrEP based on a
patient’s risk for HIV exposure AND limited to emtricitabine/tenofovir disoproxil fumarate (FTC/TDF) or
emtricitabine/tenofovir alafenamide (FTC/TAF) or cabotegravir for the purposes of preventing HIV. The
information below should be further limited by this guidance to provide the proper counts.
There are no codes specifically for this. Health centers could use the following codes to help identify patient
visits that may include counseling on or initiation of PrEP or that may be associated with currently prescribed
PrEP, based on risk for HIV exposure. The codes are NOT sufficient alone to define PrEP management.
• Possible ICD-10 codes: Z11.3, Z11.4, Z20.2, Z20.6, Z51.81, Z71.51, Z71.7, Z79.899
• Possible CPT codes: 99401 through 99404
• Possible RxNORM codes: 1721603, 1747692, 276237, 322248, 495430
Please note, this is not an exhaustive list. DO NOT report these ICD, CPT, or RxNORM codes on Table 6A.
They only serve as a recommendation to help health centers identify reportable PrEP management. Health
centers can cross check their counts with the Ending the HIV Epidemic Dashboard
, which provides state- and
territory-level counts of individuals prescribed PrEP.
8. Should suspected, possible, probable, or inconclusive SARS-CoV-2 (novel coronavirus) disease
screening and/or tests be reported as diagnosed?
No. If the provider documents “suspected,” “possible,” “probable,” or “inconclusive” coronavirus (SARS-
CoV-2) disease, DO NOT assign code U07.1 and DO NOT report the patient as having this diagnosis. Only
report confirmed novel coronavirus cases.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
83 2023 UDS MANUAL | Instructions for Table 6A
9. If a patient presents to the health center with pneumonia or other health conditions caused by
coronavirus (SARS-CoV-2) disease, is the other health condition reported on Table 6A?
Assign code U07.1 and the appropriate ICD-10 code associated with the other health condition.
Documentation in the patient’s health record and reporting of all diagnoses (not just primary diagnosis) and
services rendered during the visit are required, if applicable. For example, if a patient has pneumonia
confirmed due to coronavirus (SARS-CoV-2) disease, assign and report codes U07.1 (coronavirus disease) on
Line 4c and J12.89 (other viral pneumonia) on Line 6a.
10. We DO NOT perform some services and tests and refer these out. Can we count these?
Possibly. If you perform the service, or if you DO NOT perform the service or test but paid another provider
to provide the requested service, or if the results are returned to the health center provider to evaluate and
provide results back to the patient, you may report these services. The following examples illustrate these
rules:
• Report a Pap test specimen collected by the health center but read by an outside pathologist who then bills
a third party.
• Report a blood draw performed by the health center and sent to an outside lab who then bills Medicaid
and sends the results back to the health center.
• DO NOT report the referral of a patient to the local hospital or county health department for a
mammogram where the local hospital or county health department providers perform the test and provide
results directly to the patient.
11. Can we count patients on multiple lines if they had more than one type of service at a visit?
If patients receive multiple services at one visit and the services are reflected on this table, you may report the
patient and visit once on each applicable line. The following examples illustrate these rules:
• Report a patient with hypertension who also receives an HIV test on Line 11 (hypertension) and on Line
21 (HIV test).
• If both an HIV test and a Pap test were provided during a visit, then report a visit on both Line 21 (HIV
test) and Line 23 (Pap test).
• If a patient receives multiple immunizations at one visit, report only one visit on Line 24.
• Report a patient who comes in for an annual physical and a flu shot. Report this patient on Line 24a (flu
shot) but not on any diagnostic line (since annual physical is not collected on this table).
12. Can we count patients as having received alcohol- or substance use–related Screening, Brief
Intervention, and Referral to Treatment (SBIRT) when only some components are complete?
In order to count the patient as having received SBIRT (Line 26b), the patient must have received screening
and brief intervention OR screening, brief intervention, and referral to treatment.
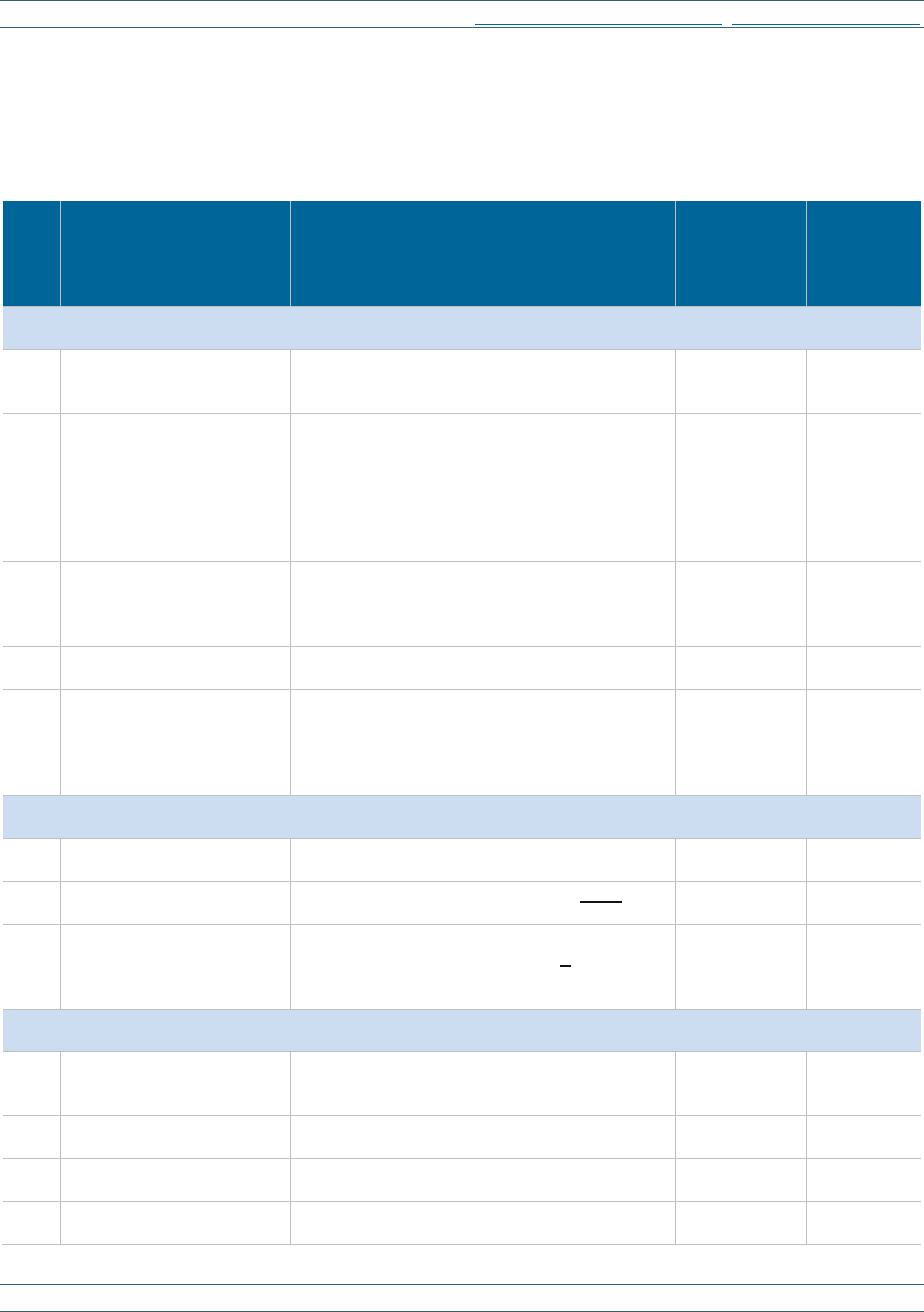
UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
84 2023 UDS MANUAL | Instructions for Table 6A
TABLE 6A: SELECTED DIAGNOSES AND SERVICES RENDERED
Calendar Year: January 1, 2023, through December 31, 2023
SELECTED DIAGNOSES
Line Diagnostic Category
Applicable ICD-10-CM Code or Value Set
Object Identifier (OID)
Number of
Visits by
Diagnosis
Regardless of
Primacy (a)
Number of
Patients
with
Diagnosis
(b)
Selected Infectious and Parasitic Disease
Selected Infectious and
Parasitic Diseases
Selected Infectious and Parasitic Diseases
Selected Infectious and Parasitic
Diseases
Selected Infectious and Parasitic
Diseases
1–2
Symptomatic/Asymptomatic
human immunodeficiency
virus (HIV)
B20, B97.35, O98.7-, Z21
OID: 2.16.840.1.113883.3.464.1003.120.12.1003
<blank for demonstration>
<blank for demonstration>
3
Tuberculosis
A15- through A19-, O98.0-, Z86.15, Z22.7
OID: 2.16.840.1.113762.1.4.1151.56 (O98.0- is
not in value set)
<blank for demonstration>
<blank for demonstration>
4
Sexually transmitted
infections (gonococcal
infections and venereal
diseases)
A50- through A64-, Z22.4
OID: 2.16.840.1.113883.3.464.1003.112.11.1003
<blank for demonstration>
<blank for demonstration>
4a
Hepatitis B
B16.0 through B16.2, B16.9, B17.0, B18.0,
B18.1, B19.1-, O98.4-
OID: 2.16.840.1.113883.3.464.1003.110.12.1025
(B19.1- and O98.4- are not in value set)
<blank for demonstration>
<blank for demonstration>
4b
Hepatitis C
B17.1-, B18.2, B19.2-
OID: 2.16.840.1.113762.1.4.1222.30
<blank for demonstration>
<blank for demonstration>
4c
Novel coronavirus (SARS-
CoV-2) disease
U07.1
OID: 2.16.840.1.113762.1.4.1248.139,
2.16.840.1.113762.1.4.1200.151
<blank for demonstration>
<blank for demonstration>
4d
Post COVID-19 condition
U09.9
OID: 2.16.840.1.113762.1.4.1222.1391
<blank for demonstration>
<blank for demonstration>
Selected Diseases of the Respiratory System
Selected Diseases of the
Respiratory System
Selected Diseases of the Respiratory System
Selected Diseases of the Respiratory
System
Selected Diseases of the
Respiratory System
5
Asthma
J45-
OID: 2.16.840.1.113883.3.526.3.362
<blank for demonstration>
<blank for demonstration>
6
Chronic lower respiratory
diseases
J40 (count J40 only when code U07.1 is not
present), J41- through J44-, J47-
<blank for demonstration>
<blank for demonstration>
6a
Acute respiratory illness due
to novel coronavirus
(SARS-CoV-2) disease
J12.82, J12.89, J20.8, J40, J22, J98.8, J80 (count
codes listed only when code U07.1 is also
present)
OID: 2.16.840.1.113762.1.4.1029.374
<blank for demonstration>
<blank for demonstration>
Selected Other Medical
Conditions
Selected Other Medical
Conditions
Selected Other Medical Conditions
Selected Other Medical Conditions
Selected Other Medical
Conditions
7
Abnormal breast findings,
female
C50.01-, C50.11-, C50.21-, C50.31-, C50.41-,
C50.51-, C50.61-, C50.81-, C50.91-, C79.81,
D05-, D48.6-, D49.3, N60- through N65-, R92-
<blank for demonstration>
<blank for demonstration>
8
Abnormal cervical findings
C53-, C79.82, D06-, N87.0, N87.1, N87.9,
R87.61-, R87.629, R87.810, R87.820
<blank for demonstration>
<blank for demonstration>
9
Diabetes mellitus
E08- through E13-, O24- (exclude O24.41-)
OID: 2.16.840.1.113883.3.464.1003.103.12.1001
<blank for demonstration>
<blank for demonstration>
10
Heart disease (selected)
I01-, I02- (exclude I02.9), I20- through I25-, I27-,
I28-, I30- through I52-
<blank for demonstration>
<blank for demonstration>

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
85 2023 UDS MANUAL | Instructions for Table 6A
Line Diagnostic Category
Applicable ICD-10-CM Code or Value Set
Object Identifier (OID)
Number of
Visits by
Diagnosis
Regardless of
Primacy (a)
Number of
Patients
with
Diagnosis
(b)
11
Hypertension
I10- through I16-, O10-, O11-
<blank for demonstration>
<blank for demonstration>
12
Contact dermatitis and other
eczema
L23- through L25-, L30- (exclude L30.1, L30.3,
L30.4, L30.5), L58-
<blank for demonstration>
<blank for demonstration>
13
Dehydration
E86-
<blank for demonstration>
<blank for demonstration>
14
Exposure to heat or cold
T33-, T34-, T67-, T68-, T69-, W92-, W93-, X30-,
X31-, X32-
<blank for demonstration>
<blank for demonstration>
14a
Overweight and obesity
E66-, Z68- (exclude Z68.1, Z68.20 through
Z68.24, Z68.51, Z68.52)
<blank for demonstration>
<blank for demonstration>
Selected Childhood
Conditions (lim ited to
ages 0 thru 17)
Selected Childhood
Conditions (limited to ages
0 through 17)
Selected Childhood Conditions (limited to ages 0 thru 17)
Selected Childhood Conditions
(limited to ages 0 thru 17)
Selected Childhood Conditions
(limited to ages 0 thru 17)
15
Otitis media and Eustachian
tube disorders
H65- through H69-
<blank for demonstration>
<blank for demonstration>
16
Selected perinatal/neonatal
medical conditions
A33, P19-, P22- through P29- (exclude P29.3-),
P35- through P96- (exclude P54-, P91.6-, P92-,
P96.81)
<blank for demonstration>
<blank for demonstration>
17
Lack of expected normal
physiological development
(such as delayed milestone,
failure to gain weight,
failure to thrive); nutritional
deficiencies in children
only. Does not include
sexual or mental
development.
E40- through E46-, E50- through E63-, P92-,
R62- (exclude R62.7), R63.3- (exclude R63.39)
<blank for demonstration>
<blank for demonstration>
Selected Mental Health and Substance Abuse
Conditions
Selected Mental Health
Conditions, Substance Use
Disorders, and
Exploitations
Selected Mental Health and Substance use Conditions
Selected Mental Health and
Substance use Conditions
Selected Mental Health and
Substance use Conditions
18
Alcohol-related disorders
F10-, G62.1, O99.31-
<blank for demonstration>
<blank for demonstration>
19
Other substance-related
disorders (excluding
tobacco use disorders)
F11- through F19- (exclude F17-), G62.0,
O99.32-
<blank for demonstration>
<blank for demonstration>
19a
Tobacco use disorder
F17-, O99.33-, Z72.0
<blank for demonstration>
<blank for demonstration>
20a
Depression and other mood
disorders
F30- through F39-
<blank for demonstration>
<blank for demonstration>
20b
Anxiety disorders, including
post-traumatic stress
disorder (PTSD)
F06.4, F40- through F42-, F43.0, F43.1-, F43.8-,
F93.0
<blank for demonstration>
<blank for demonstration>
20c
Attention deficit and
disruptive behavior
disorders
F90- through F91-
<blank for demonstration>
<blank for demonstration>
20d
Other mental disorders,
excluding drug or alcohol
dependence
F01- through F09- (exclude F06.4), F20- through
F29-, F43- through F48- (exclude F43.0- and
F43.1-), F50- through F99- (exclude F55-, F64-,
F84.2, F90-, F91-, F93.0, F98-), O99.34-, R45.1,
R45.2, R45.5, R45.6, R45.7, R45.81, R45.82,
R48.0
<blank for demonstration>
<blank for demonstration>

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
86 2023 UDS MANUAL | Instructions for Table 6A
Line Diagnostic Category
Applicable ICD-10-CM Code or Value Set
Object Identifier (OID)
Number of
Visits by
Diagnosis
Regardless of
Primacy (a)
Number of
Patients
with
Diagnosis
(b)
20e
Human trafficking
T74.5- through T74.6-, T76.5- through T76.6-,
Z04.81, Z04.82, Z62.813, Z91.42
<blank for demonstration>
<blank for demonstration>
20f
Intimate partner violence
T74.11, T74.21-, T74.31, Z69.11
<blank for demonstration>
<blank for demonstration>
SELECTED SERVICES RENDERED
Line Service Category
Applicable ICD-10-CM, CPT-
4/I/PLA, or HCPCS Code
Number of
Visits (a)
Number of
Patients (b)
Selected Diagnostic
Tests/Screening /Preventive
Services
Selected Diagnostic Tests/
Screening/Preventive Services
Selected Diagnostic Tests/Screening/Preventive Services
Selected Diagnostic
Tests/Screening/Preventive
Services
Selected Diagnostic
Tests/Screening/Preventive Services
21
HIV test
CPT-4: 86689, 86701 through
86703, 87389 through 87391,
87534 through 87539, 87806
<blank for demonstration>
<blank for demonstration>
21a
Hepatitis B test
CPT-4: 80074, 86704 through
86707, 87340, 87341, 87350,
87467, 87912
<blank for demonstration>
<blank for demonstration>
21b
Hepatitis C test
CPT-4: 80074, 86803, 86804,
87520 through 87522, 87902
<blank for demonstration>
<blank for demonstration>
21c
Novel coronavirus (SARS-CoV-2)
diagnostic test
CPT-4: 87426, 87428, 87635,
87636, 87637
HCPCS: U0001, U0002, U0003,
U0004, U0005
CPT PLA: 0202U, 0223U, 0225U,
0240U, 0241U
<blank for demonstration>
<blank for demonstration>
21d
Novel coronavirus (SARS-CoV-2)
antibody test
CPT-4: 86318, 86328, 86408,
86409, 86413, 86428, 86769,
86811
CPT PLA: 0224U, 0226U
<blank for demonstration>
<blank for demonstration>
21e
Pre-Exposure Prophylaxis (PrEP)-
associated management of all patients
on PrEP
Possible codes to explore for
PrEP management:
CPT-4: 99401 through 99404
ICD-10: Z11.3, Z11.4, Z20.2,
Z20.6, Z51.81, Z71.51, Z71.7,
Z79.899
Limited to prescribed PrEP based
on a patient’s risk for HIV
exposure AND limited to
emtricitabine/tenofovir disoproxil
fumarate (FTC/TDF) or
emtricitabine/tenofovir
alafenamide (FTC/TAF) or
cabotegravir for PrEP
<blank for demonstration>
<blank for demonstration>
22
Mammogram
CPT-4: 77063, 77065, 77066,
77067
ICD-10: Z12.31
HCPCS: G0279
<blank for demonstration>
<blank for demonstration>

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
87 2023 UDS MANUAL | Instructions for Table 6A
Line Service Category
Applicable ICD-10-CM, CPT-
4/I/PLA, or HCPCS Code
Number of
Visits (a)
Number of
Patients (b)
23
Pap test
CPT-4: 88141 through 88153,
88155, 88164 through 88167,
88174, 88175
ICD-10: Z01.41-, Z01.42, Z12.4
(exclude Z01.411 and Z01.419)
HCPCS: G0123, G0143, G0144,
G0145, G0147, G0148
<blank for demonstration>
<blank for demonstration>
24
Selected immunizations: hepatitis A;
haemophilus influenzae B (Hib);
pneumococcal, diphtheria, tetanus,
pertussis (DTaP) (DTP) (DT);
measles, mumps, rubella (MMR);
poliovirus; varicella; hepatitis B
CPT-4: 90632, 90633, 90634,
90636, 90643, 90644, 90645,
90646, 90647, 90648,
90669, 90670, 90696, 90697,
90698, 90700, 90701, 90702,
90703, 90704, 90705, 90706,
90707, 90708, 90710, 90712,
90713, 90714, 90715, 90716,
90718, 90720, 90721, 90723,
90730, 90731, 90732, 90740,
90743, 90744, 90745, 90746,
90747, 90748
<blank for demonstration>
<blank for demonstration>
24a
Seasonal flu vaccine
CPT-4: 90630, 90653 through
90657, 90658, 90661, 90662,
90672, 90673, 90674, 90682,
90685 through 90689, 90694,
90756
<blank for demonstration>
<blank for demonstration>
24b
Coronavirus (SARS-CoV-2) vaccine
CPT-I: 0001A-0004A, 0011A-
0013A, 0021A-0022A, 0031A-
0034A, 0041A-0044A, 0051A-
0054A, 0064A, 0071A-0074A,
0081A-0083A, 0091A-0094A,
0104A, 011A-0113A, 0124A,
0134A, 0144A, 0154A, 0164A,
0173A, 91300-91317
CDT: D1701-D1714
Codes listed include those
available
as of the release date of
this manual.
<blank for demonstration>
<blank for demonstration>
25
Contraceptive management
ICD-10: Z30-
<blank for demonstration>
<blank for demonstration>
26
Health supervision of infant or child
(ages 0 through 11)
CPT-4: 99381 through 99383,
99391 through 99393
ICD-10: Z00.1-, Z76.1. Z76.2
<blank for demonstration>
<blank for demonstration>
26a
Childhood lead test screening (9 to 72
months)
ICD-10: Z13.88
CPT-4: 83655
<blank for demonstration>
<blank for demonstration>
26b
Screening, Brief Intervention, and
Referral to Treatment (SBIRT)
CPT-4: 99408, 99409
HCPCS: G0396, G0397, G0443,
H0050
<blank for demonstration>
<blank for demonstration>
26c
Smoke and tobacco use cessation
counseling
CPT-4: 99406, 99407
HCPCS: S9075
<blank for demonstration>
<blank for demonstration>
26d
Comprehensive and intermediate eye
exams
CPT-4: 92002, 92004, 92012,
92014
<blank for demonstration>
<blank for demonstration>
26e
Childhood development screenings
and evaluations
CPT-4: 96110, 96112, 96113,
96217
ICD-10: Z13.4-

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
88 2023 UDS MANUAL | Instructions for Table 6A
Line Service Category Applicable ADA Code
Number of
Visits (a)
Number of
Patients (b)
Selected Dental
Services
Selected Dental Services
Selected Dental Services
Selected Dental
Services
Selected Dental
Services
27
Emergency services
CDT: D0140, D9110
<blank for demonstration>
<blank for demonstration>
28
Oral exams
CDT: D0120, D0145, D0150,
D0160, D0170, D0171, D0180
<blank for demonstration>
<blank for demonstration>
29
Prophylaxis—adult or child
CDT: D1110, D1120
<blank for demonstration>
<blank for demonstration>
30
Sealants
CDT: D1351
<blank for demonstration>
<blank for demonstration>
31
Fluoride treatment—adult or child
CDT: D1206, D1208
CPT-4: 99188
<blank for demonstration>
<blank for demonstration>
32
Restorative services
CDT: D21xx through D29xx
<blank for demonstration>
<blank for demonstration>
33
Oral surgery (extractions and other
surgical procedures)
CDT: D7xxx
<blank for demonstration>
<blank for demonstration>
34
Rehabilitative services (Endo, Perio,
Prostho, Ortho)
CDT: D3xxx, D4xxx, D5xxx,
D6xxx, D8xxx
<blank for demonstration>
<blank for demonstration>
SOURCES OF CODES
Code System Primary Source Secondary Source
ICD-10-CM
National Center for Health Statistics (NCHS)
ICD10Data.com
CPT
American Medical Association (AMA)
CMS
Code on Dental Procedures and
Nomenclature (CDT)
American Dental Association (ADA)
<blank>
CVX
CDC Vaccine Administered Code Set (CVX)
<blank>
HCPCS
CMS
HCPCSData.com
Value Sets
National Library of Medicine Value Set Authority Center
<blank>
Note: “X” in a code denotes any number, including the absence of a number in that place. Dashes (-) in a code
indicate that additional characters are required. ICD-10-CM codes all have at least four digits. These codes are not
intended to reflect whether or not a code is billable. Instead, they are used to point out that other codes in the
series are to be considered.
Table 6A Cross-Table Considerations:
• The c
ount of patients by diagnosis reported on Table 6A will not be the same count as on Tables 6B and 7,
due to differences in criteria that must be met for inclusion on Tables 6B or 7.
• If you submit Grant Reports, the total number of patients and visits reported on the grant table must be less
than or equal to the corresponding number on the Universal Report for each cell.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
89 2023 UDS MANUAL | Instructions for Tables 6B and 7
Instructions for Tables 6B and 7
Tables 6B and 7 collect data on selected quality-of-care and clinical health outcome and disparity measures.
BPHC first implemented these measures in 2008 and continues to update them. BPHC will continue to revise and
expand these measures consistent with the National Quality Strategy,
CMS electronic clinical quality measures
(eCQMs), and other national quality initiatives.
The clinical quality measures (CQMs) described in this manual must be reported by all health centers using
specifications detailed in the measure definitions described below. The majority of the UDS CQMs are aligned
with CMS 2023 Performance Period Eligible Professional/Eligible Clinician eCQMs
. Use the most current CMS-
issued eCQM specifications for the eCQM number and version referenced in the UDS Manual for 2023 reporting
and measurement period. Although there are other year and version updates available from CMS, they are NOT
to be used for 2023 reporting.
Note: The phrase “measurement period” used in this section is intended to represent calendar year 2023 unless
another timeframe is specifically noted.
For UDS clinical quality measure reporting, include and evaluate patients for the denominator who had at least
one eligible countable visit during the measurement period as specified in the measure.
The measure specifications can be found at the CMS Electronic Clinical Quality Improvement (eCQI) Resource
Center. The eCQM measure numbers and links are provided to assist you, when applicable. Further clarification
or interpretation of CMS eCQMs may be provided by the eCQM Flows and the measure steward (listed in
Appendix H). The Measure Compare tool function available through the eCQM links compares two consecutive
years of eCQM specifications and highlights changes. BPHC defers to the guidance of the measure steward
organization responsible for providing and maintaining the measure requirements and logic statements that
describe the criteria for eCQM reporting. Additionally, the use of official versions of vocabulary value sets as
contained in the
Value Set Authority Center (VSAC)
10
is encouraged for health centers capable of appropriately
using this resource as defined to support the data reporting of these clinical quality measures.
Note: CMS uses logic statements describing the criteria for eCQM reporting using Clinical Quality Language
(CQL) in an effort to standardize reporting workflows. Health centers are advised to review workflows and to
work with HIT/EHR vendors and IT personnel to ensure that required data are being captured correctly to
calculate measures.
COLUMN LOGIC INSTRUCTIONS
Column A (A, 2A, or 3A): Number of Patients in the Denominator
• Report the total number of patients who fulfill the detailed criteria described for the specified measure.
• Report all patients meeting the criteria in the health center’s denominator, including all sites (e.g., urgent care,
prenatal), all in-scope programs (e.g., targeted programs, special populations), and all providers.
• Remove patients who meet exclusion or exception criteria from the denominator.
10
Requires free user account and login.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
90 2023 UDS MANUAL | Instructions for Tables 6B and 7
Because the denominator for each measure is defined in whole or in part in terms of age (or age and sex assigned
at birth), comparisons to the numbers on Tables 3A, 6B, and 7 will be made when evaluating your submission.
The numbers in Column A of Tables 6B and 7 will NOT be equal to those that might be calculated on Table 3A
for the following reasons:
(1) Table 3A measures age as of December 31 of the calendar year. Tables 6B and 7 measure stewards may
define other time periods to measure age, although many measure age as of December 31.
(2) Most of the measures have exclusion and exception criteria that exclude patients from the assessment.
Although comparisons may be made between the numbers on Table 6A and Tables 6B and 7, the numbers in
Column A of Tables 6B and 7 will NOT be equal to those reported in Column B of Table 6A for the following
reasons:
(1) All patients, regardless of age, seen for all reportable services and diagnoses, are included on Table 6A,
but Tables 6B and 7 relate only to patients of specific age ranges.
(2) Table 6A reflects diagnoses and services during the calendar year, but in Tables 6B and 7 measures may
require patients to be considered based on active diagnoses or a look-back period of completed services.
(3) Codes utilized for metrics across the two tables may differ.
Additionally, birth outcomes on Table 7 are compared to prenatal care patients on Table 6B.
Column B (B, 2B, or 3B): Number of Records Reviewed
• Report the total number of health center patients from the denominator (Column A) for whom data have been
reviewed. The number will essentially become the denominator in evaluating the numerator criteria and will
be:
o all patients who fit the criteria (the same number as the denominator reported in Column A), or
o a number equal to or greater than 80%
11
of all patients who meet the criteria (a value no less than 80% of
the denominator reported in Column A). See Appendix C
for more information on reduced denominator
reporting.
Records for new patients should be obtained from their former providers to document prior treatment, including
data for look-back periods. Patient health records, including tests and procedures, obtained from other providers
may be recorded in the health center’s HIT/EHR system consistent with internal patient health records policies, at
which point they may be used in the calculated performance rate for the applicable measure.
The number in Column B (records reviewed) must be no less than 80% of the number in Column A. The reduced
total (in Column B) may not be the result of excluding patients based on a variable related to the measure (e.g., if
patients from a pediatric service delivery site are missing from the HIT/EHR, this method cannot be used for the
Childhood Immunization Status eCQM).
Column C (C or 2C) or 3F: Number of Charts/Records Meeting the Numerator Criteria
• Report the total number of records (included in the count for Column B) that meet the numerator criteria for
the specified clinical quality measure. The number in Column C or F (records in the numerator) can never
exceed the number in Column B (patient health records reviewed).
11
To streamline the process for reporting on the CQMs, and to encourage the use of HIT to report on the full denominator of patients, health centers may use
all of the records available in the HIT/EHR for any given clinical quality measure if at least 80% of all health center patients’ health records are included in
the HIT/EHR and the patients missing from the HIT/EHR are not related to any target group or variable involved with that given measure. For example, if
the patients from a pediatric service delivery site are missing in the HIT/EHR, it cannot be used for the childhood immunization measure.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
91 2023 UDS MANUAL | Instructions for Tables 6B and 7
• Remove patients who meet exception criteria from the numerator and denominator.
Note: The percentage of patient health records meeting the numerator criteria can be calculated by dividing
Column C or 3F by Column B.
Criteria vs. Exceptions and Exclusions in HITs/EHRs vs. Chart Reviews
In the information that follows, “conditions” or “criteria” are at times used interchangeably as “exceptions” or
“exclusions.” This is partly because of the differing language and procedures in an HIT/EHR (or practice
management system)-based report versus a chart audit report. In an HIT/EHR or PMS review, all criteria for a
measure must be locatable in the HIT/EHR and must be in the HIT/EHR for each patient at the health center. If
they cannot be found, findings will be distorted and the HIT/EHR cannot be used. It is important that the
HIT/EHR differentiates between medical and dental patients and is able to limit to either medical or dental
patients as specified in each CQM.
And vs. Or
In this section, conditions linked with “and” mean that each of the conditions must be met. If some but not all
conditions are met, the services for that patient are considered to have failed to meet the numerator criteria.
Conditions linked with “or” mean that criteria must be evaluated in the order prescribed by the measure steward
statements. For example, if the first statement is not met, move to the second, then the third, etc. If none of the
conditions are met, the services for that patient are considered to have failed to meet the numerator criteria.
DETAILED INSTRUCTIONS FOR CLINICAL QUALITY MEASURES
The clinical quality measures (CQMs) reported in the UDS relate to patients who had a countable visit. Report
each measure using the criteria outlined below. Each measure has been organized in the same way to assist with
data collection and reporting.
• Measure Description: The quantifiable indicator to be evaluated.
• Denominator: Patients who fit the detailed criteria described for inclusion in the specific measure to be
evaluated.
• Numerator: Records (from the denominator) that meet the criteria for the specified measure.
• Denominator Exclusions: Patients not to be considered for the measure and who are removed from the
denominator before determining if numerator criteria are met.
• Denominator Exceptions: Patients who meet denominator criteria but do not meet numerator criteria
because they meet any of the exceptions listed for the measure and, therefore, are removed from the
denominator.
• Specification Guidance: CMS measure guidance that assists with understanding and implementing eCQMs.
• UDS Reporting Considerations: Additional BPHC requirements and guidance that must be applied to the
specific measure and that may differ from or expand on the eCQM specifications.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
92 2023 UDS MANUAL | Instructions for Table 6B
Instructions for Table 6B: Quality of Care Measures
The quality-of-care measures reported on Table 6B are “process measures.” This means they document services
that have been shown to be correlated with and serve as a proxy for positive long-term health outcomes.
Individuals who receive routine preventive care and timely chronic care are more likely to have positive
outcomes.
Several notable changes have been made to Table 6B, as outlined below:
• The specifications for the clinical quality measures reported have been revised to align with the CMS eCQMs.
The clinical quality measures are aligned with the most current eCQMs for Eligible Professionals for the 2023
version number referenced in the UDS Manual for the measurement period. (Other updates are available, but
they should not be used for the 2023 reporting.)
• Patients with eligible visits, as defined by the measure steward for the selected measure, are to be considered
for the denominator.
• Age “as of” for several clinical quality measures has been changed and revised to align with CQL criteria.
• In addition to submitting this table as described below within the EHBs, health centers may voluntarily
submit de-identified patient-level report data using Health Level Seven (HL7®) Fast Healthcare
Interoperability Resources (FHIR®) R4 standards for this table.
• Weight Assessment and Counseling for Nutrition and Physical Activity for Children/Adolescents: Final age
to include in assessment has changed from age 16 to 17.
• The Body Mass Index (BMI) Screening and Follow-Up Plan measure numerator changed from a 12-month
requirement to a requirement during the measurement period.
• The Tobacco Screening measure now considers e-cigarette use as tobacco use, hospice care is now a
denominator exclusion, denominator exceptions have all been removed (documented medical reasons for not
screening or providing cessation intervention), and tobacco cessation intervention must now occur during the
measurement period or during the 6 months prior to the measurement period if identified as a tobacco user.
• The Colorectal Cancer Screening measure changed the denominator age from 50–75 to 45–75.
• The Screening for Depression and Follow-Up Plan changed from follow-up, if needed, on the date of the visit
to follow-up up to two days after the date of the visit.
• The Statin Therapy measure changed from current or prior diagnosis of atherosclerotic cardiovascular disease
(ASCVD) to now requiring active diagnosis of ASCVD. Patients who have diagnosis of pregnancy are no
longer excluded from the denominator, and patients with a documented reason for not being prescribed statin
therapy have been added as a denominator exception.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
93 2023 UDS MANUAL | Instructions for Table 6B
TABLE 6B: QUALITY OF CARE MEASURES
This table specifically includes the following CQMs:
Screening and Preventive Care
Maternal Care and
Children’s Health
Disease Management
• Cervical Cancer Screening
• Breast Cancer Screening
• Preventive Care and Screening:
Body Mass Index (BMI) Screening
and Follow-Up Plan
• Preventive Care and Screening:
Tobacco Use: Screening and
Cessation Intervention
• Colorectal Cancer Screening
• HIV Screening
• Preventive Care and Screening:
Screening for Depression and
Follow-Up Plan
• Early Entry into Prenatal Care
• Childhood Immunization Status
• Weight Assessment and Counseling
for Nutrition and Physical Activity
for Children/Adolescents
• Dental Sealants for Children
between 6–9 Years
• Statin Therapy for the Prevention
and Treatment of Cardiovascular
Disease
• Ischemic Vascular Disease (IVD):
Use of Aspirin or Another
Antiplatelet
• HIV Linkage to Care
• Depression Remission at Twelve
Months
SECTIONS A AND B: DEMOGRAPHIC CHARACTERISTICS OF PRENATAL CARE PATIENTS
This section includes information about patients in the prenatal care program.
• Report on all patients who are either provided direct prenatal care or referred for prenatal care.
• Report on the age and trimester of entry into prenatal care for all prenatal care patients, regardless of whether
they receive all or some of their prenatal services in the health center or are referred elsewhere.
• DO NOT include patients who had a positive pregnancy test but did not initiate prenatal care with the health
center or its referral network.
• DO NOT include patients who did not receive prenatal care from a health center provider or who were not
referred by the health center to another provider for prenatal care.
• DO NOT include patients who chose to receive all their prenatal care outside of the health center’s referral
network.
• DO NOT include pregnant patients who received care unrelated to their pregnancy and who are being seen
elsewhere for prenatal care.
Prenatal Care by Referral Only (check box)
All health centers are required to provide prenatal care to patients, either directly or by referral.
• Check the “Prenatal Care by Referral Only” box if you provide prenatal care to patients only through direct
formal written referral to another provider (such as a memorandum of understanding or memorandum of
agreement), as described on Form 5A, Columns II and III
.
• DO NOT check this box if your health center providers provide some or all prenatal care to patients directly.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
94 2023 UDS MANUAL | Instructions for Table 6B
Section A: Age of Prenatal Care Patients (Lines 1–6)
• Report the total number of patients by age group who received prenatal care during the calendar year from the
health center or from a provider in your referral network. Include all patients receiving any prenatal care,
including the delivery of their child, during the calendar year, regardless of when that care was initiated.
• Include patients who:
o receive all their prenatal care from the health center,
o were referred by the health center to another provider for all their prenatal care,
o began prenatal care with another provider but transferred to the health center at some point during their
prenatal care,
o began prenatal care with the health center but were transferred to another provider at some point during
their prenatal care,
o were provided with all their prenatal care by a health center provider but were delivered by another
provider,
o began or were referred for care during the previous calendar year or in this calendar year and delivered
during the calendar year, or
o began or were referred for their care in this calendar year but will not or did not deliver until the next
year.
• To determine the appropriate age group, use the patient’s age on December 31 of the calendar year.
Note: As many as half of all prenatal care patients reported will usually have been reported in the prior year or
will be reported in the next year.
Section B: Early Entry into Prenatal Care (Lines 7–9), No eCQM
Measure Description
Percentage of prenatal care patients who entered prenatal care during their first trimester.
Calculate as follows:
Denominator: Line 7 + Line 8 + Line 9, Columns A + B
• Patients seen for prenatal care during the year
Numerator: Line 7, Columns A + B
• Patients who began prenatal care at the health center or with a referral provider (Column A), or who began
care with another prenatal provider (Column B), during their first trimester
Exclusions/Exceptions
• Denominator Exclusions
o Not applicable
• Denominator Exceptions
o Not applicable

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
95 2023 UDS MANUAL | Instructions for Table 6B
Specification Guidance
• Not applicable
UDS Reporting Considerations
• Report on Lines 7–9 all patients who received prenatal care, either directly or through a referral, including but
not limited to the delivery of a baby during the calendar year.
o First Trimester (Line 7): Report patients who were prenatal care patients during the measurement period
and whose first visit occurred when they were estimated to be pregnant up through the end of the 13th
week after the first day of their last menstrual period.
o Second Trimester (Line 8): Report patients who were prenatal care patients during the measurement
period whose first visit occurred when they were estimated to be between the start of the 14th week and
the end of the 27th week after the first day of their last menstrual period.
o Third Trimester (Line 9): Report patients who were prenatal care patients during the measurement
period and whose first visit occurred when they were estimated to be 28 weeks or more after the first day
of their last menstrual period.
Note: It is unusual for the number in Column B to be very large or larger than that in Column A. This is
especially true for the third trimester, because it would require patients to have begun care very late and then
transfer to the health center in a very short period of time.
The sum of the numbers in the six cells of Lines 7 through 9 represents the total number of patients who received
some or all of their prenatal care from the health center during the calendar year and is equal to the number
reported on Line 6.
• Use the following criteria to identify how prenatal care patients are reported:
o Only report patients who had their first comprehensive prenatal exam with the health center or with the
referral provider as having begun prenatal care. Health center visits that include pregnancy and other lab
tests, dispensing vitamins, taking a health history, and/or obtaining a nutritional or psychosocial
assessment only DO NOT count as the start of prenatal care.
o Determine the trimester by the trimester of pregnancy that the patient was in when they began prenatal
care either at one of the health center’s service delivery locations or with another provider, including a
referral provider.
o Report a patient who begins prenatal care with the health center or is referred by the health center to
another provider only once in Column A (NOT Column B).
o Report a patient who begins prenatal care on their own with another provider and then transfers to the
health center only once in Column B (NOT in Column A).
o Patient self-report of trimester of entry is permitted.
o Report the patient twice as a prenatal care patient in those rare instances when a patient receives prenatal
care services for two separate pregnancies in the same calendar year.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
96 2023 UDS MANUAL | Instructions for Table 6B
SECTIONS C THROUGH M: OTHER QUALITY OF CARE MEASURES
In these sections, report on the findings of reviews of services provided to targeted populations.
• For sections C through M, specifically assess patients seen during the year for an eligible countable visit, as
specified in the measure criteria (e.g., patients who had a medical or mental health visit reported on Table 5 at
least once during the measurement period).
• For these measures, calculate age using the specified dates as required for each eCQM.
• Using the specified criteria, include patients seen for care even if the only care provided was in an urgent care
setting, if patients were seen only once for acute care, if patients were seen only for specialty care, or if the
patient has since left the practice.
• For measures requiring the completion of screenings, tests, or procedures to meet the numerator criteria, the
findings of the screenings, test results, or procedures must be accessible in the patient health record.
Note: I
n this section, the term “measurement period” is the timeframe specified by the measure steward. For
measures not electronically specified, this is intended to capture calendar year 2023 data.
Childhood Immunization Status (Line 10), CMS117v11
Measure Description
Percentage of children 2 years of age who had four diphtheria, tetanus and acellular pertussis (DTaP); three polio
(IPV), one measles, mumps and rubella (MMR); three or four H influenza type B (Hib); three Hepatitis B (Hep
B); one chicken pox (VZV); four pneumococcal conjugate (PCV); one Hepatitis A (Hep A); two or three rotavirus
(RV); and two influenza (flu) vaccines by their second birthday.
Calculate as follows:
Denominator: Columns A and B
• Children who turn 2 years of age during the measurement period and who had an eligible countable visit
during the measurement period, as specified in the measure criteria
o Include patients who were 2 years of age at the end of the measurement period, reflective of children with
birthdate on or after January 1, 2021, and birthdate on or before December 31, 2021.
Numerator: Column C
• Diphtheria, tetanus, and pertussis (DTaP) vaccination
Children with any of the following on or before the child’s second birthday meet criteria:
o At least four DTaP vaccinations, with different dates of service. DO NOT count a vaccination
administered prior to 42 days after birth.
o Anaphylaxis due to the diphtheria, tetanus, or pertussis vaccine.
o Encephalitis due to the diphtheria, tetanus, or pertussis vaccine.
• Poliovirus vaccination (IPV)
o At least three IPV vaccinations, with different dates of service on or before the child’s second birthday.
DO NOT count a vaccination administered prior to 42 days after birth.
• Measles, mumps, and rubella vaccination (MMR)
Children with either of the following meet criteria:

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
97 2023 UDS MANUAL | Instructions for Table 6B
o At least one MMR vaccination on or between the child’s first and second birthdays.
o All of the following anytime on or before the child’s second birthday (on the same or different date of
service): history of measles, mumps, or rubella.
• Haemophilus influenzae type b vaccination (Hib)
Children with either of the following meet criteria on or before the child’s second birthday:
o At least three Hib vaccinations, with different dates of service. DO NOT count a vaccination administered
prior to 42 days after birth.
o Anaphylaxis due to the Hib vaccine.
• Hepatitis B
Children with any of the following on or before the child’s second birthday meet criteria:
o At least three hepatitis B vaccinations, with different dates of service.
o One of the three vaccinations can be a newborn hepatitis B vaccination during the eight-day period that
begins on the date of birth and ends seven days after the date of birth. For example, if the patient’s date of
birth is December 1, the newborn hepatitis B vaccination must be on or between December 1 and
December 8.
o Anaphylaxis due to the hepatitis B vaccine.
o History of hepatitis B illness.
• Varicella vaccination (VZV)
Children with either of the following meet criteria:
o At least one VZV vaccination, with a date of service on or between the child’s first and second birthdays.
o History of varicella zoster (e.g., chicken pox) illness on or before the child’s second birthday.
• Pneumococcal conjugate
o At least four pneumococcal conjugate vaccinations, with different dates of service on or before the child’s
second birthday. DO NOT count a vaccination administered prior to 42 days after birth.
• Hepatitis A
Children with either of the following meet criteria:
o At least one hepatitis A vaccination, with a date of service on or between the child’s first and second
birthdays.
o History of hepatitis A illness on or before the child’s second birthday.
• Rotavirus
Children with any of the following meet criteria:
o At least two doses of the two-dose rotavirus vaccine on different dates of service on or before the child’s
second birthday. DO NOT count a vaccination administered prior to 42 days after birth.
o At least three doses of the three-dose rotavirus vaccine on different dates of service on or before the
child’s second birthday. DO NOT count a vaccination administered prior to 42 days after birth.
o At least one dose of the two-dose rotavirus vaccine and at least two doses of the three-dose rotavirus
vaccine, all on different dates of service, on or before the child’s second birthday. DO NOT count a
vaccination administered prior to 42 days after birth.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
98 2023 UDS MANUAL | Instructions for Table 6B
o Anaphylaxis due to the rotavirus vaccine on or before the child’s second birthday.
• Influenza
o At least two influenza vaccinations, with different dates of service on or before the child’s second
birthday. DO NOT count a vaccination administered prior to 6 months (180 days) after birth.
o One of the two vaccinations can be a live attenuated influenza vaccine (LAIV) vaccination (the nasal
spray flu vaccine) administered on the child’s second birthday. DO NOT count an LAIV vaccination
administered before the child’s second birthday.
Exclusions/Exceptions
• Denominator Exclusions
o Children with any of the following on or before the child’s second birthday:
Severe combined immunodeficiency
Immunodeficiency
HIV
Lymphoreticular cancer, multiple myeloma, or leukemia
Intussusception
o Exclude children who are in hospice care for any part of the measurement period.
• Denominator Exceptions
o Not applicable
Specification Guidance
• The measure allows a grace period by measuring numerator criteria with these recommendations between
birth and age 2.
UDS Reporting Considerations
• Include children who turned 2 years of age during the measurement period, regardless of when they were seen
for care during the year. Specifically, include them in the assessment whether the first visit in the year
occurred before or after they turned 2.
• Include children in the denominator if they came to the health center for well-child
12
services or for any other
medical visits, including treatment of an injury or illness.
• Include children in the denominator for whom no vaccination information is available and/or who were first
seen at a point when there was not enough time to fully immunize them prior to their second birthday.
• Include children who had a contraindication for a specific vaccine in the denominator. Count them as being
“compliant” for that specific vaccine, if the guidance (Specification Guidance) permits it, and then review for
the administration of the rest of the vaccines.
• To meet the numerator criteria, a child’s health record must be documented as being compliant for each
vaccine.
12
Health centers should add to their denominator those patients whose only visits were well-child visits (99381, 99382, 99391, 99392) if their automated
system does not include them. In addition, if your state uses different codes for EPSDT visits, those codes should be added.
UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
99 2023 UDS MANUAL | Instructions for Table 6B
• Registries can be used to fill any voids in the immunization record if the search is routinely done prior to or
immediately after a visit and before the end of the measurement period. For example, you may use an
immunization registry maintained by the state or other public entity that shows comparable information.
• DO NOT include patients here or anywhere on the UDS who only received a vaccination and never received
other services.
• DO NOT count as meeting the numerator criteria charts that only state that the “patient is up to date” with all
immunizations and that DO NOT list the dates of all immunizations and the names of immunization agents.
• DO NOT count toward the numerator criteria verbal assurance from a parent or other individual that a vaccine
has been given.
• Good-faith efforts to get a child immunized that fail DO NOT meet the numerator criteria. These include the
following:
o Parental failure to bring in the patient
o Parents who refuse due to personal beliefs about vaccines or for religious reasons
o Patients lost to follow-up
Cervical Cancer Screening (Line 11), CMS124v11
Measure Description
Percentage of women 21*–64 years of age who were screened for cervical cancer using either of the following
criteria:
• Women age 21*–64 who had cervical cytology performed within the last 3 years
• Women age 30–64 who had human papillomavirus (HPV) testing performed within the last 5 years
*Use 24 as of December 31 as the initial age to include in assessment. See Specification Guidance for further
detail.
Calculate as follows:
Denominator: Columns A and B
• Women 24 through 64 years of age by the end of the measurement period with an eligible countable visit
during the measurement period, as specified in the measure criteria
o Include women with birthdate on or after January 1, 1959, and birthdate on or before December 31, 1999.
Numerator: Column C
• Women with one or more screenings for cervical cancer. Appropriate screenings are defined by any one of the
following criteria:
o Cervical cytology performed during the measurement period or the 2 years prior to the measurement
period for women who are at least 21 years old at the time of the test.
o Cervical HPV testing performed during the measurement period or the 4 years prior to the measurement
period for women who are 30 years or older at the time of the test.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
100 2023 UDS MANUAL | Instructions for Table 6B
Exclusions/Exceptions
• Denominator Exclusions
o Women who had a hysterectomy with no residual cervix or a congenital absence of cervix
o Patients who were in hospice care for any part of the measurement period
o Patients who received palliative care for any part of the measurement period
• Denominator Exceptions
o Not applicable
Specification Guidance
• The measure only evaluates whether tests were performed after a woman turned 21 years of age. The
youngest age in the initial population is a patient who turned 24 years old on December 31.
UDS Reporting Considerations
• Include documentation in the patient health record of a cervical cytology and HPV tests performed outside of
the health center with the date the test was performed, who performed it, and the result of the finding provided
by the agency that conducted the test or a copy of the lab test.
• Include patients of all gender identities who have a cervix.
• DO NOT count as compliant charts that note the refusal of the patient to have the test.
Breast Cancer Screening (Line 11a), CMS125v11
Measure Description
Percentage of women 50*–74 years of age who had a mammogram to screen for breast cancer in the 27 months
prior to the end of the measurement period
*Use 52 on or after December 31 as the initial age to include in assessment. See UDS Reporting Considerations
for further detail.
Calculate as follows:
Denominator: Columns A and B
• Women 52 through 74 years of age by the end of the measurement period with an eligible countable visit
during the measurement period, as specified in the measure criteria
o Include women with birthdate on or after January 1, 1949, and birthdate on or before December 31, 1971.
Numerator: Column C
• Women with one or more mammograms any time on or between October 1 two years prior to the
measurement period and the end of the measurement period
Exclusions/Exceptions
• Denominator Exclusions
o Women who had a bilateral mastectomy or who have a history of a bilateral mastectomy or for whom
there is evidence of a right and a left unilateral mastectomy
UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
101 2023 UDS MANUAL | Instructions for Table 6B
o Patients who were in hospice care for any part of the measurement period
o Patients aged 66 or older by the end of the measurement period who were living long-term in an
institution for more than 90 consecutive days during the measurement period
o Patients aged 66 and older with frailty for any part of the measurement period: advanced illness (with one
inpatient visit or two outpatient visits) or taking dementia medications during the measurement period or
the year prior
o Patients who received palliative care during the measurement period
• Denominator Exceptions
o Not applicable
Specification Guidance
• The measure evaluates primary screening.
• DO NOT count biopsies, breast ultrasounds, or magnetic resonance imaging, because they are not appropriate
methods for primary breast cancer screening.
UDS Reporting Considerations
• The measure only evaluates whether tests were performed after a woman turned 50 years of age. The
youngest age in the initial population is 52.
• If a mammogram was performed outside of the health center, include documentation in the patient health
record with the date the test was performed, who performed it, and the result of the finding provided by the
agency that conducted the diagnostic study or a copy of the results.
• If a system cannot determine exclusions, include them in the denominator and later exclude and replace them
from the assessment, if identified.
• Include patients according to sex at birth.
• DO NOT count as compliant charts that note the refusal of the patient to have the test.
Weight Assessment and Counseling for Nutrition and Physical Activity for
Children/Adolescents (Line 12), CMS155v1
1
Measure Description
Percentage of patients 3–17 years of age who had an outpatient medical visit and who had evidence of height,
weight, and body mass index (BMI) percentile documentation and who had documentation of counseling for
nutrition and who had documentation of counseling for physical activity during the measurement period
Calculate as follows:
Denominator: Columns A and B
• Patients 3 through 17 years of age with at least one outpatient medical visit by the end of the measurement
period, as specified in the measure criteria
UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
102 2023 UDS MANUAL | Instructions for Table 6B
o Include children and adolescents with birthdate on or after January 1, 2006, and birthdate on or before
December 31, 2020.
Numerator: Column C
• Children and adolescents who have had:
o their height, weight, and BMI percentile recorded during the measurement period and
o counseling for nutrition during the measurement period and
o counseling for physical activity during the measurement period
Exclusions/Exceptions
• Denominator Exclusions
o Patients who have a diagnosis of pregnancy during the measurement period
o Patients who were in hospice care for any part of the measurement period
• Denominator Exceptions
o Not applicable
Specification Guidance
• Because BMI norms for youth vary with age and sex, this measure evaluates whether BMI percentile is
assessed rather than an absolute BMI value.
UDS Reporting Considerations
• Include medical visits performed by any medical provider. Note that this is different from the eCQM, which
requires that the visit be performed by a primary care physician or an OB/GYN. For example, include patients
who had a medical visit with an NP.
• The UDS numerator differs from the eCQM in that the eCQM requires the numerator elements to be reported
separately against two age strata (age 3–11, age 12–16). For UDS purposes, the patients must have had all
three numerator components completed in order to meet the numerator criteria using one age strata (age 3–
16).
• DO NOT count as meeting the numerator criteria charts that show only that a well-child visit was scheduled,
provided, or billed. The electronic or paper well-child visit template/form must document each of the
elements noted above.
Preventive Care and Screening: Body Mass Index (BMI) Screening and Follow-Up Plan
(Line 13), CMS69v11
Measure Description
Percentage of patients aged 18 years and older with a BMI documented during the most recent visit or during the
measurement period and who had a follow-up plan documented if BMI was outside of normal parameters
Note: Normal parameters: For age 18 years and older, BMI greater than or equal to 18.5 kg/m
2
and less than 25
kg/m
2

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
103 2023 UDS MANUAL | Instructions for Table 6B
Calculate as follows:
Denominator: Columns A and B
• Patients 18 years of age or older on the date of the visit with at least one eligible countable visit during the
measurement period, as specified in the measure criteria
o Include patients with birthdate on or before January 1, 2005, who were 18 years of age or older on the
date of their last visit.
Note: DO NOT include patients who only had virtual visits during the year in the assessment of this measure
(denominator).
Numerator: Column C
• Patients with a documented BMI during the most recent visit or during the measurement period, and BMI is
within normal parameters, and
• Patients with a documented BMI during the most recent visit or during the measurement period, and when the
BMI is outside of normal parameters, a follow-up plan is documented during the most recent visit or during
the measurement period
Note: Include in the numerator patients within normal parameters who had their BMI documented and those with
a follow-up plan if BMI is outside normal parameters.
Exclusions/Exceptions
• Denominator Exclusions
o Patients who are pregnant at any time during the measurement period
o Patients receiving palliative or hospice care at any time during the measurement period
• Denominator Exceptions
o Patients who refuse measurement of height and/or weight
o Patients with a documented medical reason for not documenting BMI or for not documenting a follow-up
plan for a BMI outside normal parameters (see Specification Guidance)
Specification Guidance
• An eligible professional or their personnel is required to measure both height and weight. Both height and
weight must be measured during the measurement period.
• BMI may be documented in the patient health record at the health center or in outside patient health records
obtained by the health center.
• If the documented BMI is outside of normal parameters, then a follow-up plan is to be documented during the
visit or during the measurement period.
• If more than one BMI is reported during the measurement period, and any of the documented BMI
assessments is outside of normal parameters, documentation of an appropriate follow-up plan is to be used to
determine whether performance has been met.
• Document the follow-up plan based on the documented BMI outside of normal parameters.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
104 2023 UDS MANUAL | Instructions for Table 6B
• Documented medical reasons for denominator exceptions include, but are not limited to:
o Elderly patients (65 years or older) for whom weight reduction or gain would complicate other underlying
health conditions, such as the following examples:
Illness or physical disability
Mental illness, dementia, confusion
Nutritional deficiency, such as vitamin or mineral deficiency
Patients in an urgent or emergent medical situation where time is of the essence and to delay
treatment would jeopardize the patient’s health status
• DO NOT use self-reported height and weight values.
UDS Reporting Considerations
• Documentation in the patient health record must show the actual BMI, or the template normally viewed by a
provider must display BMI.
• A follow-up plan may include, but is not limited to documentation of education, referral (for example, a
registered dietitian nutritionist [RDN], occupational therapist, physical therapist, primary care provider,
exercise physiologist, mental health professional, or surgeon) for lifestyle/behavioral therapy,
pharmacological interventions, dietary supplements, exercise counseling, and/or nutrition counseling.
• Telehealth or telephone-only visits are excluded from the denominator.
• DO NOT count as meeting the numerator criteria charts or templates that display only height and weight. The
fact that an HIT/EHR can calculate BMI does not replace the presence of the BMI itself.
Preventive Care and Screening: Tobacco Use: Screening and Cessation Intervention
(Line 14a), CMS138v11
Measure Description
Percentage of patients aged 18 years and older who were screened for tobacco use one or more times during the
measurement period and who received tobacco cessation intervention during the measurement period or in the 6
months prior to the measurement period if identified as a tobacco user
Calculate as follows:
Denominator: Columns A and B
• Patients aged 18 years and older seen for at least two eligible countable visits in the measurement period or at
least one preventive eligible countable visit during the measurement period, as specified in the measure
criteria
o Include patients with birthdate on or before January 1, 2005.
Numerator: Column C
• Patients who were screened for tobacco use at least once during the measurement period and NOT identified
as a tobacco user, and
• Patients who were screened for tobacco use at least once during the measurement period and received
tobacco cessation intervention during the measurement period or during the 6 months prior to the
measurement period if identified as a tobacco user

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
105 2023 UDS MANUAL | Instructions for Table 6B
Note: Include in the numerator patients with a negative screening and those with a positive screening who had
cessation intervention if a tobacco user.
Exclusions/Exceptions
• Denominator Exclusions
o Patients who were in hospice care for any part of the measurement period
• Denominator Exceptions
o Not applicable
Specification Guidance
• If patients use any type of tobacco (i.e., smokes or uses smokeless tobacco), tobacco cessation intervention
(counseling and/or pharmacotherapy) is expected.
• In order to promote a team-based approach to patient care, the tobacco cessation intervention can be
performed by another health care provider; therefore, the tobacco use screening and tobacco cessation
intervention DO NOT need to be performed by the same provider.
• If a patient has multiple tobacco use screenings during the 12-month period, use the most recent screening
that has a documented status of tobacco user or non-user.
• If tobacco use status of a patient is unknown, the patient does NOT meet the screening component required to
be counted in the numerator and has not met the numerator criteria. “Unknown” includes patients who were
not screened and patients with indefinite answers.
• If a patient has a diagnosis of limited life expectancy, that patient has a valid denominator exception for not
being screened for tobacco use or for not receiving tobacco use cessation intervention (counseling and/or
pharmacotherapy) if identified as a tobacco user.
• The current evidence is insufficient to recommend electronic cigarettes (e-cigarettes) for tobacco cessation.
However, the U.S. Food and Drug Administration definition of tobacco includes e-cigarettes, hookah pens,
and other electronic nicotine delivery systems. Therefore, the measure does consider the use of e-cigarettes
and other electronic nicotine delivery systems to be tobacco use.
UDS Reporting Considerations
• Report in the numerator records that demonstrate that the patient had been asked about their use of all forms
of tobacco during the measurement period.
• If the cessation intervention is pharmacotherapy, then the prescription must be active (one that has not
expired) or ordered during the measurement period.
• Include patients who receive tobacco cessation intervention by any provider, including those who:
o received tobacco use cessation counseling services, or
o received an order for (a prescription or a recommendation to purchase an over-the-counter [OTC]
product) a tobacco use cessation medication, or
o are on (using) a tobacco use cessation agent.
• Identify preventive visits using “Preventive Care Services” CPT codes referenced in the eCQM.
• The UDS denominator differs from the eCQM in that the eCQM requires the patient population and
numerator to be reported separately; for UDS purposes, the patients must be evaluated as one group.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
106 2023 UDS MANUAL | Instructions for Table 6B
• DO NOT count as meeting the numerator criteria providing written self-help materials only.
Statin Therapy for the Prevention and Treatment of Cardiovascular Disease (Line 17a),
CMS347v
6
Measure Description
Percentage of the following patients—all considered at high risk of cardiovascular events—who were prescribed
or were on statin therapy during the measurement period:
• All patients who have an active diagnosis of clinical atherosclerotic cardiovascular disease (ASCVD) or have
ever had an ASCVD procedure, or
• Patients 20 years of age or older who have ever had a low-density lipoprotein cholesterol (LDL-C) laboratory
result level greater than or equal to 190 mg/dL or were previously diagnosed with or currently have an active
diagnosis of familial hypercholesterolemia, or
• Patients 40 through 75 years of age with a diagnosis of diabetes
Calculate as follows:
Denominator: Columns A and B
• All patients who have an active diagnosis of ASCVD or have ever had an ASCVD procedure, or
• Patients who were 20 years of age and older at the start of the measurement period who:
o ever had a laboratory result of LDL-C greater than or equal to 190 mg/dL or
o were previously diagnosed with or currently have an active diagnosis of familial hypercholesterolemia, or
• Patients 40 through 75 years of age at the start of the measurement period with type 1 or type 2 diabetes;
• With an eligible countable visit during the measurement period, as specified in the measure criteria
• Include patients of any age for the ASCVD determination; patients with birthdate on or before January 1,
2003 for LDL-C determination; and patients with birthdate on or after January 1, 1948, and birthdate on or
before January 1, 1983 for diabetes determination.
Numerator: Column C
• Patients who are actively using or who received an order (prescription) for statin therapy at any time during
the measurement period
Exclusions/Exceptions
• Denominator Exclusions
o Patients who are breastfeeding at any time during the measurement period
o Patients who have a diagnosis of rhabdomyolysis at any time during the measurement period
• Denominator Exceptions
o Patients with statin-associated muscle symptoms or an allergy to statin medication
o Patients who are receiving palliative or hospice care
o Patients with active liver disease or hepatic disease or insufficiency
o Patients with end-stage renal disease (ESRD)

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
107 2023 UDS MANUAL | Instructions for Table 6B
o Patients with documentation of a medical reason for not being prescribed statin therapy
Specification Guidance
• Current statin therapy (including statin medication samples provided to patients) must be documented in the
patient’s current medication list or ordered during the measurement period.
• Ensure patients are not counted in the denominator more than once. Once a patient meets one set of
denominator criteria (check from first listed in Measure Description to last), they are included and further risk
checks are not needed.
• Intensity of statin therapy or lifestyle modification coaching is NOT being assessed for this measure; only
prescription or use of any statin therapy is being assessed.
• DO NOT count other cholesterol-lowering medications as meeting the numerator criteria; only statin therapy
meets the numerator criteria.
UDS Reporting Considerations
• Patients who had telephone-only visits are excluded from the denominator.
Ischemic Vascular Disease (IVD): Use of Aspirin or Another Antiplatelet (Line 18),
CMS164v7
Measure Description
Percentage of patients 18 years of age and older who were diagnosed with acute myocardial infarction (AMI), or
who had a coronary artery bypass graft (CABG) or percutaneous coronary interventions (PCIs) in the 12 months
prior to the measurement period or who had an active diagnosis of IVD during the measurement period, and who
had documented use of aspirin or another antiplatelet during the measurement period
Calculate as follows:
Denominator: Columns A and B
• Patients 18 years of age and older with an eligible countable visit during the measurement period who had an
AMI, CABG, or PCI during the 12 months prior to the measurement period or who had a diagnosis of IVD
overlapping the measurement period, as specified in the measure criteria
o Include patients with birthdate on or before January 1, 2005.
Numerator: Column C
• Patients who had an active medication of aspirin or another antiplatelet during the measurement period
Exclusions/Exceptions
• Denominator Exclusions
o Patients who had documentation of use of anticoagulant medications overlapping the measurement period
o Patients who were in hospice care during the measurement period
• Denominator Exceptions
o Not applicable

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
108 2023 UDS MANUAL | Instructions for Table 6B
Specification Guidance
• Not applicable
UDS Reporting Considerations
• Include in the numerator patients who received a prescription for, were given, or were using aspirin or another
antiplatelet drug.
• The electronic specifications for this measure have not been updated. Follow the CMS164v7
specifications
for UDS reporting.
Colorectal Cancer Screening (Line 19), CMS130v11
Measure Description
Percentage of adults 45*–75 years of age who had appropriate screening for colorectal cancer
*Use 46 on or after December 31 as the initial age to include in assessment.
Calculate as follows:
Denominator: Columns A and B
• Patients 46 through 75 years of age by the end of the measurement period with an eligible countable visit
during the measurement period, as specified in the measure criteria
o Include patients with birthdate on or after January 1, 1948, and birthdate on or before December 31, 1977.
Numerator: Column C
• Patients with one or more screenings for colorectal cancer. Appropriate screenings are defined by any one of
the following criteria:
o Fecal occult blood test (FOBT) during the measurement period
o Fecal immunochemical test (FIT)-deoxyribonucleic acid (DNA) during the measurement period or the 2
years prior to the measurement period
o Flexible sigmoidoscopy during the measurement period or the 4 years prior to the measurement period
o Computerized tomography (CT) colonography during the measurement period or the 4 years prior to the
measurement period
o Colonoscopy during the measurement period or the 9 years prior to the measurement period
Exclusions/Exceptions
• Denominator Exclusions
o Patients with a diagnosis or past history of colorectal cancer or total colectomy
o Patients who were receiving palliative or hospice care for any part of the measurement period
o Patients aged 66 or older by the end of the measurement period who were living long-term in an
institution for more than 90 consecutive days during the measurement period
o Patients aged 66 and older by the end of the measurement period with an indication of frailty for any part
of the measurement period who also meet any of the following advanced illness criteria: advanced illness

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
109 2023 UDS MANUAL | Instructions for Table 6B
with one inpatient visit or two outpatient visits during the measurement period or the year prior; or taking
dementia medications during the measurement period or the year prior
• Denominator Exceptions
o Not applicable
Specification Guidance
• DO NOT count digital rectal exam (DRE) or FOBT tests performed in an office setting or performed on a
sample collected via DRE.
UDS Reporting Considerations
• There are two FOBT test options: the guaiac fecal occult blood test (gFOBT) and the immunochemical-based
fecal occult blood test (iFOBT).
• Lab tests (FOBT and FIT-DNA) performed elsewhere must be confirmed by documentation in the chart:
either a copy of the test results or correspondence between the clinic personnel and the performing
lab/provider showing the results.
• FOBTs can be used to document meeting the numerator criteria. This test, if performed, is required each
measurement period. For example, a patient who had an FOBT in November 2022 would still need one in
2023.
• Collect stool specimens for FOBT and FIT-DNA, as recommended by the manufacturer.
• FOBT and FIT-DNA test kits can be mailed to patients, but receipt, processing, and documentation of the test
sample is required.
• DO NOT use self-reported test results.
HIV Linkage to Care (Line 20), No eCQM
Measure Description
Percentage of patients newly diagnosed with HIV who were seen for follow-up treatment within 30 days of
diagnosis
13
Calculate as follows:
Denominator: Columns A and B
• Patients first diagnosed with HIV by the health center between December 1 of the prior year through
November 30 of the current measurement period and who had at least one eligible countable visit during the
measurement period or prior year, as specified in the measure criteria
o Include patients who were diagnosed with HIV for the first time ever
14
by the health center between
December 1, 2022, and November 30, 2023,
15
and had at least one medical visit during 2023 or 2022.
13
Note that this measure does not conform to the calendar year reporting requirement.
14
“Patients first diagnosed with HIV” is defined as patients without a previous HIV diagnosis who received a reactive initial HIV test confirmed by a
positive supplemental antibody immunoassay HIV test.
15
Because the measure allows up to 30 days to complete the follow-up, look back 30 days to find the entire denominator of patients who should have had a
follow-up during the measurement period.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
110 2023 UDS MANUAL | Instructions for Table 6B
Numerator: Column C
• Newly diagnosed HIV patients that received treatment within 30 days of diagnosis. Include patients who were
newly diagnosed by your health center providers and:
o had a medical visit with your health center provider who initiates treatment for HIV, or
o had a visit with a referral resource who initiates treatment for HIV.
Exclusions/Exceptions
• Denominator Exclusions
o Not applicable
• Denominator Exceptions
o Not applicable
Specification Guidance
• Not applicable
UDS Reporting Considerations
• Treatment must be initiated within 30 days of the HIV diagnosis (NOT just a referral made, education
provided, or retest at a referral site).
• Include patients in the numerator only if they received treatment for HIV care within 30 days of the diagnosis.
• If the treatment is by referral to another provider or organization (such as a Ryan White provider), the medical
treatment at the referral source must begin during the 30-day period. Documentation that the visit was
completed (from the provider to whom the patient was referred) is required.
• Identification of patients for this measure crosses years and may include prior-year patients.
• Reactive initial HIV tests and patients who self-identify as being HIV positive without documentation must
be followed by a supplemental test to confirm diagnosis.
• DO NOT include patients who:
o Were diagnosed elsewhere, even if they can provide documentation of the positive test result
o Had a positive reactive initial screening test but not a positive supplemental test
o Were positive on an initial screening test provided by you but were then sent to another provider for
definitive testing and treatment
Note: T
here are no ICD-10-CM or CPT codes to identify newly diagnosed HIV patients. It is strongly encouraged
that you modify your HIT/EHR to record this information or keep track of the patients who are identified in a
separate system.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
111 2023 UDS MANUAL | Instructions for Table 6B
HIV Screening (Line 20a), CMS349v5
Measure Description
Percentage of patients aged 15–65 at the start of the measurement period who were between 15–65 years old
when tested for HIV
This is calculated as follows:
Denominator: Columns A and B
• Patients aged 15 through 65 years of age at the start of the measurement period who had at least one
outpatient eligible countable visit during the measurement period, as specified in the measure criteria
o Include patients with birthdate on or after January 2, 1957, and birthdate on or before January 1, 2008.
Numerator: Column C
• Patients with documentation of an HIV test performed on or after their 15
th
birthday and before their 66
th
birthday
Exclusions/Exceptions
• Denominator Exclusions
o Patients diagnosed with HIV prior to the start of the measurement period
• Denominator Exceptions
o Not applicable
Specification Guidance
• This measure evaluates the proportion of patients aged 15–65 at the start of the measurement period who have
documentation of having received an HIV test at least once on or after their 15
th
birthday and before their 66
th
birthday.
• In order to satisfy the measure, the health center must have documentation of the administration of the
laboratory test present in the patient’s health record.
• HIV tests performed elsewhere must be confirmed by documentation in the chart: either a copy of the test
results or correspondence between the clinic personnel and the performing lab/provider showing the results.
• Patient attestation or self-report to meet the measure requirements is NOT permitted.
UDS Reporting Considerations
• Telephone-only visits are excluded from the denominator.
Preventive Care and Screening: Screening for Depression and Follow-Up Plan (Line
21), CMS2v1
2
Measure Description
Percentage of patients aged 12 years and older screened for depression on the date of the visit or up to 14 days
prior to the date of the visit using an age-appropriate standardized depression screening tool and, if positive, a
follow-up plan is documented on the date of or up to two days after the date of the qualifying visit

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
112 2023 UDS MANUAL | Instructions for Table 6B
This is calculated as follows:
Denominator: Columns A and B
• Patients aged 12 years and older at the beginning of the measurement period with at least one eligible
countable visit during the measurement period, as specified in the measure criteria
o Include patients with birthdate on or before January 1, 2011.
Numerator: Column C
• Patients who were screened for depression on the date of the visit or up to 14 days prior to the date of the visit
using an age-appropriate standardized tool, and screened negative for depression
• Patients who were screened for depression on the date of the visit or up to 14 days prior to the date of the visit
using an age-appropriate standardized tool, and if screened positive for depression, a follow-up plan is
documented on the date of or up to two days after the date of the qualifying visit
Note: Include in the numerator patients with a negative screening and those with a positive screening who had a
follow-up plan documented.
Exclusions/Exceptions
• Denominator Exclusions
o Patients who have been diagnosed with depression or bipolar disorder at any time prior to the qualifying
visit, regardless of whether the diagnosis is active or not
• Denominator Exceptions
o Patients who refuse to participate
o Medical reason(s), including:
Patients who are in urgent or emergent situations
16
where time is of the essence and to delay
treatment would jeopardize the patient’s health status
Patients with documentation of medical reason for not screening the patient for depression (e.g.,
cognitive, functional, or motivational limitations) that may impact the accuracy of results
Specification Guidance
• Patients who have ever been diagnosed with depression or bipolar disorder prior to the eligible visit will be
excluded from the measure.
• The depression screening must be completed on the date of the visit or up to 14 days prior to the date of the
visit using an age-appropriate standardized depression screening tool and must be reviewed and addressed in
the office of the provider on the date of the visit.
• Numerator should be evaluated and reported based on the screening outcome.
• If the screening result is positive, a follow-up plan must be documented on the date of the visit or up to two
days after the visit. A follow-up plan could be additional evaluation, referral, treatment, pharmacological
intervention, or other interventions.
16
Do not exclude patients seen for routine care in urgent care centers or emergency rooms you operate.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
113 2023 UDS MANUAL | Instructions for Table 6B
• Standardized depression screening tools
17
are normalized and validated for the age-appropriate patient
population in which they are used, must be documented in the patient health record, and must be used to meet
the numerator criteria.
o Examples of depression screening tools for adolescents, adults, and perinatal patients are included in the
FAQ for Table 6B.
o Document the screening tool used in the patient health record. Each standardized screening tool provides
guidance on whether a particular score is considered positive for depression.
• Use the most recent screening results.
• The follow-up plan must be related to a positive depression screening.
• Follow-up for a positive depression screening must include one or more of the following:
o Additional interventions designed to treat depression, such as behavioral health evaluation,
psychotherapy, or additional treatment.
o Referral to a provider for further evaluation for depression.
o Pharmacological interventions, when appropriate.
UDS Reporting Considerations
• Although a Patient Health Questionnaire (PHQ-9)
18
may follow a PHQ-2 as a new screening, if the result is
positive, then a compliant follow-up plan on the date of the visit is still required.
• Screening may occur outside of a countable visit.
• Documentation of a follow-up plan “on the date of the visit” can refer to any countable visit, NOT only a
medical visit.
• A suicide risk assessment DOES NOT qualify for the numerator as a follow-up plan.
• DO NOT count patients who are re-screened as meeting the numerator criteria as a follow-up plan to a
positive screen.
• DO NOT count a PHQ-9 screening that follows a positive PHQ-2 screening during the measurement period as
meeting the numerator criteria for a follow-up plan to a positive depression screening.
Depression Remission at Twelve Months (Line 21a), CMS159v11
Measure Description
Percentage of patients aged 12 years and older with major depression or dysthymia who reached remission 12
months (+/- 60 days) after an index event
This is calculated as follows:
Denominator: Columns A and B
• Patients aged 12 years and older with a diagnosis of major depression or dysthymia and an initial PHQ-9 or
PHQ-9 modified for teens (PHQ-9M) score greater than 9 during the index event between November 1, 2021
17
Refer to the publisher and the health center clinical team to interpret the results of screening tools.
18
A PHQ is a screening instrument used by providers to monitor the severity of depression and response to treatment.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
114 2023 UDS MANUAL | Instructions for Table 6B
through October 31, 2022 and at least one eligible countable visit during the measurement period, as
specified in the measure criteria
o Include patients with birthdate on or before November 1, 2009, who were 12 years of age or older on the
date of the index event.
Note: Patients may be screened using PHQ-9 and PHQ-9M on the same date or up to 7 days prior to the visit
(index event).
Numerator: Column C
• Patients who achieved remission at 12 months as demonstrated by the most recent 12-month (+/- 60 days)
PHQ-9 or PHQ-9M score of less than 5
Exclusions/Exceptions
• Denominator Exclusions
o Patients with a diagnosis of bipolar disorder, personality disorder emotionally labile, schizophrenia,
psychotic disorder, or pervasive developmental disorder
o Patients:
Who died
Who received hospice or palliative care services
Who were permanent nursing home residents
• Denominator Exceptions
o Not applicable
Specification Guidance
• Not applicable
UDS Reporting Considerations
• Although PHQ-9 is not the only screening tool approved for the Screening for Depression and Follow-Up
Plan measure, performance for the Depression Remission at Twelve Months must be evaluated using a
PHQ-9 or PHQ-9M screening tool.
• It is possible that the PHQ-9M has been mislabeled as PHQ modified for adolescents (PHQ-A). The PHQ-A
is an 80+ item questionnaire (not a 9-question tool). Use a PHQ-9M version that is approved by the
developers of the PHQ-9 for adolescents.
• The index event is the date the patient had an initial PHQ-9 or PHQ-9M (modified for teens) score greater
than 9 and a diagnosis of major depression or dysthymia during the time period between November 1, 2021,
through October 31, 2022.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
115 2023 UDS MANUAL | Instructions for Table 6B
Dental Sealants for Children between 6–9 Years (Line 22), CMS277v0
19
Measure Description
Percentage of children, age 6–9 years, at moderate to high risk for caries who received a sealant on a first
permanent molar during the measurement period
Note: Although the draft eCQM reflects 5 through 9 years of age, use ages 6 through 9 as the measure steward
intended. This includes patients who were 9 years of age at the beginning of the measurement period.
Calculate as follows:
Denominator: Columns A and B
• Children 6 through 9 years of age with an eligible oral assessment or comprehensive or periodic oral
evaluation countable visit who are at moderate to high risk for caries in the measurement period, as specified
in the measure criteria
o Include children with birthdate on or after January 2, 2013, and birthdate on or before January 1, 2017.
Numerator: Column C
• Children who received a sealant on a permanent first molar tooth during the measurement period
Exclusions/Exceptions
• Denominator Exclusions
o Not applicable
• Denominator Exceptions
o Children for whom all first permanent molars are non-sealable (i.e., molars are either decayed, filled,
currently sealed, or un-erupted/missing)
Specification Guidance
• The intent is to measure whether a child received a sealant on at least one of the four permanent first molars.
• “Elevated risk” must be a finding at the patient level, NOT a population-based factor such as low
socioeconomic status.
• Look for tooth-level data for sealant placement. Capture sealant application within buccal pits on a first
permanent molar in the numerator.
UDS Reporting Considerations
• Include dental sealants placed by the health center or by another dental provider who saw health center dental
patients through a referral, regardless of whether it was paid for by the health center.
• Use ADA codes to document caries risk level determined through an assessment.
• The electronic specifications for this measure have not been updated. Follow the CMS277v0
20
specifications
for UDS reporting.
19
Access measure value set details on the UDS Training and Technical Assistance website.
20
Contact the UDS Support Center to access measure details.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
116 2023 UDS MANUAL | Instructions for Table 6B
FAQ FOR TABLE 6B
1. On which line do we count patients who began prenatal care during the first trimester?
Report the patient on Line 7, and in Column A or B depending on if they began their care with the health
center or with a non–health center provider. For example:
• If the patient began prenatal care during the first trimester at a health center’s service delivery location or
with a provider to which the health center referred the patient, report the patient on Line 7 in Column A.
• If the patient received prenatal care from another provider during the first trimester before coming to the
health center’s service delivery location, report the patient on Line 7 in Column B, regardless of when the
patient begins care with the health center or through direct referral from the health center to another
provider.
2. What timeframe is used to determine each of the trimesters of entry into prenatal care?
The trimesters of entry into prenatal care are as follows:
• First trimester: 0 weeks–13 and 6/7 weeks (months 1–3)
• Second trimester: 14 and 0/7 weeks–27 and 6/7 weeks (months 4–6)
• Third trimester: 28 and 0/7 weeks–40 and 6/7 weeks (months 7–9)
3. A child came in only once during the year for an injury and never returned for well-child care. Do we
have to consider the child’s chart to not have met the numerator criteria since we only treated for the
injury?
Yes. After a patient enters a health center’s system of medical care, the center is expected to provide all
needed preventive health care and/or document that the patient has received it. Report the patient in the
denominator but NOT the numerator, since the record did not meet the numerator criteria.
4. Is the cervical cancer screening review for women starting at age 21 or at age 23?
For this measure, look only at women who were age 23 through age 64 at some point in the measurement
period. Because the measure asks about Pap tests administered in 2023, 2022, or in 2021, it is possible that a
23-year-old woman assessed under this measure would have been 21 in 2021. If the patient received a Pap test
in that year, the patient would be considered to have met the numerator criteria. Although you look only at
women who are 24 through 64 by the end of the measurement period, their qualifying test may have been
done when they were 21 through 64.
5. What if a patient we treat for hypertension and diabetes goes to an OB/GYN in the community for
reproductive health care? Do we still have to consider the patient in the denominator for the cervical
cancer screening measure? What if we DO NOT offer Pap tests?
After the patient has been seen in your clinic, you are responsible for ensuring that they have the appropriate
cervical cancer screening. This can be done by providing the Pap test or documenting the results of a test that
someone else performed. Health centers are encouraged to coordinate care and document Pap test results by
contacting providers. The health center may obtain a copy of the patient’s test result to include in their patient
health record to inform their future care. Consider the patient as part of the denominator for the cervical
cancer screening measure if they received any medical visit(s) in the measurement period. If there is no
evidence of a timely cervical cancer screening included in their patient health record, consider this as NOT
having met the numerator criteria.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
117 2023 UDS MANUAL | Instructions for Table 6B
6. If we inform parents of the importance of immunizations but they refuse to have their child
immunized, may we count the patient health record as having met the numerator criteria if the refusal
is documented?
No. A child is fully immunized only if there is documentation that the child received the vaccine or there is
contraindication for the vaccine, evidence of the antigen, or history of illness. Refusal does NOT meet the
exclusion criteria.
7. Are parents required to bring to the health center documentation of childhood immunizations received
outside the health center?
When possible, health centers are encouraged to access childhood immunizations provided outside the health
center through health information exchange or through read-only EHR access to immunization information
systems, or through other health information exchange-facilitated means. If health information exchange
access to this information is not available, parents are encouraged to provide documentation of immunizations
that their children received elsewhere. Documentation of childhood immunizations may also be obtained by
contacting providers of immunizations directly to obtain documentation by fax or email, by requesting health
center patients mail a copy of their immunization history, through receipt of payment for the vaccine from the
pharmacy, by finding the child in a state or county immunization registry, or through other appropriate means.
8. Some of the immunization details are different from those used by the Centers for Disease Control and
Prevention (CDC) in the Clinic Assessment Software Application (CASA) or Comprehensive-CASA
reviews of our clinic. May we use these CDC standards to report on the UDS?
No. HRSA is now using the CMS eCQM standards to evaluate provision of vaccines to children. Using a
different set of standards will distort the data. A health center may use a different set of standards for its own
internal QI/quality assurance program, but these may not be substituted for the UDS reporting requirements.
9. Does “counseling for nutrition and . . . physical activity” include specific content that must be
provided? Does it need to be provided if the child is within the normal range?
No, the counseling has no specific required content, although it does have specific CPT coding requirements.
It is tailored by the provider given the patient’s BMI percentile and other clinical and social data.
Yes, the counseling must be provided to all children and adolescents. Counseling is aimed at promoting
routine physical activity and healthy eating for all children and adolescents. For younger children, counseling
will be provided to the parent or caregiver.
10. For adult patients, our protocol calls for weight to be measured at every visit but height to be measured
“at least once every 2 years.” Is this acceptable?
BMI is calculated from current height and weight. Both height and weight must be measured during the most
recent visit or during the measurement period, and may be obtained from separate visits.
11. The tobacco screening measure says that there must be intervention for tobacco users. What specific
interventions must be used?
A broad range of counseling and pharmacotherapy is available for tobacco use. Which intervention to use is at
the discretion of each provider.
12. Do quit lines meet the numerator criteria for tobacco cessation?
Yes. Tobacco cessation services provided by quit lines do meet the numerator criteria for the tobacco
screening and cessation intervention measure if the intervention is documented in the patient’s health record.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
118 2023 UDS MANUAL | Instructions for Table 6B
13. How should we collect data for measures that require a look-back period?
Many of the UDS CQMs (e.g., cervical cancer screening, colorectal cancer screening, childhood
immunizations, others) require a look-back period (reference to historical data prior to the measurement
period). It is important that this information is noted in patient health records. It is recommended that you
obtain records for new patients from their former providers to document their prior treatment, including data
for look-back periods. Patient health records obtained from other providers may be recorded in the health
center’s HIT/EHR consistent with internal patient health record policies, at which point they could be used in
the performance review. Additionally, if you change EHRs, ensure that the prior data are transferred to the
new system.
14. Can we use National Quality Forum (NQF) or Healthcare Effectiveness Data and Information Set
(HEDIS) directly to report on the clinical quality measures?
No. For UDS reporting, you must report on the clinical quality measures defined by UDS and outlined in this
manual, most of which align with CMS’s Promoting Interoperability eCQMs.
15. Which patients are we required to report in the denominator for the dental sealants measure?
Health centers providing dental services directly on-site or through paid referral under contract must report on
all dental patients age 6 through 9 at the start of the measurement period who are at elevated risk for caries in
the denominator. Caries risk assessment must be based on patient-level factors and documented with
appropriate ADA codes. This may not be based on population-based factors, such as low socioeconomic
status.
16. Do DNA colorectal cancer screening tests meet the numerator criteria for the colorectal cancer
screening measure?
Yes. FIT-DNA colorectal cancer screening tests (such as Cologuard) meet the numerator criteria for the
colorectal cancer screening measure when performed during the measurement period or in the 2 years prior.
17. If a patient who is newly diagnosed with HIV dies before they receive treatment, do we count them in
the HIV linkage to care measure?
Yes. Include the patient in the denominator, assuming they met the diagnosis criteria. If they died before
receiving the first visit for initiation of treatment, DO NOT count them in the numerator.
18. Can brand-name prescriptions meet the numerator criteria for measures that include a pharmaceutical
component?
Yes. Since only scientific or generic names are stored in the RxNORM value sets, the health center and
vendor need to map the generic and brand names when a new equivalent or brand name is discovered missing
from RxNORM.
19. What does “diagnosis that overlaps the measurement period” mean, as stated for some of the
measures?
The overlap statement means that if patients had the diagnosis at any point during the measurement period,
they are to be included in the denominator and assessed for meeting the numerator criteria.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
119 2023 UDS MANUAL | Instructions for Table 6B
20. If we are able to see that the patient has received a needed service (such as a mammogram or
colonoscopy), such as through our health information exchange or read-only EHR access, can we count
that toward clinical quality measure compliance?
Yes. If a needed service is viewable and accessible in the patient health record directly, or through health
information exchange or read-only EHR access, it may count toward compliance as long as it meets the
specified numerator criteria.
21. What do we need to do in the reporting of specific eCQMs that we have identified to have a
denominator exclusion?
Patients who have been identified to have met a denominator exclusion during the numerator criteria check
need to be removed from the numerator and denominator (and should no longer be considered for the
measure).
22. We would like to recommend changes to specific eCQM requirements being collected in the UDS. Can
HRSA make the changes based on our feedback?
Although HRSA is interested in learning about eCQM changes you would recommend, you should contact
the measure steward through the ONC Issue Tracking System
to submit recommendations to existing eCQM
logic. Appendix H contains the list of measure stewards.
23. What standardized depression screenings comply with the Screening for Depression and Follow-Up
Plan measure?
Use a standardized depression screening tool, which is a normalized and validated tool developed for the
patient population in which it is to be utilized. Examples of depression screening tools include, but are not
limited to those listed in the following chart:
UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
120 2023 UDS MANUAL | Instructions for Table 6B
Adolescent Screening Tools
(12–17 years)
Adult Screening Tools
(18 years and older)
Perinatal Screening Tools
• Patient Health Questionnaire for
Adolescents (PHQ-A)
• Beck Depression Inventory-
Primary Care Version (BDI-PC)
• Mood Feeling Questionnaire
(MFQ)
• Center for Epidemiologic Studies
Depression Scale (CES-D)
• Patient Health Questionnaire
(PHQ-9)
• Pediatric Symptom Checklist (PSC-
17)
• Primary Care Evaluation of Mental
Disorders (PRIME MD)-PHQ-2
• PHQ-9
• Beck Depression Inventory (BDI or
BDI-II)
• CES-D
• Depression Scale (DEPS)
• Duke Anxiety-Depression Scale
(DADS)
• Geriatric Depression Scale (GDS)
• Cornell Scale for Depression in
Dementia (CSDD)
• PRIME MD-PHQ-2
• Hamilton Rating Scale for
Depression (HAM-D)
• Quick Inventory of Depressive
Symptomatology Self-Report
(QID-SR)
• Computerized Adaptive Testing
Depression Inventory (CAT-DI)
• Computerized Adaptive Diagnostic
Screener (CAD-MDD)
• Edinburgh Postnatal Depression
Scale
• Postpartum Depression Screening
Scale
• PHQ-9
• BDI
• BDI-II
• CES-D
• Zung Self-Rating Depression Scale

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
121 2023 UDS MANUAL | Instructions for Table 6B
TABLE 6B: QUALITY OF CARE MEASURES
Calendar Year: January 1, 2023, through December 31, 2023
0
Prenatal Care Provided by Referral Only (Check if Yes)
[blank for demonstration]
Section A—Age Categories for Prenatal Care Patients:
Demographic Characteristics of Prenatal Care Patients
Line
Age
Number of Patients (a)
1
Less than 15 years
[blank for demonstration]
2
Ages 15–19
[blank for demonstration]
3
Ages 20–24
[blank for demonstration]
4
Ages 25–44
[blank for demonstration]
5
Ages 45 and over
[blank for demonstration]
6
Total Patients (Sum of Lines 1–5)
[blank for demonstration]
Section B—Early Entry into Prenatal Care
Line Early Entry into Prenatal Care
Patients Having First Visit with
Health Center (a)
Patients Having First Visit with
Another Provider (b)
7
First Trimester
[blank for demonstration]
[blank for demonstration]
8
Second Trimester
[blank for demonstration]
[blank for demonstration]
9
Third Trimester
[blank for demonstration]
[blank for demonstration]
Section C—Childhood Immunization Status
Line Childhood Immunization Status
Total Patients with
2nd Birthday (a)
Number of
Records Reviewed
(b)
Number of Patients
Immunized (c)
10
MEASURE: Percentage of children 2
years of age who received age-
appropriate vaccines by their 2nd
birthday
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
Section D—Cervical and Breast Cancer Screening
Line Cervical Cancer Screening
Total Female Patients
Aged 24 through 64 (a)
Number of
Records Reviewed
(b)
Number of Patients
Tested (c)
11
MEASURE: Percentage of women
24–64 years of age who were
screened for cervical cancer
[blank for demonstration]
[blank for
demonstration]
[blank for demonstration]
Line Breast Cancer Screening
Total Female Patients
Aged 52 through 74 (a)
Number of
Records Reviewed
(b)
Number of Patients
with Mammogram (c)
11a
MEASURE: Percentage of women
52–74 years of age who had a
mammogram to screen for breast
cancer
[blank for demonstration]
[blank for
demonstration]
[blank for demonstration]

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
122 2023 UDS MANUAL | Instructions for Table 6B
Section E—Weight Assessment and Counseling for Nutrition and Physical Activity of Children/Adolescents
Line
Weight Assessment and Counseling
for Nutrition and Physical Activity
for Children/Adolescents
Total Patients Aged 3
through 17 (a)
Number of
Records Reviewed
(b)
Number of Patients
with Counseling and
BMI Documented (c)
12
MEASURE: Percentage of patients
3–17 years of age with a BMI
percentile and counseling on nutrition
and physical activity documented
[blank for demonstration]
[blank for
demonstration]
[blank for demonstration]
Section F—Preventive Care and Screening: Body Mass Index (BMI) Screening and Follow-Up Plan
Line
Preventive Care and Screening:
Body Mass Index (BMI) Screening
and Follow-Up Plan
Total Patients Aged 18
and Older (a)
Number of
Records Reviewed
(b)
Number of Patients
with BMI Charted
and Follow-Up Plan
Documented as
Appropriate (c)
13
MEASURE: Percentage of patients
18 years of age and older with (1)
BMI documented and (2) follow-up
plan documented if BMI is outside
normal parameters
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
Section G—Preventive Care and Screening: Tobacco Use: Screening and Cessation Intervention
Line
Preventive Care and Screening:
Tobacco Use: Screening and
Cessation Intervention
Total Patients Aged 18
and Older (a)
Number of
Records Reviewed
(b)
Number of Patients
Assessed for Tobacco
Use and Provided
Intervention if a
Tobacco User (c)
14a
MEASURE: Percentage of patients
aged 18 years of age and older who
(1) were screened for tobacco use one
or more times during the
measurement period, and (2) if
identified to be a tobacco user
received cessation counseling
intervention
[blank for demonstration]
[blank for
demonstration]
[blank for demonstration]
Section H—Statin Therapy for the Prevention and Treatment of Cardiovascular Disease
Line
Statin Therapy for the Prevention
and Treatment of Cardiovascular
Disease
Total Patients at High
Risk of Cardiovascular
Events (a)
Number of
Records Reviewed
(b)
Number of Patients
Prescribed or On
Statin Therapy (c)
17a
MEASURE: Percentage of patients at
high risk of cardiovascular events
who were prescribed or were on statin
therapy
[blank for demonstration]
[blank for
demonstration]
[blank for demonstration]

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
123 2023 UDS MANUAL | Instructions for Table 6B
Section I—Ischemic Vascular Disease (IVD): Use of Aspirin or Another Antiplatelet
Line
Ischemic Vascular Disease (IVD):
Use of Aspirin or Another
Antiplatelet
Total Patients Aged 18
and Older with IVD
Diagnosis or AMI,
CABG, or PCI
Procedure (a)
Number of
Records Reviewed
(b)
Number of Patients
with Documentation
of Aspirin or Other
Antiplatelet Therapy
(c)
18
MEASURE: Percentage of patients
18 years of age and older with a
diagnosis of IVD or AMI, CABG, or
PCI procedure with aspirin or another
antiplatelet
[blank for demonstration]
[blank for
demonstration]
[blank for demonstration]
Section J—Colorectal Cancer Screening
Line Colorectal Cancer Screening
Total Patients Aged 46
through 75 (a)
Number of
Records Reviewed
(b)
Number of Patients
with Appropriate
Screening for
Colorectal Cancer (c)
19
MEASURE: Percentage of patients
46 through 75 years of age who had
appropriate screening for colorectal
cancer
[blank for
demonstration]
[blank for
demonstration]
[blank for
demonstration]
Section K—HIV Measures
Line HIV Linkage to Care
Total Patients First
Diagnosed with HIV
(a)
Number of
Records Reviewed
(b)
Number of Patients
Seen Within 30 Days
of First Diagnosis of
HIV (c)
20
MEASURE: Percentage of patients
whose first-ever HIV diagnosis was
made by health center personnel
between December 1 of the prior year
and November 30 of the measurement
period and who were seen for follow-
up treatment within 30 days of that
first-ever diagnosis
[blank for demonstration]
[blank for
demonstration]
[blank for demonstration]
Line HIV Screening
Total Patients Aged 15
through 65 (a)
Number of
Records Reviewed
(b)
Number of Patients
Tested for HIV (c)
20a
MEASURE: Percentage of patients
15 through 65 years of age who were
tested for HIV when within age range
[blank for demonstration]
[blank for
demonstration]
[blank for demonstration]

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
124 2023 UDS MANUAL | Instructions for Table 6B
Section L—Depression Measures
Line
Preventive Care and Screening:
Screening for Depression and
Follow-Up Plan
Total Patients Aged 12
and Older (a)
Number of
Records Reviewed
(b)
Number of Patients
Screened for
Depression and
Follow-Up Plan
Documented as
Appropriate (c)
21
MEASURE: Percentage of patients
12 years of age and older who were
(1) screened for depression with a
standardized tool and, if screening
was positive, (2) had a follow-up plan
documented
[blank for
demonstration]
[blank for
demonstration]
[blank for
demonstration]
Line
Depression Remission at Twelve
Months
Total Patients Aged 12
and Older with Major
Depression or
Dysthymia (a)
Number of
Records Reviewed
(b)
Number of Patients
who Reached
Remission (c)
21a
MEASURE: Percentage of patients
12 years of age and older with major
depression or dysthymia who reached
remission 12 months (+/- 60 days)
after an index event
[blank for
demonstration]
[blank for
demonstration]
[blank for
demonstration]
Section M—Dental Sealants for Children between 6–9 Years
Line
Dental Sealants for Children
between 6–9 Years
Total Patients Aged 6
through 9 at Moderate
to High Risk for
Caries (a)
Number of
Records Reviewed
(b)
Number of Patients
with Sealants to First
Molars (c)
22
MEASURE: Percentage of children 6
through 9 years of age at moderate to
high risk of caries who received a
sealant on a first permanent molar
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
Table 6B Cross-Table Considerations:
• Patients with countable visits on Table 5 are generally eligible for inclusion in eCQMs reported on Table 6B.
• The relationship between the denominators on Table 6B should be verified as reasonable when compared to
the total number of patients by age on Table 3A and the percentage of patients by service category on Table 5.
• The count of patients by diagnosis reported on Table 6A will NOT be the same count as on Table 6B, due to
differences in criteria that must be met for inclusion on Table 6B.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
125 2023 UDS MANUAL | Instructions for Table 7
Instructions for Table 7: Health Outcomes and Disparities
The health outcome and disparity measures reported on Table 7 are “clinical process and outcome measures,”
which means they document measurable outcomes of clinical intervention as a surrogate for good long-term
health outcomes. Increasing the proportion of health center patients who have a good intermediate health outcome
generally leads to improved health status of the patient population in the future.
Several notable changes have been made to Table 7, as outlined below:
• The specifications for the clinical quality measures reported have been revised to align with the CMS eCQMs.
The clinical quality care measures are aligned with the most current eCQMs for Eligible Professionals for the
2023 version number referenced in the UDS Manual for the measurement period. (Other updates are
available, but they should not be used for the 2023 reporting.)
• Patients with eligible visits, as defined by the measure steward for the selected measure, are to be considered
for the denominator.
• Age “as of” for several clinical quality measures have changed and revised to align with CQL criteria.
• In addition to submitting this table as described below within the EHBs, health centers may voluntarily
submit de-identified patient-level report data using Health Level Seven (HL7®) Fast Healthcare
Interoperability Resources (FHIR®) R4 standards for this table.
• Patients 81 years of age and older by the end of the measurement period with an indication of frailty for any
part of the measurement period has been added as a denominator exclusion for the Hypertension measure.
• The Diabetes measure no longer indicates in the Specification Guidance that patients with a diagnosis of
secondary diabetes due to another condition (such as gestational diabetes) are to be excluded from the
denominator.
• This table has been updated to include sub-categories for Asian and Other Pacific Islander, as well as broader
selection for ethnicity by including additional Hispanic, Latino/a, or Spanish origin sub-categories.
TABLE 7: HEALTH OUTCOMES AND DISPARITIES MEASURES
This table specifically includes the following CQMs:
Maternal Care and
Children’s Health
Disease Management
• Low Birth Weight
• Controlling High Blood Pressure
• Diabetes: Hemoglobin A1c (HbA1c) Poor Control
(>9.0%)
RACE AND ETHNICITY REPORTING
Table 7 reports health outcome data by race and Hispanic, Latino/a, or Spanish ethnicity to provide information
on health centers’ efforts to reduce health disparities.
• Race and Hispanic, Latino/a, or Spanish ethnicity are self-reported by patients and should be collected as part
of a standard registration process.
• Care must be taken by health centers that have separate reporting systems for patient registration and clinical
data to ensure race and ethnicity data across the systems are aligned.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
126 2023 UDS MANUAL | Instructions for Table 7
• Because the initial patient population for each measure is defined in terms of race and ethnicity, comparisons
between the numbers on Tables 3B and 7 will be made when evaluating your submission. See the crosswalk
of comparable fields in Appendix B
.
Note: The reporting of patients’ race and ethnicity on the UDS uses HHS data standards, which are a
disaggregation of OMB standards and may differ from the race and ethnicity levels required for other eCQM
reporting programs.
Note: The “Subtotal Hispanic, Latino/a, or Spanish Origin” and “Subtotal Not Hispanic, Latino/a, or Spanish
Origin” lines are grayed out on all three sections of Table 7. They are provided as a system-generated
subtotal.
SECTION A: DELIVERIES AND BIRTH WEIGHT
HIV-P
OSITIVE PREGNANT PATIENTS, TOP LINE (LINE 0)
• Report the total number of HIV-positive pregnant patients served by the health center during the calendar year
on Line 0, regardless of whether the health center provides prenatal care or HIV treatment for these patients.
DELIVERIES PERFORMED BY HEALTH CENTER PROVIDER (LINE 2)
• Report the total number of deliveries performed by health center providers.
• On this line ONLY, include deliveries, regardless of outcome, of any patient, regardless of whether or not
they were part of the health center’s prenatal care program during the calendar year. Include such
circumstances as:
o the delivery of another doctor’s patients when the health center provider participates in a call group and is
on call at the time of delivery,
o emergency deliveries when the health center provider is on call for the emergency room, and
o deliveries of non–health center patients performed by a health center provider as a requirement for
privileging at a hospital.
• DO NOT include deliveries for which a clinic provider separately bills, receives, and retains payment for the
delivery, such as in a moonlighting situation.
DELIVERIES AND BIRTH WEIGHT DATA BY RACE AND HISPANIC, LATINO/A, OR SPANISH
ETHNICITY, COLUMNS 1A–1D
• Report on all prenatal care patients who delivered who are either provided direct care or referred for care.
These patients must also be included in the prenatal care counts on Table 6B.
• Report all health center patients who delivered during the calendar year and all babies born to them in
Columns 1a–1d. Include any patient of the health center who is referred to another provider for some or all of
their prenatal care.
• Report patients delivering (Column 1a) and babies (Columns 1b, 1c, and 1d) separately by their race and
ethnicity. Obtain race and ethnicity of mothers from the information on their patient registration forms.
Obtain race and ethnicity of babies from their registration forms, their birth certificates, or from their parent.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
127 2023 UDS MANUAL | Instructions for Table 7
Prenatal Care Patients and Referred Prenatal Care Patients Who Delivered During the
Year (Column 1a)
• Report all health center prenatal care patients who delivered during the calendar year, including those who
health center personnel cared for and delivered and those who had some or all of their care (including
delivery) provided by a referral provider.
• This column collects data on “patients who delivered.” Report one patient as having delivered, even if the
delivery results in multiple births (e.g., twins or triplets), or is a stillbirth.
• Include all patients who had deliveries, regardless of the outcome.
• DO NOT include deliveries when you have no documentation that the delivery occurred (patients lost to
follow-up).
• DO NOT include patients who, based on their due date, should have delivered but for whom you DO NOT
have explicit documentation of the delivery.
• DO NOT include miscarriages as deliveries.
Note: The percentage of prenatal care patients who delivered can be calculated by dividing Table 7, Line i,
Column 1a by Table 6B, Line 6, Column A. Use the cross-table guidance in Appendix B
to assist with this
reporting.
Birth Weight of Infants Born to Prenatal Care Patients Who Delivered During the Year
(Columns 1b–1d)
Low Birth Weight (Columns 1b and 1c), no eCQM
Measure Description
Percentage of babies of health center prenatal care patients born whose birth weight was below normal (less than
2,500 grams)
Note: The reporting of this measure captures all birth weight categories, not only those birth weights that meet the
numerator criteria.
Calculate as follows:
Denominator: Columns 1b + 1c + 1d
• Babies born during the measurement period to prenatal care patients
Numerator: Columns 1b + 1c
• Babies born with a birth weight below normal (under 2,500 grams)
Exclusions/Exceptions
• Denominator Exclusions
o Stillbirths or miscarriages
• Denominator Exceptions
o Not applicable

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
128 2023 UDS MANUAL | Instructions for Table 7
Specification Guidance
• Not applicable
UDS Reporting Considerations
• Repor
t the total number of live births during the calendar year for patients who received prenatal care from
the health center or a referral provider during the calendar year, according to the appropriate birth weight
group (in grams):
o Very Low Birth Weight (Column 1b): Weight at birth was less than 1,500 grams.
o Low Birth Weight (Column 1c): Weight at birth was 1,500 grams through 2,499 grams.
o Normal Birth Weight (Column 1d): Weight at birth was equal to or greater than 2,500 grams.
Note: Be careful not to confuse pounds and ounces for grams when reporting these numbers. Include birth weight
for neonatal demises.
• If the delivery is of multiple babies (e.g., twins or triplets), report the birth weight of each baby separately.
• Report data regardless of whether the health center did the delivery or referred the delivery to another
provider, and regardless of whether the patient transferred to another provider on their own. Follow-up on all
patients is required.
• In rare instances, there may be no birth outcomes recorded although there may be evidence (i.e., records
indicate delivery occurred) that the patient delivered. Report the patient as having delivered (Column 1a) with
no birth outcomes (Columns 1b–1d).
• The number of deliveries reported in Column 1a will normally be different than the total number of babies
reported in Columns 1b–1d because of multiple births and stillbirths.
• Although data are provided for each race and ethnicity category, the measure looks only at the totals.
21
Note: This is a “negative” measure: The higher the proportion of infants born below normal birth weight, the
worse the performance on the measure.
SECTIONS B AND C: OTHER HEALTH OUTCOME AND DISPARITY MEASURES
In these sections, report the findings of reviews of services provided to targeted populations.
• Sections B and C specifically assess patients seen during the year for an eligible countable visit, as specified
in the measure criteria (e.g., patients who had a medical or mental health visit reported on Table 5 at least
once during the calendar year).
• Using the specified criteria, include patients seen for care even if the only care provided was in an urgent care
setting, patients were seen only once for acute care, patients were seen only for specialty care, or patients have
since left the practice.
• For measures requiring the completion of screenings, tests, or procedures to meet the numerator criteria, the
findings of the screenings, test results, or procedures must be accessible in the patient health record. Patient
self-report is NOT accepted.
21
However, during the review of the UDS Report, reviewers may question unusually high or low proportion of low-birth-weight babies for individual race or
ethnicity categories.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
129 2023 UDS MANUAL | Instructions for Table 7
Controlling High Blood Pressure (Columns 2a–2c), CMS165v11
Measure Description
Percentage of patients 18–85 years of age who had a diagnosis of essential hypertension starting before and
continuing into, or starting during the first six months of the measurement period, and whose most recent blood
pressure (BP) was adequately controlled (less than 140/90 mmHg) during the measurement period
Calculate as follows:
Denominator: Columns 2a and 2b
• Patients 18 through 85 years of age by the end of the measurement period who had a diagnosis of essential
hypertension starting before and continuing into, or starting during the first 6 months of the measurement
period, with an eligible countable visit during the measurement period, as specified in the measure criteria
o Include patients with birthdate on or after January 1, 1938, and birthdate on or before December 31, 2005.
Numerator: Column 2c
• Patients whose most recent blood pressure is adequately controlled (systolic blood pressure less than 140
mmHg and diastolic blood pressure less than 90 mmHg) during the measurement period
Exclusions/Exceptions
• Denominator Exclusions
o Patients with evidence of ESRD, dialysis, or renal transplant before or during the measurement period
o Patients with a diagnosis of pregnancy during the measurement period
o Patients who were in hospice care for any part of the measurement period
o Patients aged 66 or older by the end of the measurement period who were living long-term in a nursing
home any time on or before the end of the measurement period
o Patients aged 66–80 by the end of the measurement period with an indication of frailty for any part of the
measurement period who also meet any of the following advanced illness criteria: advanced illness with
one inpatient visit or two outpatient visits or taking dementia medications during the measurement period
or the year prior
o Patients 81 and older by the end of the measurement period with an indication of frailty for any part of the
measurement period
o Patients who received palliative care for any part of the measurement period
• Denominator Exceptions
o Not applicable
Specification Guidance
• Only blood pressure readings performed by a provider or remote monitoring device are acceptable for the
numerator criteria with this measure.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
130 2023 UDS MANUAL | Instructions for Table 7
• Blood pressure readings are acceptable if:
o taken in person by a clinician,
o measured remotely by an electronic monitoring device capable of transmitting the blood pressure data to
the clinician, or
o taken by a remote monitoring device and conveyed by the patient to the clinician.
• It is the clinician’s responsibility and discretion to confirm the remote monitoring device used to obtain the
blood pressure is considered acceptable and reliable and whether the blood pressure reading is considered
accurate before documenting it in the patient’s medical record.
• If there are multiple blood pressure readings on the last day the patient was seen, use the lowest systolic and
the lowest diastolic reading as the most recent blood pressure reading.
• If no blood pressure is recorded during the measurement period, the patient’s blood pressure is assumed “not
controlled.” Report them in Columns 2a and 2b, but NOT in Column 2c. Ranges and thresholds do not meet
criteria for this measure. A distinct numeric result for both the systolic and diastolic BP reading is required for
numerator compliance.
• DO NOT include blood pressure readings taken during an acute inpatient stay or emergency department visit.
UDS Reporting Considerations
• Include patients who have an active diagnosis of essential hypertension even if their medical visits during the
year were unrelated to the diagnosis.
• Include blood pressure readings taken at any visit type at the health center as long as the result is from the
most recent visit.
• Although data are provided for each race and ethnicity category, the measure looks only at the totals.
Diabetes: Hemoglobin A1c (HbA1c) Poor Control (>9.0 percent) (Columns 3a–3f),
CMS122v1
1
Measure Description
Percentage of patients 18–75 years of age with diabetes who had hemoglobin A1c (HbA1c) greater than 9.0
percent during the measurement period
Calculate as follows:
Denominator: Columns 3a and 3b
• Patients 18 through 75 years of age by the end of the measurement period with diabetes with an eligible
countable visit during the measurement period, as specified in the measure criteria
o Include patients with birthdate on or after January 1, 1948, and birthdate on or before December 31, 2005.
Numerator: Column 3f
• Patients whose most recent HbA1c level performed during the measurement period was greater than 9.0%, or
was missing, or was not performed during the measurement period

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
131 2023 UDS MANUAL | Instructions for Table 7
Exclusions/Exceptions
• Denominator Exclusions
o Patients who were in hospice care for any part of the measurement period
o Patients aged 66 or older by the end of the measurement period who were living long-term in a nursing
home any time on or before the end of the measurement period
o Patients aged 66 or older by the end of the measurement period with an indication of frailty for any part of
the measurement period who also meet any of the following advanced illness criteria: advanced illness
with one inpatient visit or two outpatient visits or taking dementia medications during the measurement
period or the year prior
o Patients who received palliative care for any part of the measurement period
• Denominator Exceptions
o Not applicable
Specification Guidance
• If the HbA1c test result is in the patient health record, the test can be used to determine the numerator criteria.
UDS Reporting Considerations
• Report patients who have an active diagnosis of diabetes even if their medical visits during the year were
unrelated to the diagnosis.
• Use codes as outlined in the measure specifications to determine if diagnosis of secondary diabetes due to
another condition is to be included.
• Include patients in the numerator whose most recent HbA1c level is greater than 9.0%, for whom the most
recent HbA1c result is missing, or for whom no HbA1c tests were performed or documented during the
measurement period.
• Even if the treatment of the patient’s diabetes has been referred to a non–health center provider, the health
center is expected to have the current lab test results in its records.
• Although data are provided for each race and ethnicity category, the measure looks only at the totals.
Note: This is a “negative” measure: The lower the number of adult patients with diabetes with poor diabetes
control, the better the performance on the measure.
FAQ FOR TABLE 7
1. When would we use Line h, “Unreported/Chose not to disclose” race and ethnicity?
Use Line h only in those instances where patients DO NOT provide their race and DO NOT state whether
they are of Hispanic, Latino/a, or Spanish origin. Report patients who provide a race but DO NOT
affirmatively answer a question about Hispanic, Latino/a, or Spanish ethnicity as Not Hispanic, Latino/a, or
Spanish origin on the appropriate race line (Lines 2a–2g). Report patients who indicate they are Hispanic,
Latino/a, or Spanish origin but DO NOT provide a race on Line 1g.
2. Data are requested by race and Hispanic, Latino/a, or Spanish ethnicity. How are these to be coded?
Report race and Hispanic, Latino/a, or Spanish ethnicity on this table in the same manner used to report on
Table 3B. Refer to instructions for Table 3B
for further information describing race and ethnicity categories.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
132 2023 UDS MANUAL | Instructions for Table 7
Ensure the same information is recorded in both the patient health record and the registration form to avoid
errors.
3. Are patients with diabetes required to bring to the health center documentation of HbA1c tests
received from outside the health center?
The health center is required to have HbA1c test results in patient health records. If the health center does not
perform the test, contact the provider who performed the tests. The documentation can be brought in by the
patient, but can also be obtained by fax, by requesting that the patient mail a copy of test results, or through
other appropriate means.
4. In Section A, Deliveries and Birth Outcomes, should the race and ethnicity of the baby be the same as
that of the mother?
Not necessarily. Report the race and ethnicity of the mother (Column 1a) separately from that of the baby
(Column 1b, 1c, or 1d). The baby’s race and ethnicity may differ from the mother’s.
5. How do we report miscarriages and pregnancy terminations on this table?
You don’t. Report all pregnant patients in your prenatal care program (direct or by referral) on Table 6B, but
report only those patients who deliver on Table 7. Consider a stillbirth to be a delivery for purposes of
reporting in Column 1a, but DO NOT report the baby by birth weight in Columns 1b, 1c, or 1d.
6. How do we determine “active diagnosis” that is required for some measures?
Patient health records frequently contain a “problem list,” a list of “active diagnoses,” or lists by other names.
Any diagnosis on the list for part or all of the calendar year is considered “active.”
7. Can we use our population health management system to report on the eCQMs?
Possibly. Health centers that have Office of the National Coordinator for Health IT (ONC)-certified I2I-
Track, personal computer dimensional measurement inspection software (PC-DMIS), a patient electronic care
system (PECS), data reporting and analytics solutions (DRVS), population health management systems, or
other supporting systems may use them to report the denominator only if it can be limited to the measurement
period and only if it includes all required data elements (e.g., it includes data for the required time frame for
all patients with hypertension from all service sites).
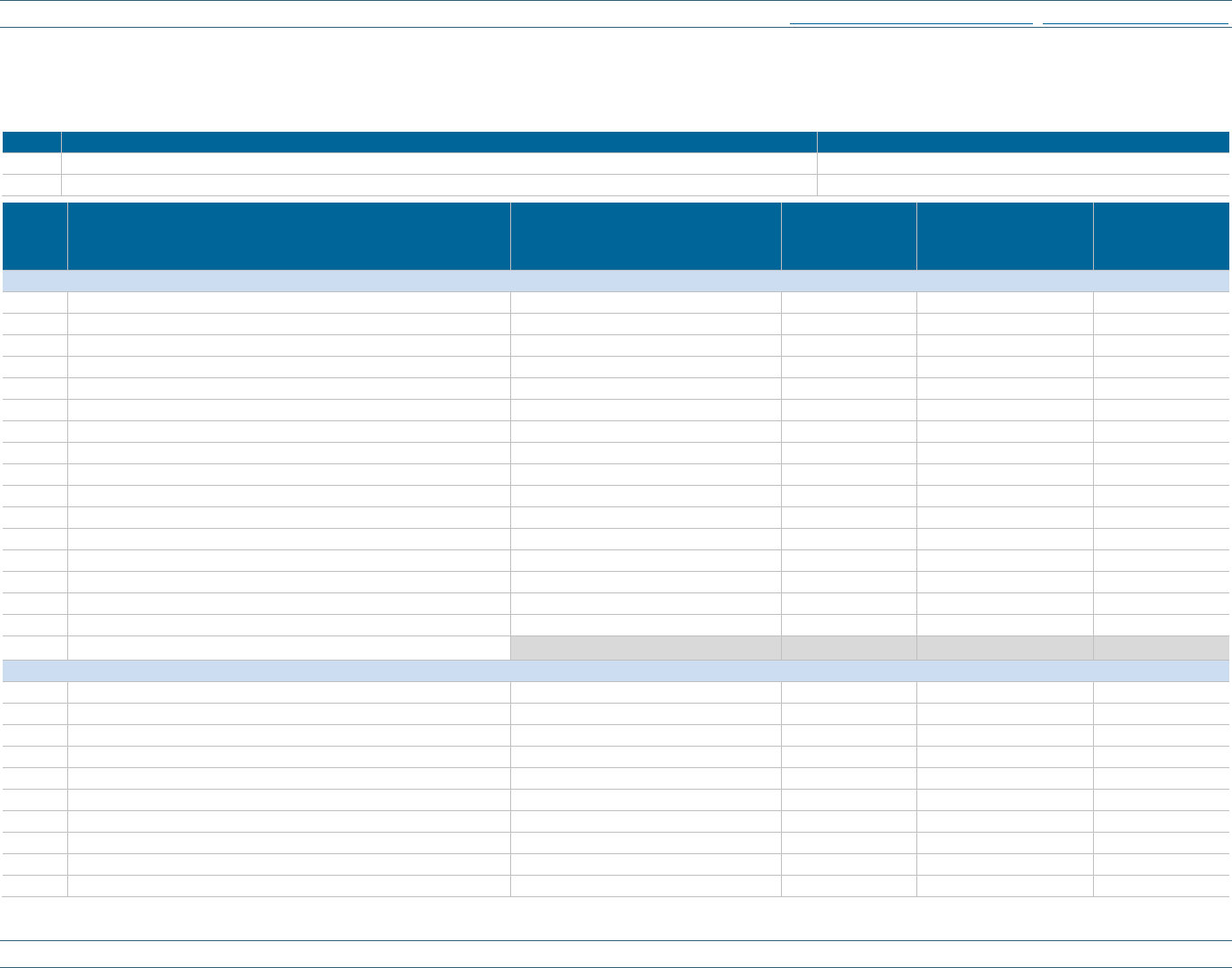
UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
133 2023 UDS MANUAL | Instructions for Table 7
TABLE 7: HEALTH OUTCOMES AND DISPARITIES
Calendar Year: January 1, 2023, through December 31, 2023
Section A: Deliveries and Birth Weight
Line
Description
Patients (a)
0
HIV-Positive Pregnant Patients
<blank for demonstration>
2
Deliveries Performed by Health Center’s Providers
<blank for demonstration>
Line
Race and Ethnicity
Prenatal Care Patients Who
Delivered During the Year
(1a)
Live Births:
<1500 grams
(1b)
Live Births:
1500–2499 grams
(1c)
Live Births:
≥2500 grams
(1d)
<sectio n div ider cell >
Mexican, Mexican American, Chicano/a
<section divider cell>
<section divider cell>
<section divider cell>
<section divider cell>
1a1m
Asian Indian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1a2m
Chinese
1a3m
Filipino
1a4m
Japanese
1a5m
Korean
1a6m
Vietnamese
1a7m
Other Asian
1b1m
Native Hawaiian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b2m
Other Pacific Islander
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b3m
Guamanian or Chamorro
1b4m
Samoan
1cm
Black/African American
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1dm
American Indian/Alaska Native
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1em
White
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1fm
More than One Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1gm
Unreported/Chose Not to Disclose Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
subtotal
Subtotal Mexican, Mexican American, Chicano/a
<cell not reported>
<cell not reported>
<cell not reported>
<cell not reported>
<blank for demonstratio n>
Puerto Rican
<section divider cell>
<section divider cell>
<section divider cell>
<section divider cell>
1a1p
Asian Indian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1a2p
Chinese
1a3p
Filipino
1a4p
Japanese
1a5p
Korean
1a6p
Vietnamese
1a7p
Other Asian
1b1p
Native Hawaiian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b2p
Other Pacific Islander
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b3p
Guamanian or Chamorro

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
134 2023 UDS MANUAL | Instructions for Table 7
Line
Race and Ethnicity
Prenatal Care Patients Who
Delivered During the Year
(1a)
Live Births:
<1500 grams
(1b)
Live Births:
1500–2499 grams
(1c)
Live Births:
≥2500 grams
(1d)
1b4p
Samoan
1cp
Black/African American
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1dp
American Indian/Alaska Native
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1ep
White
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1fp
More than One Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1gp
Unreported/Chose Not to Disclose Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
subtotal
Subtotal Puerto Rican
<cell not reported>
<cell not reported>
<cell not reported>
<cell not reported>
<blank for demonstratio n>
Cuban
<section divider cell>
<section divider cell>
<section divider cell>
<section divider cell>
1a1c
Asian Indian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1a2c
Chinese
1a3c
Filipino
1a4c
Japanese
1a5c
Korean
1a6c
Vietnamese
1a7c
Other Asian
1b1c
Native Hawaiian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b2c
Other Pacific Islander
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b3c
Guamanian or Chamorro
1b4c
Samoan
1cc
Black/African American
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1dc
American Indian/Alaska Native
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1ec
White
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1fc
More than One Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1gc
Unreported/Chose Not to Disclose Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
subtotal
Subtotal Cuban
<cell not reported>
<cell not reported>
<cell not reported>
<cell not reported>
<blank for demonstratio n>
Another Hispanic, Latino/a, or Spanish Origin
<section divider cell>
<section divider cell>
<section divider cell>
<section divider cell>
1a1a
Asian Indian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1a2a
Chinese
1a3a
Filipino
1a4a
Japanese
1a5a
Korean
1a6a
Vietnamese
1a7a
Other Asian
1b1a
Native Hawaiian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b2a
Other Pacific Islander
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
135 2023 UDS MANUAL | Instructions for Table 7
Line
Race and Ethnicity
Prenatal Care Patients Who
Delivered During the Year
(1a)
Live Births:
<1500 grams
(1b)
Live Births:
1500–2499 grams
(1c)
Live Births:
≥2500 grams
(1d)
1b3a
Guamanian or Chamorro
1b4a
Samoan
1ca
Black/African American
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1da
American Indian/Alaska Native
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1ea
White
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1fa
More than One Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1ga
Unreported/Chose Not to Disclose Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
subtotal
Subtotal Another Hispanic, Latino/a, or Spanish Origin
<cell not reported>
<cell not reported>
<cell not reported>
<cell not reported>
<blank for demonstratio n>
Hispanic, Latino/a, or Spanish Origin Combined
<section divider cell>
<section divider cell>
<section divider cell>
<section divider cell>
1a1o
Asian Indian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1a2o
Chinese
1a3o
Filipino
1a4o
Japanese
1a5o
Korean
1a6o
Vietnamese
1a7o
Other Asian
1b1o
Native Hawaiian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b2o
Other Pacific Islander
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b3o
Guamanian or Chamorro
1b4o
Samoan
1co
Black/African American
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1do
American Indian/Alaska Native
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1eo
White
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1fo
More than One Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1go
Unreported/Chose Not to Disclose Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
subtotal
Subtotal Hispanic, Latino/a, or Spanish Origin, Combined
<cell not reported>
<cell not reported>
<cell not reported>
<cell not reported>
Total Hispanic, Latino/a, or Spanish Origin
<cell not reported>
<cell not reported>
<cell not reported>
<cell not reported>
<blank for demonstratio n>
Not Hispanic, Latino/a, or Spanish Origin
<section divider cell>
<section divider cell>
<section divider cell>
<section divider cell>
2a1
Asian Indian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
2a2
Chinese
2a3
Filipino
2a4
Japanese
2a5
Korean
2a6
Vietnamese
2a7
Other Asian

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
136 2023 UDS MANUAL | Instructions for Table 7
Line
Race and Ethnicity
Prenatal Care Patients Who
Delivered During the Year
(1a)
Live Births:
<1500 grams
(1b)
Live Births:
1500–2499 grams
(1c)
Live Births:
≥2500 grams
(1d)
2b1
Native Hawaiian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
2b2
Other Pacific Islander
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
2b3
Guamanian or Chamorro
2b4
Samoan
2c
Black/African American
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
2d
American Indian/Alaska Native
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
2e
White
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
2f
More than One Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
2g
Unreported/Chose Not to Disclose Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
subtotal
Total Not Hispanic, Latino/a, or Spanish Origin
<cell not reported>
<cell not reported>
<cell not reported>
<cell not reported>
<blank for demonstratio n>
Unreported/Chose Not to Disclose Race and Ethnicity
<section divider cell>
<section divider cell>
<section divider cell>
<section divider cell>
h
Unreported/Chose Not to Disclose Race and Ethnicity
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
i
Total
<cell not reported>
<cell not reported>
<cell not reported>
<cell not reported>

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
137 2023 UDS MANUAL | Instructions for Table 7
Section B: Controlling High Blood Pressure
Line Race and Ethnicity
Total Patients 18 through 84 Years of
Age with Hypertension
(2a)
Number of Records Reviewed
(2b)
Patients with Hypertension
Controlled
(2c)
<blank for demonstratio n>
Mexican, Mexican American,
Chicano/a
<section divider cell>
<section divider cell>
<section divider cell>
1a1m
Asian Indian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1a2m
Chinese
1a3m
Filipino
1a4m
Japanese
1a5m
Korean
1a6m
Vietnamese
1a7m
Other Asian
1b1m
Native Hawaiian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b2m
Other Pacific Islander
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b3m
Guamanian or Chamorro
1b4m
Samoan
1cm
Black/African American
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1dm
American Indian/Alaska Native
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1em
White
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1fm
More than One Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1gm
Unreported/Chose Not to Disclose Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
subtotal
Subtotal Mexican, Mexican American,
Chicano/a
<cell not reported>
<cell not reported>
<cell not reported>
<blank for demonstratio n>
Puerto Rican
<section divider cell>
<section divider cell>
<section divider cell>
1a1p
Asian Indian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1a2p
Chinese
1a3p
Filipino
1a4p
Japanese
1a5p
Korean
1a6p
Vietnamese
1a7p
Other Asian
1b1p
Native Hawaiian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b2p
Other Pacific Islander
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b3p
Guamanian or Chamorro
1b4p
Samoan
1cp
Black/African American
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1dp
American Indian/Alaska Native
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
138 2023 UDS MANUAL | Instructions for Table 7
Line Race and Ethnicity
Total Patients 18 through 84 Years of
Age with Hypertension
(2a)
Number of Records Reviewed
(2b)
Patients with Hypertension
Controlled
(2c)
1ep
White
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1fp
More than One Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1gp
Unreported/Chose Not to Disclose Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
subtotal
Subtotal Puerto Rican
<cell not reported>
<cell not reported>
<cell not reported>
<blank for demonstratio n>
Cuban
<section divider cell>
<section divider cell>
<section divider cell>
1a1c
Asian Indian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1a2c
Chinese
1a3c
Filipino
1a4c
Japanese
1a5c
Korean
1a6c
Vietnamese
1a7c
Other Asian
1b1c
Native Hawaiian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b2c
Other Pacific Islander
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b3c
Guamanian or Chamorro
1b4c
Samoan
1cc
Black/African American
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1dc
American Indian/Alaska Native
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1ec
White
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1fc
More than One Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1gc
Unreported/Chose Not to Disclose Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
subtotal
Subtotal Cuban
<cell not reported>
<cell not reported>
<cell not reported>
<blank for demonstratio n>
Another Hispanic, Latino/a, or Spanish
Origin
<section divider cell>
<section divider cell>
<section divider cell>
1a1a
Asian Indian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1a2a
Chinese
1a3a
Filipino
1a4a
Japanese
1a5a
Korean
1a6a
Vietnamese
1a7a
Other Asian
1b1a
Native Hawaiian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b2a
Other Pacific Islander
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b3a
Guamanian or Chamorro
1b4a
Samoan
1ca
Black/African American
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
139 2023 UDS MANUAL | Instructions for Table 7
Line Race and Ethnicity
Total Patients 18 through 84 Years of
Age with Hypertension
(2a)
Number of Records Reviewed
(2b)
Patients with Hypertension
Controlled
(2c)
1da
American Indian/Alaska Native
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1ea
White
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1fa
More than One Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1ga
Unreported/Chose Not to Disclose Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
subtotal
Subtotal Another Hispanic, Latino/a, or
Spanish Origin
<cell not reported>
<cell not reported>
<cell not reported>
<blank for demonstratio n>
Hispanic, Latino/a, or Spanish Origin,
Combined
<section divider cell>
<section divider cell>
<section divider cell>
1a1o
Asian Indian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1a2o
Chinese
1a3o
Filipino
1a4o
Japanese
1a5o
Korean
1a6o
Vietnamese
1a7o
Other Asian
1b1o
Native Hawaiian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b2o
Other Pacific Islander
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b3o
Guamanian or Chamorro
1b4o
Samoan
1co
Black/African American
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1do
American Indian/Alaska Native
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1eo
White
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1fo
More than One Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1go
Unreported/Chose Not to Disclose Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
subtotal
Subtotal Hispanic, Latino/a, or Spanish
Origin, Combined
<cell not reported>
<cell not reported>
<cell not reported>
Total Hispanic, Latino/a, or Spanish
Origin
<cell not reported>
<cell not reported>
<cell not reported>
<blank for demonstratio n>
Not Hispanic, Latino/a, or Spanish
Origin
<section divider cell>
<section divider cell>
<section divider cell>
2a1
Asian Indian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
2a2
Chinese
2a3
Filipino
2a4
Japanese
2a5
Korean
2a6
Vietnamese

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
140 2023 UDS MANUAL | Instructions for Table 7
Line Race and Ethnicity
Total Patients 18 through 84 Years of
Age with Hypertension
(2a)
Number of Records Reviewed
(2b)
Patients with Hypertension
Controlled
(2c)
2a7
Other Asian
2b1
Native Hawaiian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
2b2
Other Pacific Islander
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
2b3
Guamanian or Chamorro
2b4
Samoan
2c
Black/African American
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
2d
American Indian/Alaska Native
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
2e
White
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
2f
More than One Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
2g
Unreported/Chose Not to Disclose Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
subtotal
Total Not Hispanic, Latino/a, or Spanish
Origin
<cell not reported>
<cell not reported>
<cell not reported>
<blank for demonstratio n>
Unreported/Chose Not to Disclose Race
and Ethnicity
<section divider cell>
<section divider cell>
<section divider cell>
h
Unreported/Chose Not to Disclose Race
and Ethnicity
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
i
Total
<cell not reported>
<cell not reported>
<cell not reported>

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
141 2023 UDS MANUAL | Instructions for Table 7
Section C: Diabetes: Hemoglobin A1c Poor Control
Line Race and Ethnicity
Total Patients 18 through 74 Years of
Age with Diabetes
(3a)
Number of Records Reviewed
(3b)
Patients with HbA1c >9.0%
or No Test During Year
(3f)
<blank for demonstratio n>
Mexican, Mexican American,
Chicano/a
<section divider cell>
<section divider cell>
<section divider cell>
1a1m
Asian Indian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1a2m
Chinese
1a3m
Filipino
1a4m
Japanese
1a5m
Korean
1a6m
Vietnamese
1a7m
Other Asian
1b1m
Native Hawaiian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b2m
Other Pacific Islander
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b3m
Guamanian or Chamorro
1b4m
Samoan
1cm
Black/African American
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1dm
American Indian/Alaska Native
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1em
White
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1fm
More than One Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1gm
Unreported/Chose Not to Disclose Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
Subtotal
Subtotal Mexican, Mexican American,
Chicano/a
<cell not reported>
<cell not reported>
<cell not reported>
<blank for demonstratio n>
Puerto Rican
<section divider cell>
<section divider cell>
<section divider cell>
1a1p
Asian Indian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1a2p
Chinese
1a3p
Filipino
1a4p
Japanese
1a5p
Korean
1a6p
Vietnamese
1a7p
Other Asian
1b1p
Native Hawaiian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b2p
Other Pacific Islander
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b3p
Guamanian or Chamorro
1b4p
Samoan
1cp
Black/African American
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1dp
American Indian/Alaska Native
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
142 2023 UDS MANUAL | Instructions for Table 7
Line Race and Ethnicity
Total Patients 18 through 74 Years of
Age with Diabetes
(3a)
Number of Records Reviewed
(3b)
Patients with HbA1c >9.0%
or No Test During Year
(3f)
1ep
White
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1fp
More than One Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1gp
Unreported/Chose Not to Disclose Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
Subtotal
Subtotal Puerto Rican
<cell not reported>
<cell not reported>
<cell not reported>
<blank for demonstratio n>
Cuban
<section divider cell>
<section divider cell>
<section divider cell>
1a1c
Asian Indian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1a2c
Chinese
1a3c
Filipino
1a4c
Japanese
1a5c
Korean
1a6c
Vietnamese
1a7c
Other Asian
1b1c
Native Hawaiian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b2c
Other Pacific Islander
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b3c
Guamanian or Chamorro
1b4c
Samoan
1cc
Black/African American
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1dc
American Indian/Alaska Native
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1ec
White
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1fc
More than One Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1gc
Unreported/Chose Not to Disclose Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
Subtotal
Subtotal Cuban
<cell not reported>
<cell not reported>
<cell not reported>
<blank for demonstratio n>
Another Hispanic, Latino/a, or
Spanish Origin
<section divider cell>
<section divider cell>
<section divider cell>
1a1a
Asian Indian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1a2a
Chinese
1a3a
Filipino
1a4a
Japanese
1a5a
Korean
1a6a
Vietnamese
1a7a
Other Asian
1b1a
Native Hawaiian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b2a
Other Pacific Islander
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b3a
Guamanian or Chamorro
1b4a
Samoan
1ca
Black/African American
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
143 2023 UDS MANUAL | Instructions for Table 7
Line Race and Ethnicity
Total Patients 18 through 74 Years of
Age with Diabetes
(3a)
Number of Records Reviewed
(3b)
Patients with HbA1c >9.0%
or No Test During Year
(3f)
1da
American Indian/Alaska Native
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1ea
White
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1fa
More than One Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1ga
Unreported/Chose Not to Disclose Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
Subtotal
Subtotal Another Hispanic, Latino/a, or
Spanish Origin
<cell not reported>
<cell not reported>
<cell not reported>
<blank for demonstratio n>
Hispanic, Latino/a, or Spanish Origin,
Combined
<section divider cell>
<section divider cell>
<section divider cell>
1a1o
Asian Indian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1a2o
Chinese
1a3o
Filipino
1a4o
Japanese
1a5o
Korean
1a6o
Vietnamese
1a7o
Other Asian
1b1o
Native Hawaiian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b2o
Other Pacific Islander
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1b3o
Guamanian or Chamorro
1b4o
Samoan
1co
Black/African American
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1do
American Indian/Alaska Native
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1eo
White
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1fo
More than One Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
1go
Unreported/Chose Not to Disclose Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
Subtotal
Subtotal Hispanic, Latino/a, or Spanish
Origin
<cell not reported>
<cell not reported>
<cell not reported>
Total Hispanic, Latino/a, or Spanish
Origin
<cell not reported>
<cell not reported>
<cell not reported>
<blank for demonstratio n>
Not Hispanic, Latino/a, or Spanish
Origin
<section divider cell>
<section divider cell>
<section divider cell>
2a1
Asian Indian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
2a2
Chinese
2a3
Filipino
2a4
Japanese
2a5
Korean
2a6
Vietnamese
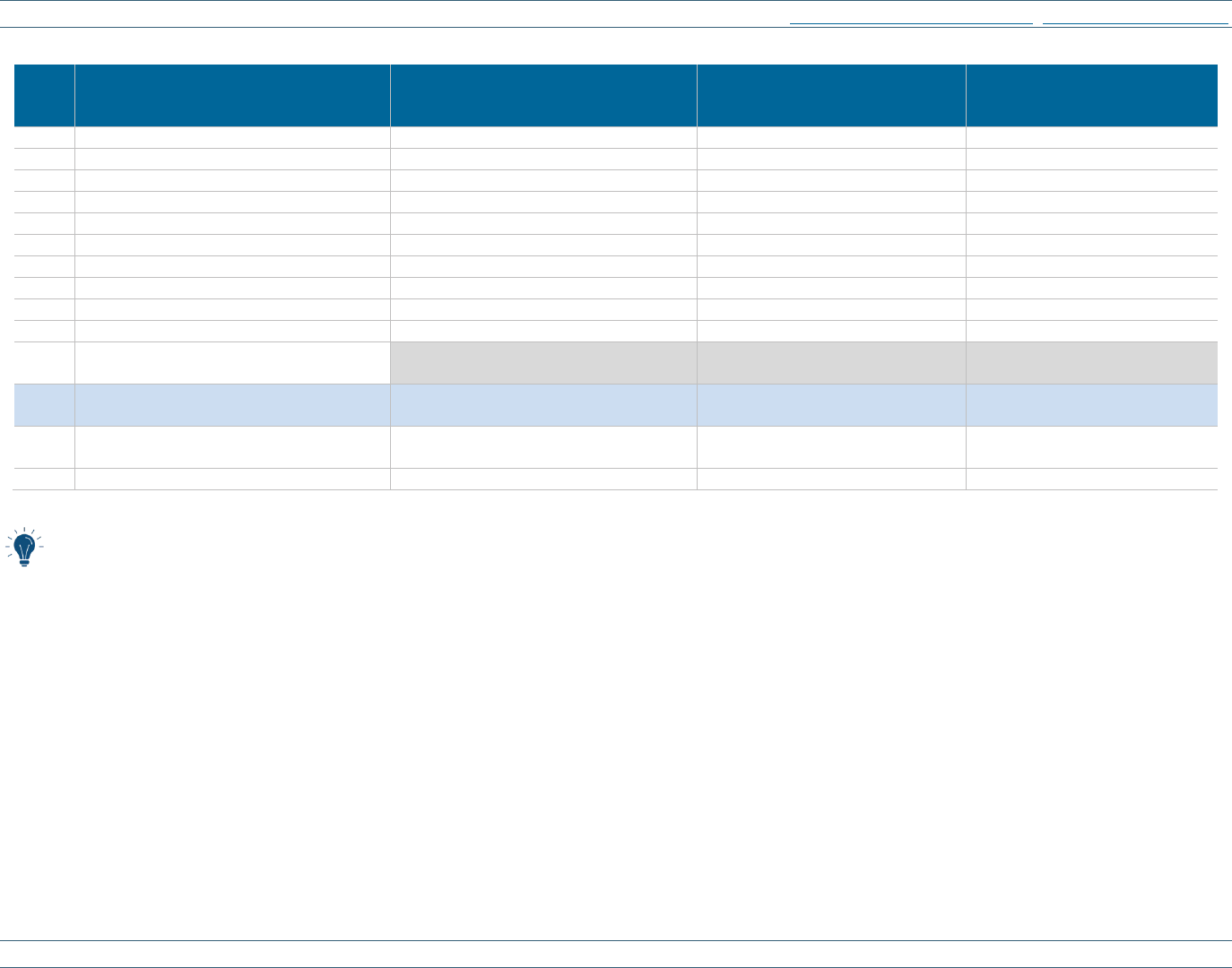
UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
144 2023 UDS MANUAL | Instructions for Table 7
Line Race and Ethnicity
Total Patients 18 through 74 Years of
Age with Diabetes
(3a)
Number of Records Reviewed
(3b)
Patients with HbA1c >9.0%
or No Test During Year
(3f)
2a7
Other Asian
2b1
Native Hawaiian
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
2b2
Other Pacific Islander
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
2b3
Guamanian or Chamorro
2b4
Samoan
2c
Black/African American
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
2d
American Indian/Alaska Native
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
2e
White
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
2f
More than One Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
2g
Unreported/Chose Not to Disclose Race
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
subtotal
Total Not Hispanic, Latino/a, or Spanish
Origin
<cell not reported>
<cell not reported>
<cell not reported>
<blank for demonstratio n>
Unreported/Chose Not to Disclose
Race and Ethnicity
<section divider cell>
<section divider cell>
<section divider cell>
h
Unreported/Chose Not to Disclose Race
and Ethnicity
<blank for demonstration>
<blank for demonstration>
<blank for demonstration>
i
Total
<cell not reported>
<cell not reported>
<cell not reported>
Table 7 Cross-Table Considerations:
• Patients with countable visits on Table 5 are generally eligible for inclusion in eCQMs reported on Table 7.
• The relationship between the denominators on Table 7 should be verified as reasonable when compared to the total number of patients by age on Table
3A and patients by race and ethnicity on Table 3B.
• The count of patients by diagnosis reported on Table 6A will not be the same counts as on Table 7, due to differences in criteria that must be met for
inclusion on Table 7.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
145 2023 UDS MANUAL | Instructions for Table 8A
Instructions for Table 8A: Financial Costs
Table 8A collects the total cost of all activities attributable to the calendar year that are within the approved scope
of project. Total costs include all costs within the health center scope of project, regardless of source of funding
(e.g., the Health Center Program award, patient and third-party payments, other grants and contracts). Thus, Table
8A describes what it costs to operate the health center’s approved scope of project.
There are no major changes to this table.
TABLE 8A: FINANCIAL COSTS
This table provides accrued costs and allocation of facility and non-clinical support services by cost center.
COLUMN REPORTING REQUIREMENTS
This table is made up of three columns: Accrued Costs (Column A), Allocation of Facility and Non-Clinical
Support Services (Column B), and the Total Cost after Allocation (Column C).
• Report the costs accrued in the calendar year, including depreciation, regardless of when (or, in the case of
donations on Line 18, if) actual cash payments were made.
• Report only the depreciation on capital assets, including those acquired with BPHC grants, NOT the full cost.
• Report interest payments on loans as an expense.
• DO NOT report bad debt expense or the repayment of the principal of a loan. These are not reported
anywhere in the UDS Report.
Note: A table summarizing the cost columns is included in FAQ for Table 8A
.
Column A: Accrued Costs
• Report the accrued costs in U.S. dollars (USD) associated with each of the service delivery cost centers listed.
See Line Definitions
for costs to include in each category.
• Report the total facility cost and the total cost of non-clinical support services (also referred to as
administrative costs) separately on Lines 14 and 15.
Column B: Allocation of Facility Costs and Non-Clinical Support Service Costs
• Report the allocation of facility and non-clinical support services costs (USD) (from Lines 14 and 15, Column
A) to each of the cost centers. See Allocation Methods
at the end of the instructions for this table for guidance
on allocating facility and non-clinical support service costs.
Column C: Total Cost After Allocation of Facility and Non-Clinical Support Services
• Report the cost (USD) of each of the cost centers listed on Lines 1–13.
• This cost is the sum of the direct cost, reported in Column A, plus the allocation of facility and non-clinical
support services costs, reported in Column B.
Note: Al
l UDS calculations involving total cost, such as total costs per patient, are based on Line 17 and DO
NOT include the value of donated services, supplies, or facilities reported on Line 18.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
146 2023 UDS MANUAL | Instructions for Table 8A
COST CENTER LINE REPORTING REQUIREMENTS
• Align costs reported on Table 8A with FTEs and services reported on Table 5. A crosswalk that classifies
personnel for various cost line items is available in Appendix B
.
• If an individual’s FTE is split across multiple lines on Table 5, the same proportional allocation must be used
for that individual’s personnel costs on this table.
Medical Personnel Costs (Line 1)
• Report all medical personnel costs, including salaries and fringe benefits for medical care personnel reported
on Table 5, Lines 1–12, including costs for personnel and contracted individuals.
• Include medical interns and residents who were paid directly or under a contract with their teaching
institution.
• Report vouchered or contracted medical services, including the cost of any medical visit paid for directly by
the health center, such as at-risk specialty care from a managed care organization (MCO) contract or other
specialty care.
• Report the amount of Promoting Interoperability Programs and any EHR incentive payments the health center
permits the provider to retain. (Also, report all Promoting Interoperability Programs EHR incentive payments
received during the calendar year from Medicare or Medicaid as cash receipts on Table 9E, Line 3a.) DO
NOT report the Promoting Interoperability Programs EHR incentive payments retained by the health center
on this table.
• Include costs for medical activities by medical personnel even when they are not directly providing care to
patients, such as chairing or attending meetings, supervising personnel, writing clinical protocols, designing
formularies, setting hours, or approving specialty referrals. The exception to this rule is when a medical
director or chief medical officer is engaged in non-clinical activities at the corporate level, in which case
time and costs are allocated to the non-clinical category.
• DO NOT report the costs of medical lab and X-ray personnel (report on Line 2) or dedicated HIT/EHR
informatics and QI personnel (report on Line 12a).
• DO NOT report the costs of intake, patient health records, and billing and collections, as these are considered
non-clinical support costs (report on Line 15).
Medical Lab and X-Ray Costs (Line 2)
• Report all costs for the provision of medical lab and X-ray services reported on Table 5, Lines 13 and 14
(including sonography, mammography, and any advanced forms of tomography), including salaries and
fringe benefits provided directly or under contract.
• DO NOT include other direct medical costs, including but not limited to medical supplies, equipment
depreciation, and related travel (report on Line 3).
• DO NOT include dental lab and X-ray costs (report as Dental, Line 5).
• DO NOT include costs for retinography readings by specialists (most commonly for diabetic patients) (report
as Vision Services, Line 9a).
Other Direct Medical Costs (Line 3)
• Report all non-personnel direct costs for medical care, including but not limited to supplies, equipment
depreciation, related travel, medical education expense not including fringe benefits (which are reported on

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
147 2023 UDS MANUAL | Instructions for Table 8A
Line 1), meeting registration and travel, uniform laundering, recruitment, membership in professional
societies, books, and journal subscriptions.
• Report the cost of the medical aspects of an HIT/EHR system, including but not limited to the depreciation of
software and hardware, training costs, and licensing fees. If the HIT/EHR system is used in other service
categories (e.g., mental health, dental), allocate costs to each of the services in which it is used.
• DO NOT report non-clinical support services and facility costs associated with these cost centers (report on
Lines 14 and 15, Column A, and then allocate them to the cost center in Column B). (See also FAQ for Table 5
).
Total Medical (Line 4)
Sum Lines 1 + 2 + 3.
Other Clinical Services (Lines 5–10)
This category includes personnel and related costs for dental, mental health, substance use disorder, pharmacy,
vision, and services rendered by other professional personnel (e.g., chiropractors, naturopaths, occupational and
physical therapists, speech and hearing therapists, podiatrists). Unlike medical, all costs are included on a single
line.
• Report all direct costs for the provision of services in the listed service area, including but not limited to
personnel, fringe benefits, training, contracted services, office supplies, equipment depreciation, related
travel, HIT/EHR, lab services, and X-ray.
• DO NOT report non-clinical support services and facility costs associated with these cost centers (report on
Lines 14 and 15, Column A, and then allocate them to the cost center in Column B). (See also FAQ for Table 5
.)
Dental (Line 5)
• Report all direct costs for the provision of dental services reported on Table 5, Lines 16–18.
Mental Health (Line 6)
• Report all direct costs for the provision of mental health services reported on Table 5, Lines 20a–20c, other
than substance use disorder services.
• If a behavioral health program provides both mental health and substance use disorder services, the cost
should be allocated between the two services. Allocations must align with FTEs and visits reported on Table
5. DO NOT make any allocations based on the detail reported on the Selected Service Detail Addendum.
Substance Use Disorders (Line 7)
• Report all direct costs for the provision of substance use disorder services reported on Table 5, Line 20.
• If a behavioral health program provides both mental health and substance use disorder services, the cost should
be allocated between the two services. Allocations must align with FTEs and visits reported on Table 5.
• DO NOT make any allocations based on the detail reported on the Selected Service Detail Addendum.
Pharmacy (Not Including Pharmaceuticals) (Line 8a)
• Report all direct costs for the provision of pharmacy services reported on Table 5, Lines 23a–23d.
• If 340B drugs are purchased by or on behalf of a clinic and dispensed by a contract pharmacy, report the full
dispensing fee and any other service fees (such as “share of profit,” pharmacy benefit manager costs,
inventory fees, ordering fees, administrative fees, or a charge for pharmacy computer services) on this line,

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
148 2023 UDS MANUAL | Instructions for Table 8A
regardless of whether the health center pays the full amount, pays a net after subtraction of revenue at the
contract pharmacy, or simply receives a reduced net payment from the pharmacy.
• DO NOT include the cost of pharmaceuticals (report on Line 8b).
• DO NOT report the cost of personnel engaged in assisting patients to become eligible for free
pharmaceuticals from manufacturers (often called PAPs) (report as Eligibility Assistance on Line 11e).
Pharmaceuticals (Line 8b)
• Report all costs for the purchase of pharmaceuticals only.
• Include vaccines and medications administered at the health center (e.g., penicillin, Depo-Provera,
buprenorphine).
• Report the full cost of 340B drugs purchased by or on behalf of the clinic and dispensed by a contract
pharmacy. This includes 340B drugs paid for in full by the health center, as well as the full cost of drugs paid
for through an agreement whereby the pharmacy initially pays for the drugs and then deducts the cost from
their receipts.
• DO NOT include other supplies here (report on Line 8a, Pharmacy).
• DO NOT include the value of donated pharmaceuticals (report on Line 18, Column C).
Note: Allocation of Facility and Non-Clinical Support Services, Column B, is grayed out on Pharmaceuticals,
Line 8b. Report any overhead allocation for pharmaceuticals on Line 8a, Pharmacy.
Other Professional (Line 9)
• Report all direct costs for the provision of other professional and ancillary health care services reported on
Table 5, Line 22, including but not limited to, podiatry, chiropractic, acupuncture, naturopathy, speech and
hearing pathology, or occupational and physical therapy. (A more complete list appears in Appendix A
.)
• DO NOT report the cost of WIC, Program of All-Inclusive Care for the Elderly (PACE), or ADHC here
(report on Line 12, Other Program-Related).
Note: Use the “specify” field to detail the other professional costs reported on this line.
Vision (Line 9a)
• Report all direct costs for the provision of vision services reported on Table 5, Lines 22a–22c, including
optometry, ophthalmology, and vision support personnel.
• Include the cost of frames and lenses.
• Include costs for retinography (including for diabetic patients) and any contracted costs for reading the
results.
Total Other Clinical (Line 10)
Sum of Lines 5 + 6 + 7 + 8a + 8b + 9a.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
149 2023 UDS MANUAL | Instructions for Table 8A
Enabling (Lines 11a–11h, 11)
Enabling services include a wide range of services that support and assist primary care and facilitate patient
access to care. Report all direct costs for the provision of enabling services reported on Table 5, Lines 24–28,
including salary, fringe benefits, supplies, equipment depreciation, related travel, and contracted services.
• Report enabling services by function. Use Lines 11a–11h to detail the cost of seven specific types of enabling
services and an “other” category for all other forms of enabling services.
o Case management (11a)
o Transportation (11b)
o Outreach (11c)
o Health education (11d)
o Eligibility assistance (includes assistance in obtaining program eligibility, including PAP and health
insurance coverage options) (11e)
o Translation/interpretation services (11f)
o Other (specify the other forms of enabling services included on this line if used) (11g)
o Community health workers (11h)
• The enabling services personnel costs reported (for Lines 11a and 11d) must be consistent with the FTEs and
visits reported on Table 5.
Note: Descriptions of the services and personnel that belong in each of these categories are included in the
Instructions for Table 5 and in Appendix A
.
Note: The overhead to be allocated to all enabling service categories is reported in Column B on Line 11, Total
Enabling Services. Allocation of Facility and Non-Clinical Support Services, Column B, is grayed out for all
other enabling service categories.
Total Enabling Services (Line 11)
Sum of Lines 11a + 11b + 11c + 11d + 11e + 11f + 11g + 11h.
Other Program-Related (Line 12)
• Report costs of all in-scope items and programs not classifiable as medical, dental, behavioral, vision,
enabling, or other professional health services (Lines 1–11).
• Include programs and items such as WIC, child care centers, ADHC centers, fitness centers, Head Start and
Early Head Start, housing, clinical trials, research, employment training, the cost of space, staff, and other
items leased to others, retail pharmacy services provided to non–health center patients, the amount of grant
funds passed through to other agencies if patient activity is not included in the health center’s reporting, and
similar activities.
• Report salaries, fringe benefits, supplies, equipment depreciation, related travel, and contracted services.
• Report the estimated cost of facilities, programs, or services that may be part of the health center scope of
project but are not tied to health center patient activity. Examples might include renting out space in the health
center or providing retail pharmacy services to non-patient members of the community.
• Describe the programs and their costs using the “specify” field provided. The program descriptions should
correspond to the “specify” field on Table 5, Line 29a, where FTE are reported.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
150 2023 UDS MANUAL | Instructions for Table 8A
Quality Improvement (QI) (Line 12a)
• Report all direct costs for the health center’s QI program reported on Table 5, Line 29b, including all
personnel who are dedicated in whole or in part to QI.
• Include the costs of personnel dedicated to the QI program and/or HIT/EHR system development and
analysis, their fringe benefits, supplies, equipment depreciation, related travel, and contracted services.
• DO NOT allocate portions of the time and cost that QI personnel spend attending meetings, participating in
peer review, designing or interpreting QI findings, and so on to other service categories.
Total Enabling, Other Program-Related, and Quality Improvement Services (Line 13)
Sum of Lines 11 + 12 +12a.
Facility Costs (Line 14)
• Report costs associated with FTE reported on Table 5, Line 31, including all personnel dedicated to facility
services and their fringe benefits, as well as supplies, equipment depreciation, related travel, and contracted
services.
• Include rent and/or depreciation (not asset acquisition cost), facility mortgage interest (but not principal)
payments, utilities, security, grounds keeping, facility maintenance and repairs, janitorial services, and all
other related costs.
• DO NOT report the cost of space leased to others on this line. Instead, report it as Other Program-Related
costs on Line 12. The receipts associated with these leases are reported on Table 9E, Line 10.
Note: Allocation of Facility and Non-Clinical Support Services, Column B, and Total Cost After Allocation of
Facility and Non-Clinical Support Services, Column C, are grayed out for Facility Costs, Line 14.
Non-Clinical Support Services Costs (Line 15)
• Report non-clinical support services costs (sometimes referred to as administrative costs) associated with the
personnel reported on Table 5, Lines 30a–30c and 32, including the cost of all non-clinical support services
personnel, senior administrative personnel (CEO, CFO, COO, HR director, et al.), billing and collections
personnel, patient health records and intake personnel, and the costs associated with them.
• Include salaries, fringe benefits, supplies, equipment depreciation, related travel, and contracted services.
• Report corporate costs (e.g., purchase of facility and liability insurance, not including malpractice insurance,
audits, legal fees, interest payments on non-facility loans, and communication costs including phone and
internet).
• Report costs attributable to the board of directors, including travel expenses, meetings, directors’ and officers’
insurance, conference registration fees, and similar expenses.
• Some grant programs limit the proportion of grant funds that may be used for non-clinical support services.
DO NOT consider those limits on “administrative” costs for those programs when completing Lines 14 and
15. The non-clinical support services and facility categories for this report include all such personnel working
at the health center, whether or not that cost was includable or considered “administrative” in a grant budget.
• DO NOT report bad debt expenses for patient services here or anywhere on this table. Report self-pay bad
debt as an adjustment to patient self-pay charges on Table 9D, Line 13.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
151 2023 UDS MANUAL | Instructions for Table 8A
Note: Allocation of Facility and Non-Clinical Support Services, Column B, and Total Cost After Allocation of
Facility and Non-Clinical Support Services, Column C, are grayed out for Non-Clinical Support Services Costs,
Line 15.
Total Facility and Non-Clinical Support Services (Line 16)
Sum of Lines 14 + 15.
Note: Since the direct facility and non-clinical support cost in Column A is allocated to the other cost centers,
nothing is reported in Columns B or C on Lines 14–16. These fields are grayed out.
Total Accrued Costs (Line 17)
22
Sum of Lines 4 + 10 + 13 + 16.
Note: Allocation of Facility and Non-Clinical Support Services, Column B, is grayed out for Total Accrued
Costs, Line 17.
Value of Donated Facilities, Services, and Supplies (Line 18, Column C)
• Report the total imputed (assigned) value of all in-kind and donated services, facilities, and supplies that are
necessary to the health center’s operation applicable to the calendar year and within your scope of project as
follows.
• Report the estimated reasonable acquisition cost of donated personnel, supplies, services, space rental, and
estimated depreciation for the use of donated equipment.
• Report donated pharmaceuticals (including vaccines) at the price that would be paid under the
federal Section
340B Drug Pricing Program, NOT the manufacturer’s suggested retail price.
• Estimate reasonable acquisition cost of donated personnel at the cost of hiring comparable personnel.
• If the health center is not paying NHSC for assignees, include the full market value of NHSC federal
assignee(s), including “ready responders.” Capitalize NHSC-furnished equipment, including a dental
operatory, at the amount reported on the NHSC Equipment Inventory Document, and report the appropriate
depreciation expense for the calendar year.
• Use the “specify” field provided to describe the donated items and amounts in detail.
• DO NOT include the value of donations in Column A on the lines above.
• DO NOT use the sum of the usual and customary charges rendered by providers who donate their services to
value their donation.
Note: Accrued Cost, Column A, and Allocation of Facility and Non-Clinical Support Services, Column B, are
grayed out for Value of Donated Facilities, Services, and Supplies, Line 18.
Total with Donations (Line 19)
Sum of Lines 17 + 18, Column C.
Note: Accrued Cost, Column A, and Allocation of Facility and Non-Clinical Support Services, Column B, are
grayed out for Total with Donations, Line 19.
22
This is the amount used in the BPHC calculation of measures involving total cost.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
152 2023 UDS MANUAL | Instructions for Table 8A
COLUMN B: FACILITY AND NON-CLINICAL SUPPORT SERVICES ALLOCATION
INSTRUCTIONS
There are multiple ways that facility and non-clinical support services (Lines 14 and 15, Column A) may be
allocated to the cost centers in Column B (Lines 1–13).
• Use the simplest method that produces a reasonably accurate result that is comparable to that obtained by a
more complex method.
• Use the method described below if a more accurate method is not available.
• It is recommended that facility and non-clinical support costs that can be directly associated to a cost center
be allocated first when those costs represent a significant portion of the cost being allocated to the cost center.
For instance, the facility and non-clinical support costs of a service delivery site that only provides dental
services can be directly allocated to Dental, Line 5. The HIT/EHR support personnel who support the medical
department can be directly allocated to Medical, Line 1.
• The remaining allocation of indirect costs can be done using a single- or multi-step allocation process such as
those described below.
• A preferable and commonly used two-step method is to first allocate facility costs based upon the proportion
of square feet used by each cost center at each location. The second step is to allocate the remaining non-
clinical support service cost based upon the percentage of direct cost that is non-clinical support, after the
allocation of facility cost is applied.
• Given that managing personnel consumes most of administrative overhead, a one-step method based solely on
the percentage distribution of square feet will usually NOT produce an accurate allocation of overhead.
• When a two-step method is not used, a typical one-step method uses the proportion of facility and non-clinical
support costs (overhead costs) to total direct cost (excluding facility, non-clinical support, and
pharmaceuticals). The resulting percentage is multiplied by the total direct cost for each cost center to arrive
at the overhead allocation for each cost center.
Facility
Facility cost is commonly allocated based upon the proportion of square feet used by each cost center at each
location.
Note: The record of square feet used by each cost center at each location should be updated each year or as space
use changes.
Non-Clinical Support Services
Some of the indirect non-clinical support costs may be allocated separately based on known use or other factors.
• Adjust for decentralized front desk personnel, billing and collection systems and personnel, etc.
• Allocate costs for billing and accounting systems based on use.
• Allocate various components of non-clinical services based on their use when these amounts are significant,
and the use is not shared equally.
• Allocate a lesser percentage to large purchased-service costs (e.g., lab, X-ray, pharmacy) that are known to
consume less overhead.
• Allocate the remaining indirect non-clinical support cost to each cost center based on the proportion each cost
center’s direct cost plus previously allocated overhead cost is of the total of those costs.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
153 2023 UDS MANUAL | Instructions for Table 8A
Other Allocation Considerations
• Lines 1 and 3 both refer to aspects of the medical practice. It is acceptable to report the allocation of all
medical facility and non-clinical support services on Line 1 if a more appropriate allocation between Lines 1
and 3 is not available.
• Pharmaceuticals (Line 8b) does not have an open cell to report an allocation. This is because pharmaceuticals
are exclusively purchased goods that have no personnel included and, therefore, consume a significantly
lesser facility and non-clinical support charge than services involving personnel. Any allocation of overhead
(which is usually minimal) that you choose to make for pharmaceuticals must be reported on Line 8a.
• There may be other sizable contracted or purchased goods and services that use less facility and non-clinical
support. A lesser allocation may be appropriate.
FAQ FOR TABLE 8A
1. How do we account for donated services?
If a provider comes to your health center and renders a service to your patients, report both the FTE (on Table
5) and the value, which is determined by “what the health center would reasonably pay” for the time (not the
service), on Table 8A, Line 18. For example, if an optometrist sees five patients in a 2-hour period, report the
amount you would pay an optometrist for 2 hours of work, not the total charges for the five visits.
However, if you refer a patient to a provider outside of your health center for a service and the provider
donates these services, DO NOT report the activity, the charge, or the value of the time or service on the
UDS. This is outside of the health center’s scope of project and is considered a donation made by the external
provider to the patient. For example, if you refer a patient to a cardiologist who provides free consultation,
DO NOT count the visit or the monetary value of the provider’s service.
2. How do we account for donated drugs?
If drugs are donated directly to the health center, which then dispenses them to a patient, calculate and report
on Line 18 the value of the drug at what the health center would reasonably pay for them. This is NOT the
retail cost of the drug; it is the 340B price of the drug—an amount that is generally 40–60% of the average
wholesale price (AWP).
3. We get most of our vaccines through Vaccines for Children (VFC) or other state and county programs.
Are these considered donated drugs and accounted for here?
Yes. Report the value of donated drugs that are used in the health center, such as vaccines, on Line 18 in
Table 8A―again, at the reasonable cost based on 340B drug pricing or at a discounted price from the AWP.
4. Our doctors were paid the EHR incentive payments directly by CMS. If we let them keep some or all of
these dollars, are they reported anywhere on Table 8A?
Yes. Establish reporting mechanisms whereby your providers inform you of payments received and account
for these funds. If providers are permitted to retain some or all these funds, report the amount as additional
provider compensation on Line 1. In addition, report the Promoting Interoperability EHR payments received
from Medicare or Medicaid on Table 9E, Line 3a.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
154 2023 UDS MANUAL | Instructions for Table 8A
5. What method of overhead (facility and non-clinical support services) allocation should we use for this
table?
There are multiple ways that facility and non-clinical support services may be allocated to the cost centers in
Column B. Use the method that produces a reasonably accurate result. See the suggested single- and multi-
step allocation methods
for additional information on these methods.
6. Do we need to allocate overhead for purchased goods and services?
Purchased (contracted) services DO NOT warrant a full overhead charge, given that they DO NOT involve
the management of personnel. However, the procurement and supervision of those arrangements do consume
overhead that should be reported. Assuming the amount of purchased services are significant, a lesser
overhead allocation set at a rate that covers the cost of accounting, inventory management, and contract
management is appropriate.
7. Why do our financial statements NOT tie to the UDS financials?
The UDS financials (Tables 8A, 9D, and 9E) will NOT tie to your financial statements for some or all of the
following reasons:
(1) The UDS Report is to reflect calendar year January 1–December 31 data, but the health center’s fiscal
year may be a different period.
(2) Activity outside the scope of the federal project is included in the health center’s financial statements but
excluded in the UDS.
(3) Net patient service revenue that could be estimated from table 9D (charges less adjustments) may differ
from the financial statements because the UDS only reports self-pay bad debt rather than the full
adjustment for bad debt attributable to all payers and circumstances.
(4) Settlement and wrap revenue is only reported in the UDS upon its receipt, and health centers may be able
to recognize and report some or all of the revenue on an accrual basis in the period it is earned.
(5) Table 9E reports all non–patient service-related revenue on a cash basis, and health centers will recognize
this revenue on an accrual basis in their financial statements.
8. What do we need to report in the different columns of this table?
The column definitions
are detailed on Table 8A. Below is a summary of what to include in each column.
Accrued Cost (a)
Allocation of Facility and Non-
Clinical Support Services (b)
Total Cost After Allocation of Facility
and Non-Clinical Support Services (c)
Costs attributable to the calendar year
by cost center.
Report costs of:
• personnel
• fringe benefits
• supplies
• equipment
• depreciation
• interest paid
• related travel
Exclude bad debt and repayment of
principal on loans.
Allocation of facility and non-clinical
support services (Column A, Lines 14
and 15) to each cost center.
Note: Total of Column B must be
equal to Column A, Line 16.
Represents cost to operate services.
Note: Sum of Columns A + B (done
automatically in EHBs).

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
155 2023 UDS MANUAL | Instructions for Table 8A
9. How are awardee-subrecipient and contractor relationships to be reported?
Report the total cost of subawardee project operations in the UDS Report of the awarded health center that
provided a subaward to the other health center (subawardee). If the subawardee is also a Health Center
Program awardee, the subawardee will also report this activity on its UDS.
Activity associated with contracts for services purchased by one health center and provided by another health
center will be reported in the UDS Report of both health centers. The health center providing the services
reports the costs and activity of the services provided. The health center purchasing the services reports the
cost and the activity of the services purchased.
10. How do we report the cost of shared or common space?
All facility costs, including the cost of common space, are included and reported on Line 14, Facility, in
Column A, Accrued Costs.
11. How do we report the cost of space, staff, or other items that the health center leased or donated to
others?
The cost of space, staff, and other items leased or donated by the health center to others is reported on Line
12, Other Program-Related Services.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
156 2023 UDS MANUAL | Instructions for Table 8A
TABLE 8A: FINANCIAL COSTS
Calendar Year: January 1, 2023, through December 31, 2023
Line Cost Center Accrued Cost (a)
Allocation of
Facility and Non-
Clinical Support
Services (b)
Total Cost After
Allocation of
Facility and Non-
Clinical Support
Services (c)
[section divide]
Financial Costs of Medical Care
[section divide]
[section divide]
[section divide]
1
Medical Personnel
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
2
Lab and X-ray
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
3
Medical/Other Direct
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
4
Total Medical Care Services
(Sum of Lines 1 through 3)
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for section divide]
Financial Costs of Other Clinical
Services
[blank for section divide]
[blank for section divide]
[blank for section divide]
5
Dental
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
6
Mental Health
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
7
Substance Use Disorder
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
8a
Pharmacy (not including pharmaceuticals)
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
8b
Pharmaceuticals
[blank for demonstration]
[Cell not reported]
[blank for demonstration]
9
Other Professional
(specify___)
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
9a
Vision
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
10
Total Other Clinical Services
(Sum of Lines 5 through 9a)
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for section divide]
Financial Costs of Enabling and Other
Services
[blank for section divide]
[blank for section divide]
[blank for section divide]
11a
Case Management
[blank for demonstration]
[Cell not reported]
[blank for demonstration]
11b
Transportation
[blank for demonstration]
[Cell not reported]
[blank for demonstration]
11c
Outreach
[blank for demonstration]
[Cell not reported]
[blank for demonstration]
11d
Health Education
[blank for demonstration]
[Cell not reported]
[blank for demonstration]
11e
Eligibility Assistance
[blank for demonstration]
[Cell not reported]
[blank for demonstration]
11f
Interpretation Services
[blank for demonstration]
[Cell not reported]
[blank for demonstration]
11g
Other Enabling Services
(specify___)
[blank for demonstration]
[Cell not reported]
[blank for demonstration]
11h
Community Health Workers
[blank for demonstration]
[Cell not reported]
[blank for demonstration]
11
Total Enabling Services
(Sum of Lines 11a through 11h)
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
12
Other Program-Related Services
(specify___)
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
12a
Quality Improvement
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
13
Total Enabling and Other Services
(Sum of Lines 11, 12, and 12a)
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
157 2023 UDS MANUAL | Instructions for Table 8A
Line
Cost Center
Accrued Cost (a)
Allocation of
Facility and Non-
Clinical Support
Services (b)
Total Cost After
Allocation of
Facility and Non-
Clinical Support
Services (c)
[blank for section divide]
Facility and Non-Clinical Support
Services and Totals
[blank for section divide]
[blank for section divide]
[blank for section divide]
14
Facility
[blank for demonstration]
[Cell not reported]
[Cell not reported]
15
Non-Clinical Support Services
[blank for demonstration]
[Cell not reported]
[Cell not reported]
16
Total Facility and Non-Clinical Support
Services
(Sum of Lines 14 and 15)
[blank for demonstration]
[Cell not reported]
[Cell not reported]
17
Total Accrued Costs
(Sum of Lines 4 + 10 + 13 + 16)
[blank for demonstration]
[Cell not reported]
[blank for demonstration]
18
Value of Donated Facilities, Services, and
Supplies (specify___)
[Cell not reported]
[Cell not reported]
[blank for demonstration]
19
Total with Donations
(Sum of Lines 17 and 18)
[Cell not reported]
[Cell not reported]
[blank for demonstration]
Table 8A Cross-Table Considerations:
• The personnel and visits on Table 5 are routinely compared to the costs on Table 8A. See the crosswalk of
comparable fields in Appendix B
.
• Report the value of donated goods and services received on Table 8A. Report cash donations received on
Table 9E.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
158 2023 UDS MANUAL | Instructions for Table 9D
Instructions for Table 9D: Patient Service Revenue
This table collects patient service revenue, including charges, collections, and adjustments attributable to the
calendar year.
The Health Center Program Compliance Manual
requires that all health centers have a fee schedule, based on
locally prevailing rates and actual health center costs, and that they discount these fees (see discussion regarding
sliding fee discounts) based on a patient’s income and family/household size. Health centers are also required to
make reasonable efforts to collect payment from patients and/or their third-party payers, consistent with Health
Center Program Compliance Manual requirements.
Line 8c for the COVID-19 Uninsured Program has been removed because the deadlines for COVID-19 testing
and treatment claims submissions ended on March 22, 2022, and vaccine administration claims ended on April 5,
2022.
TABLE 9D: PATIENT SERVICE REVENUE
This table reports charge, collection, and adjustment data for patient services provided within the health center’s
scope of federal project.
Revenue reported on Table 9D generally aligns with the classification of patients by type of medical insurance
reported on Table 4. A crosswalk that shows this alignment is available in Appendix B
.
ROWS: PAYER CATEGORIES AND FORM OF PAYMENT
Five major payer categories are listed: Medicaid, Medicare, Other Public, Private, and Self-Pay. All but Self-Pay
have three sub-categories: non-managed care, capitated managed care, and fee-for-service managed care.
Only report charges, collections, and adjustments as managed care when all of the following criteria are met:
• There is a contract with an MCO where the MCO assumes some risk.
• Managed care enrollees are assigned to the health center and/or a primary care provider (PCP) within the
health center and must obtain approval to be reassigned to another PCP.
• Monthly membership data are provided by or are available from the MCO.
• Enrollees must receive prior approval from their PCP prior to being seen elsewhere for a reimbursable non-
emergency care service or contracted specialty care.
Payer Categories
Medicaid (Lines 1–3)
• Report all services billed to and paid for by Medicaid (Title XIX), including:
o Medicaid managed care programs that may be operated by private insurers. For example, in states with a
capitated Medicaid program, the health center may have a contract with a private plan like Blue Cross to
administer the plan. The payer would be Medicaid, even though the actual payment may have come from
Blue Cross.
o EPSDT, which has various names in different states and is a part of Title XIX. The EPSDT program
includes some children who are eligible for limited outpatient screening and treatment services only and
are not included in the rest of the Medicaid program. Report their charges on Line 1.
o CHIP, which has different names in different states, if paid through Medicaid.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
159 2023 UDS MANUAL | Instructions for Table 9D
o Medicaid expansion programs that provide funds for eligible individuals to purchase their own insurance,
if it is possible to identify them. Otherwise report as Private.
o The portion of charges for dually eligible patients that are reclassified to Medicaid after being initially
submitted to Medicare.
o The portion of the charge paid by Medicaid for Medicaid patients enrolled in a “share of cost” program.
o ADHC or Program of All-Inclusive Care for the Elderly (PACE) if administered by Medicaid. Treat as
discussed in Appendix B
.
Medicare (Lines 4–6)
• Report all services billed to and paid for by Medicare (Title XVIII), including:
o Medicare managed care programs, including Medicare Advantage plans run by private insurers. For
example, where the health center has a contract with a private plan like Blue Cross for Medicare
Advantage, consider the payer to be Medicare, even though the actual payment may come from Blue
Cross.
o The portion of charges for patients covered through multiple insurances (e.g., Medicare and Medicaid,
Medicare and Private) that are initially paid for by Medicare.
o ADHC or PACE if administered by Medicare. Treat as discussed in Appendix B
.
Other Public (Lines 7–9)
• Report all services billed to and paid for by state or local government programs, including:
o CHIP when paid for through private insurers. (See Lines 1–3 if CHIP is paid through Medicaid.)
o Family planning programs such as Title X programs, BCCEDPs (with various state names), and other
dedicated state or local programs.
Note: A
lthough these categorical grant programs are considered Other Public payers, patients are generally
classified as Uninsured on Table 4 because the programs do NOT cover comprehensive primary care.
o State-run insurance plans.
o Municipal or county jails and state prisons.
o Public schools and institutions that engage with the health center on a fee-for-service or other service-
based contract basis.
• DO NOT include:
o State or local indigent care programs. Report their charges, any associated self-pay collections, etc. on the
Self-Pay line of Table 9D, Line 13 and program funds received on Table 9E, Line 6a, as described below.
o Third-party coverage purchased through state or federal exchanges (which may be subsidized). Report as
Private.
o Patients covered through subsidies from a Medicaid expansion program. Report as Medicaid.
Private (Lines 10–12)
• Report all services billed to and paid for by private (commercial) insurance companies or by other third-party
payers, including:
o Insurance purchased for public employees or retirees, such as Tricare, Trigon, and the Federal Employees
Health Benefits Program, as these are benefits belonging to the patient.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
160 2023 UDS MANUAL | Instructions for Table 9D
o Workers’ compensation, which is a form of liability coverage for employers.
o Insurance purchased through state exchanges, unless you can identify the patient as being enrolled
through purchased subsidies from a Medicaid expansion program.
o Contract payments from other organizations who engage the clinic on a fee-for-service or other
reimbursement basis, such as a Head Start program that pays for annual physical exams at a contracted
rate or a private school, private jail, or large company that pays for a provision of medical care at a per-
session or other negotiated rate.
o Supplemental insurance (plans that typically cover some amounts not paid or disallowed by Medicare).
• DO NOT report Medicaid, Medicare, or Other Public managed care programs administered by private
insurers as Private.
Self-Pay (Line 13)
• Report all charges and related collections where the patient is responsible, including:
o The full charge of services for uninsured patients with no insurance coverage.
o Co-payments, deductibles, and charges to insured individuals for non-covered services that become the
patient’s personal responsibility.
o Medicaid patients enrolled in a “share of cost” program in which they pay some portion of the fee as a co-
payment or a deductible. In this case, reclassify the patient’s share of the cost to Self-Pay, Line 13.
o State or local indigent care programs that subsidize services rendered to the uninsured.
Report all charges for these services and collections from patients on the Self-Pay line (Line 13,
Columns A and B).
Report all amounts not collected or due from the patients as sliding fee discounts or bad debt write-
off, as appropriate, on Line 13, Columns E and F.
Report collections from the associated state and local indigent care programs on Table 9E, Line 6a,
and specify the name of the program paying for the services.
Form of Payment
Non-Managed Care—Fee-for-Service
A payment model in which procedures and services are separately charged and paid for patients not assigned to
the health center under a managed care contract. Third-party payers pay some or all of the bill, generally based on
agreed-upon maximums or discounts.
Managed Care—Capitated
A payment model in which a health center contracts with an MCO for a list of services. The MCO pays the health
center a capitation fee (a set amount, usually paid monthly, for each enrolled patient assigned to the health center)
regardless of whether any services were rendered during the month. No further direct payment is provided if
the services rendered are on the list of services covered by the capitation fee in the agreement between the health
center and the MCO.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
161 2023 UDS MANUAL | Instructions for Table 9D
Managed Care—Fee-for-Service
A payment model in which a health center contracts with an MCO, is assigned patients for whom the health
center is responsible for providing primary care services and is reimbursed on a fee-for-service (or encounter-rate)
basis for covered services.
Managed Care—Combined Capitation and Fee-for-Service
A common payment model in which some of the services covered by the MCO are reimbursed with a capitation
payment and the remainder of covered services are “carved out” and reimbursed on a fee-for-service basis. Carve-
outs may include treatment of specific diseases (e.g., HIV) or specific services (e.g., prenatal care, labor/delivery).
In this situation, the charges, collections, and adjustments are separately reported on the corresponding managed
care lines—those that are for a defined set of services covered by the capitation and those that are reimbursed on a
fee-for-service basis.
COLUMNS: CHARGES, PAYMENTS, AND ADJUSTMENTS RELATED TO SERVICES
DELIVERED
Column A: Full Charges This Period
• Report total charges for patient services provided during the calendar year by each payer source. This will
initially reflect the total full charges (per the health center’s fee schedule) for patients whose services were
billed to that payer category during the calendar year.
• Report charges based on the organization’s fee schedule for services that are billed to and covered in whole or
in part by a payer, or the patient, even if some or all of them are subsequently written off as contractual
adjustments, sliding fee discounts, or bad debts. Always report full gross charges according to the health
center fee schedule, NOT a contracted or negotiated rate.
Note: Under no circumstances should the actual amount paid by Medicaid or Medicare (such as those described
as FQHC, G-code, or T-code rates) or the amount paid by any other payer be used as the actual charges. Charges
must come from the health center’s schedule of fees, typically based on CPT codes, or retail charge (for
pharmacy).
• Report pharmaceuticals dispensed through a (340B) contract pharmacy at the pharmacy’s UCR gross charge,
even though they have a contracted rate with third-party payers.
• Include charges for ancillary services, such as laboratory and imaging.
• Include charges for eyeglasses, durable medical equipment, and other similar supply items.
• Include charges for dispensing or injecting pharmaceuticals donated to the health center or directly to a
patient if they appear on bills and are collected from first and third parties.
• DO NOT report:
o “contractual adjustments” as a charge. Instead, report the difference between gross charges and the
amount reimbursed from third parties as an Adjustment
in Column D.
o charges that are generally not billable to or covered by traditional third-party payers. Some examples
include WIC services, parking or job training, and transportation and similar enabling services (not
generally included in Column A, except where the payer [e.g., Medicaid] accepts billing and pays for
these services).

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
162 2023 UDS MANUAL | Instructions for Table 9D
Reclassifying Charges
Services may have been paid for by more than one source. For example, a patient may have a portion of their
charge paid by their primary insurance and may have the remainder paid by a secondary insurer or the patient or
both. Management information systems should automatically reclassify charges rejected by a payer.
• In these instances, report the charge accepted by the primary payer along with any negotiated adjustment
amount for their portion of the services to that payer line.
• Transfer the charges for the balance to the secondary payer; after the secondary payer claim settles, transfer
the balance to a tertiary payer (if one exists) and, eventually, to the patient as a self-pay charge.
• Only report the amount charged to each payer, reclassifying any portion of the charge to secondary or tertiary
payers (if they exist).
• If reclassifying cannot be done automatically, manually transfer the amount rejected from the initial payer to
the next payer.
• DO NOT reclassify charges by using an adjustment and rebilling to another payer category; this will result in
an overstatement of total gross charges by reporting the charges twice.
Column B: Amount Collected This Period
• Report in Column B the gross receipts for the calendar year, including receipts for services that may have
been rendered in a prior calendar year.
• Report FQHC reconciliations, managed care pool distributions, pay-for-performance (P4P) payments, quality
bonuses, court settlements, and other payments in Column B and in Columns C1, C2, C3, and/or C4.
• When a contract pharmacy is dispensing 340B drugs on behalf of the health center, report the total cash
received by the pharmacy separately for patients and third-party payers.
• Report the managed care capitation payments (monthly payments) received during the calendar year as a
collection, NOT as a charge, on the capitation line.
Note:
Report charges and collections for deductibles and co-payments that are charged to, paid by, and/or due
from patients as Self-Pay on Line 13.
Columns C1–C4: Retroactive Settlements, Receipts, or Paybacks
• Report in Columns C1–C4 retroactive settlements, receipts, and paybacks, in addition to including them in
Column B. The most common are Medicaid, Medicare, and CHIP FQHC cost report settlements and
wraparound payments. Cost report settlements are lump-sum retroactive payments or recoupments based on
the filing of a cost report. Wraparound payments are made periodically and represent the difference between
amounts reimbursed and amounts due based upon the approved FQHC visit rates.
• Include managed care pool distributions, P4P incentive payments, quality bonuses, and paybacks to FQHC
payers or HMOs.
• Report retroactive payments received from third parties from a current or prior calendar year, as appropriate,
in Column B, subtract from Column D, and also report in Columns C1–C3.
• DO NOT report accruing anticipated receipts in Columns C1–C4. Only report retroactive settlements,
receipts, or paybacks on a cash basis.
• DO NOT report wraparound payments if the State pays the FQHC rate upon billing. States that pay the FQHC
rate rather than a market rate will typically not make wraparound reconciliation payments.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
163 2023 UDS MANUAL | Instructions for Table 9D
Column C1: Collection of Reconciliation/Wraparound, Current Year
• Report FQHC cash receipts from settlements and wraparound payments from Medicare, Medicaid, or Other
Public payers that are for services provided during the current calendar year. Include the current-year
component, if any, of multi-year settlements here.
Column C2: Collection of Reconciliation/Wraparound, Previous Years
• Report FQHC cash receipts from reconciliations and wraparound payments from Medicare, Medicaid, or
Other Public payers that are for services provided during previous calendar years. Include the prior-year
component of multiyear settlements here.
A supplemental wraparound payment may be made for each visit, including managed care visits, to adjust total
payment to equal FQHC cost-based rates.
Apportion settlement data reported in Columns C1 and C2 between the fee-for-service lines and the managed
care lines when both payment reimbursement methods are used. You may use the percentage distribution of
visits, charges, or net charges as the basis for the allocation if exact amounts are unknown.
Note: Columns C1 and C2 are not reported and are grayed out on the Private payer and Self-Pay lines.
Column C3: Collection of Other Payments Including Pay for Performance, Quality Bonuses, Risk Pools,
and Incentives
• Report other cash payments, including managed care risk pool redistribution, incentives including P4P
incentives, and quality bonuses from any payer.
• Include payment for patients enrolled in the CMS primary care demonstration projects, regardless of whether
there is a visit involved.
• Report settlements that result from a court decision that requires a payer to make a settlement to the health
center, including a multiyear settlement. These payments may apply to either a managed care or non-managed
care payer.
• DO NOT report eligible provider payments from CMS for implementing EHRs (referred to as Promoting
Interoperability Programs payments). Report these payments on Table 9E, Line 3a.
Note: Column C3 is not reported and is grayed out on the Self-Pay line.
Column C4: Penalty/Payback
• Report, as a positive number, refund payments made by the health center to payers because of overpayments.
Only report amounts paid back during the calendar year.
• Report “penalty” payments made to payers due to the health center’s failure to meet utilization or other
performance goals.
• If a check was written for the payback, report the payback amount in Column C4, subtract this amount from
Column B, and add it to Column D as an adjustment. Alternatively, if the payback amount is deducted from a
remittance, report it in Column C4, but DO NOT adjust Columns B or D.
Note: Column C4 is not reported and is grayed out on the Self-Pay line.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
164 2023 UDS MANUAL | Instructions for Table 9D
Column D: Adjustments
Virtually all insurance companies have a maximum amount they pay for a given service and the health center
agrees to write off the difference between what they charge and that contracted amount. These are reported as
contractual adjustments.
• Report in Column D adjustments granted as part of an agreement with a third-party payer.
• Report adjustments as a positive number, unless as you reduce the initial adjustment by the amount of
retroactive settlements and receipts (reported in Columns C1, C2, and C3), current- and prior-year FQHC
reconciliations, managed care pool distributions, quality or P4P awards, and other payments the result is a
negative number. A negative adjustment means more was received for the service than charged.
Note: Adjustments that have the normal effect of reducing the charge are reported without brackets or a minus
sign in Column D, and those that have the effect of increasing charges are reported as a negative number.
Adjustments will not normally exceed charges.
• Capitated managed care plans (Lines 2a, 5a, 8a, and 11a only) typically pay on a per-member, per-month
basis and make payments in the current month of enrollment, which means these plans are typically the only
plans that DO NOT carry significant receivables. In these instances, report the difference between the charges
for the capitated services provided and the capitation earned during the calendar year (Column A minus
Column B) as the adjustment (Column D), unless there are early or late capitation payments.
• No adjustments can be entered on Line 13 (Self-Pay), because patient adjustments are recognized as either
sliding fee discounts (Line 13, Column E) or as self-pay bad debt (Line 13, Column F).
• If your organization records capitation receipts in the general ledger, this will require that the charges for
capitation services be eliminated from the PMS with an adjustment, as no payment is expected to be recorded
in the PMS. DO NOT report these in Column D. Only report adjustments in Column D that are the difference
between the charges for capitated services and the capitations earned. If the capitations earned were all
received during the calendar year, the adjustment will equal the difference between Column A and Column B.
If not all of the capitations earned were received during the calendar year, Column A less Column B less
Column D will equal the capitation amount due to the health center.
• DO NOT report amounts for which another third party or a patient is billed (e.g., amounts due from patients
or “Medigap” payers for co-payments) as adjustments. Transfer these charges from the primary payer to the
secondary and subsequent payers.
Note: Column D is not reported and is grayed out on the Self-Pay line.
Column E: Sliding Fee Discounts
The health center’s sliding fee discount policies and procedures determine the discounts, if any, to apply to
charges owed by patients.
• Report the amount of sliding fee discounts applied to patient charges based on the patient’s ability to pay
using patient’s income and family/household size.
• Include sliding discounts applied to co-payments and deductibles, as applicable.
• Report prompt pay discounts provided under a hardship fee waiver program as sliding fee discounts.
• DO NOT report:
o automatic discounting of charges for specific categories of patients (e.g., students, patients experiencing
homelessness, or agricultural workers) as a sliding fee discount.
o bad debt write-off or forgiveness as a sliding fee discount.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
165 2023 UDS MANUAL | Instructions for Table 9D
o other types of discounts that DO NOT meet the criteria as a sliding fee discount.
Note: Column E is grayed out on all third-party payer lines and only available on the self-pay line.
Note: When a sliding fee discount is used to write off part of a charge originally made to a third party, such as
Medicare or a private insurance company’s co-payment or deductible, first transfer or reclassify the charge to
self-pay. To transfer or reclassify, first reduce the third-party charge by the amount due from the patient and then
increase the self-pay charges by the same amount.
Column F: Bad Debt Write-Off
Bad debt write-off may occur due to the health center’s inability to locate patients, a patient’s refusal to pay, a
patient’s inability to pay for amounts not subject to a sliding fee discount, or a patient’s inability to pay even after
the sliding fee discount is granted.
• Report amounts billed to and defaulted on by any patient. Report bad debts only from patients as self-pay bad
debts.
• Report either the amount directly written off from patient accounts during the calendar year or the amount of
change in the allowance account attributable to self-pay as of the end of the calendar year.
• DO NOT report the bad debt associated with third parties, which may include charges that were not billed
within the time permitted by the payer, charges for services rendered to insured patients by providers who
were not credentialed by that payer, charges due from payers who are bankrupt, and similar bad debts. These
are not currently reported on the UDS.
Note: Column F is available only on the Self-Pay line and is grayed out on all third-party payer lines.
Total Patient Service Revenue (Line 14)
Sum of Lines 3 + 6 + 9 + 12 + 13.
FAQ FOR TABLE 9D
1. How should charges and collections for patients enrolled in an indigent care program be handled?
Report such charges as Self-Pay, Line 13, in Column A.
Report the payments, whether made on a per-visit basis or as a lump sum for services rendered, on Line 6a of
Table 9E. See Cross-Table Reporting Guidance for Indigent Programs
for specific instructions.
DO NOT report on this table payments received from state or local indigent care programs subsidizing
services rendered to patients who are uninsured.
DO NOT report anything as an indigent care program without first reviewing this with the UDS Support
Center or your UDS Reviewer.
2. Should the charges less collections less adjustments equal zero?
No, normally this is NOT equal to zero. Charges (Column A) minus collections (Column B) minus
adjustments (Columns D, E, and F) equals the change in accounts receivable or the amount by which what is
owed to the health center increases or decreases during the calendar year. Straight capitation plans (Lines 2a,
5a, 8a, and 11a) may show no change in accounts receivable assuming all capitations earned were received
during the calendar year. Combined capitation and fee-for-service managed care plans may occasionally show

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
166 2023 UDS MANUAL | Instructions for Table 9D
a change in accounts receivable on the capitation line due to pending charges, which would be for services not
covered by the capitation that have yet to be transferred to the fee-for-service managed care line.
3. If we have not received any reconciliation payments for the calendar year, what do we report in
Column C1 (current-year reconciliations)?
Only those cost report settlements and wraparound reconciliations attributable to the report calendar year are
reported in Column C1, so report zero in Column C1.
4. We often use our sliding fee discount program to write off the co-payment portion of the Medicare
charge for our certified low-income patients. The sliding fee discount column (Column E) is grayed out
for Medicare. How do we record this write-off?
It is grayed out for Medicare because the write-off is applied to the patient, not Medicare. To do this,
reclassify or transfer the amount of the co-payment from the charge column of the Medicare line (Lines 4–6,
as appropriate) to the Self-Pay line (Line 13). It can then be written off as a sliding fee discount on Line 13.
Use the same process for any other third-party payer co-payment or deductible write-off for patients who
received a sliding fee discount.
5. Our system does not automatically reclassify amounts due from other carriers or from the patient.
Must we, for example, reclassify Medicare charges that become co-payments or Medicaid charges?
Yes. Regardless of whether it is done automatically by your PMS/HIT/EHR or manually, reflect this
reclassification of charges that end up being the responsibility of a party other than the initial party. As a rule,
your system will make this adjustment in some way, but you may need to work with your vendor to get a
report on the amounts transferred or consult with the UDS Support Center or UDS Reviewer about how to do
this.
6. How do we report the charges and collections for pharmaceuticals dispensed at our contract
pharmacies?
We discuss contract pharmacy reporting at length in Appendix B
. In general, report the full charge in Column
A by payer. Report the amount received from the payer on the line corresponding to whom the payment was
received from in Column B. Report the amount that is written off for an insurance company in Column D.
Report any sliding discount amount written off for a patient as a sliding fee discount in Column E. Similar
rules apply if drugs are billable to Medicaid and Medicare.
7. How should we report the charges associated with “G-codes”?
G-codes specify a reimbursement rate associated with a service or package of services that your health center
has described to Medicare. They are NOT reported as charges or with fee schedule charges. (Similar amounts
may be paid to you by other third-party payers as well.) For UDS, report these in:
• Column A: The sum of actual fee schedule/CPT-related charges for visits
• Column B: What your health center received for payment
• Column D: The discounted amount disallowed between charges and the amount received
Remember to reduce the charges by the Medicare co-payment (20% of the allowable charge) and to reclassify
them to the secondary payer or the patient, as appropriate. See discussion of reclassifying co-payments.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
167 2023 UDS MANUAL | Instructions for Table 9D
Note: If both the actual charge and the G-code charge are routinely applied to the visit by your system, you
must remove the G-code charges by running a report to get the total for G-code charges for the year and then
subtracting this number from the total charges (actual plus G-code). Report the difference in Column A. Reduce
Column D by the G-code amount if it was adjusted using a similar process.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
168 2023 UDS MANUAL | Instructions for Table 9D
TABLE 9D: PATIENT SERVICE REVENUE
Calendar Year: January 1, 2023, through December 31, 2023
[blank for
demonstration]
[blank for demonstration]
[blank for
demonstration]
[blank for demonstration]
Retroactive S
ettlements, Receipts
, and Paybacks
(c)
[blank for demonstration]
[blank for demonstration]
[blank for
demonstration]
Line Payer Category
Full
Charges
This
Period
(a)
Amount
Collected
This
Period
(b)
Collection of
Reconciliation/
Wraparound
Current Year
(c1)
Collection of
Reconciliation/
Wraparound
Previous Years
(c2)
Collection of
Other
Payments:
P4P, Risk
Pools, etc.
(c3)
Penalty/
Payback
(c4)
Adjustments
(d)
Sliding Fee
Discounts
(e)
Bad
Debt
Write
-Off
(f)
1 Medicaid Non-Managed Care
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[not reported]
[not reported]
2a
Medicaid Managed Care
(capitated)
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[not reported]
[not reported]
2b
Medicaid Managed Care (fee-
for-service)
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[not reported]
[not reported]
3
Total Medicaid
(Sum of Lines 1 + 2a + 2b)
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[not reported]
[not reported]
4 Medicare Non-Managed Care
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[not reported]
[not reported]
5a
Medicare Managed Care
(capitated)
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[not reported]
[not reported]
5b
Medicare Managed Care (fee-
for-service)
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[not reported]
[not reported]
6
Total Medicare
(Sum of Lines 4 + 5a + 5b)
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[not reported]
[not reported]
7
Other Public, including Non-
Medicaid CHIP, Non-Managed
Care
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[not reported]
[not reported]
8a
Other Public, including Non-
Medicaid CHIP, Managed Care
(capitated)
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[not reported]
[not reported]
8b
Other Public, including Non-
Medicaid CHIP, Managed Care
(fee-for-service)
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[not reported]
[not reported]
9
Total Other Public
(Sum of Lines 7 + 8a + 8b)
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[not reported]
[not reported]

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
169 2023 UDS MANUAL | Instructions for Table 9D
[blank for
demonstration]
[blank for demonstration]
[blank for
demonstration]
[blank for demonstration]
Retroactive S
ettlements, Receipts
, and Paybacks
(c)
[blank for demonstration]
[blank for demonstration]
[blank for
demonstration]
Line Payer Category
Full
Charges
This
Period
(a)
Amount
Collected
This
Period
(b)
Collection of
Reconciliation/
Wraparound
Current Year
(c1)
Collection of
Reconciliation/
Wraparound
Previous Years
(c2)
Collection of
Other
Payments:
P4P, Risk
Pools, etc.
(c3)
Penalty/
Payback
(c4)
Adjustments
(d)
Sliding Fee
Discounts
(e)
Bad
Debt
Write
-Off
(f)
10 Private Non-Managed Care
[blank for demonstration]
[blank for demonstration]
[not reported]
[not reported]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[not reported]
[not reported]
11a
Private Managed Care
(capitated)
[blank for demonstration]
[blank for demonstration]
[not reported]
[not reported]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[not reported]
[not reported]
11b
Private Managed Care (fee-for-
service)
[blank for demonstration]
[blank for demonstration]
[not reported]
[not reported]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[not reported]
[not reported]
12
Total Private
(Sum of Lines 10 + 11a + 11b)
[blank for demonstration]
[blank for demonstration]
[not reported]
[not reported]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[not reported]
[not reported]
13 Self-Pay
[blank for demonstration]
[blank for demonstration]
[not reported]
[not reported]
[not reported]
[not reported]
[not reported]
[blank for demonstration]
[blank for
demonstration]
14
TOTAL
(Sum of Lines 3 + 6 + 9 + 12 +
13)
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for demonstration]
[blank for
demonstration]
Table 9D Cross-Table Considerations:
• Charges and collections by payer on Table 9D are related to the classification of patients by medical insurance on Table 4. See the crosswalk of
comparable fields in Appendix B
. For example, dividing Medicaid revenue on Table 9D, Line 3, Column B by Total Medicaid Patients on Table 4,
Line 8 equals the average collection per Medicaid patient.
• Other Public charges and collections on Table 9D are generally not directly comparable to Table 4 Other Public. Categorical grants such as Title X and
BCCEDP are NOT insurance and the patients are usually classified as Uninsured on Table 4, but their associated charges and collections are shown as
Other Public on Table 9D.
• Managed care revenue on Table 9D relates to member months on Table 4. Dividing managed care capitation revenue by member months equals
average capitation per member per month (PMPM). For example, dividing Medicaid capitation revenue (Table 9D, Line 2a, Column B − (c1 + c2 + c3
− c4)) by Table 4, Line 13a, Column A equals Medicaid PMPM.
• Billable visits reported on Table 5 should relate to patient charges reported on Table 9D.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
170 2023 UDS MANUAL | Instructions for Table 9E
Instructions for Table 9E: Other Revenue
Table 9E reports revenue-related non–patient service receipts, including grants, contracts, and other funds
received in the calendar year from sources supporting the scope of project. This table includes all revenue
received that are not directly tied to the delivery of a specific patient service.
Several notable changes have been made to Table 9E, as outlined below:
• Supplemental funding for Expanding COVID-19 Vaccination (ECV) has been added as Line 1p.
TABLE 9E: OTHER REVENUE
This table provides information about the health center program’s receipt of funds used to support in-scope
activities not reported on Table 9D.
• Report all non–patient service-related funds received during the calendar year that supported the federally
approved scope of project.
• Use the “last party rule” to classify the receipts. The “last party rule,” for UDS reporting purposes, means
that grant, contract, and other funds should always be reported based on the entity from which the health
center received them, regardless of the source from which they originated.
• DO NOT report any receipts on both Tables 9D and 9E, as this will duplicate the cash revenue received.
Note:
Tables 9D and 9E receipts are summed to equal total cash revenue received during the calendar year.
BPHC GRANTS
Health Center Program Grants, Lines 1a Through 1e
• Report drawdowns received during the calendar year for the Health Center Program (section 330) grant,
including:
o Amounts consistent with the Payment Management System (PMS)-272
federal cash transaction report.
Report grant drawdowns as follows:
MHC on Line 1a
CHC on Line 1b
HCH on Line 1c
PHPC on Line 1e
o Supplemental funding (with the exception of COVID-19) from HRSA is provided as part of the 330
grant. Report these grant funds on the appropriate 330 grant Lines 1a–1e, as specified in the health center
Notice of Award.
o Direct funding, including NAP or expansion funds, is reported only on these lines.
o Include amounts that the health center received and passed through to another Health Center Program
awardee.
• DO NOT reduce the drawdown by the amount the health center passed through to another health center,
including sub-awardees or sub-recipients.
• If you are a look-alike or BHW primary care clinic, DO NOT report grant receipts from the BPHC Health
Center Program on these lines. The fields are grayed out in the EHBs.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
171 2023 UDS MANUAL | Instructions for Table 9E
Total Health Center Program (Line 1g)
Sum of Lines 1a through 1e.
Capital Development Grants (Line 1k)
• Report the amount of BPHC Capital Development Grant dollars drawn down.
• Include funds from the Health Center Program facility program, as well as funds from the HRSA-
administered school-based service site capital grant program.
• Report Capital Assistance for Hurricane Response and Recovery Efforts (CARE), Capital Assistance for
Disaster Response and Recovery Efforts (CADRE), and other funds awarded by HRSA to assist in the
reconstruction and repair of facilities destroyed or damaged by natural disasters.
COVID-19 Supplemental Funding
Lines 1l through 1p2
• Report drawdowns received during the calendar year for COVID-19 supplemental funding, consistent with
the PMS-272 federal cash transaction report. Report grant drawdowns as follows:
o Coronavirus Preparedness and Response Supplemental Appropriations Act (activity code H8C) (Line 1l)
o Coronavirus Aid, Relief, and Economic Security (CARES) Act (activity code H8D) (Line 1m)
o Expanding Capacity for Coronavirus Testing (activity code H8E and ECT) (Line 1n)
o American Rescue Plan (ARP), including ARP capital improvement grants (activity code H8F, L2C, and
C8E) (Line 1o)
o Expanding COVID-19 Vaccination (ECV) (activity code ECV) (Line 1p)
o Other COVID-19-related funding drawn down from BPHC grants (Line 1p2). Use the “specify” field to
detail the names and amounts of other COVID-19-related funding from HRSA.
Total COVID-19 Supplemental (Line 1q)
Sum of Lines 1l through 1p2.
Total BPHC Grants (Line 1)
Sum of Lines 1g + 1k + 1q.
OTHER FEDERAL GRANTS
Ryan White Part C—HIV Early Intervention Grants (Line 2)
• Report drawdowns received during the calendar year for Ryan White Part C cash receipts.
• Guidance for reporting funds from other Ryan White titles is provided in the FAQ for Table 9E
.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
172 2023 UDS MANUAL | Instructions for Table 9E
Other Federal Grants (Line 3)
Federal grants include only those funds received directly by the health center from the U.S. Treasury for which
there is a Notice of Federal Award. Examples of common “other federal” grants reported are from the Office of
Minority Health (OMH), the Indian Health Service (IHS), the Department of Housing and Urban Development
(HUD), Federal Communications Commission (FCC), and the Substance Abuse and Mental Health Services
Administration (SAMHSA).
• Report drawdowns received during the calendar year for any other federal grants that are within the scope of
project. Use the “specify” field to detail the names and amounts of other federal grants.
• Include IHS funds (not including PL 93-638 Compact funds
) if your health center is dually funded as an
IHS/HRSA-funded health center. Report PL 93-638 Compact funds on Line 6a, Indigent Care.
• Include ARP funds drawn down from other HRSA bureaus (not BPHC or Ryan White Part C) or from other
federal agencies.
Medicare and Medicaid EHR Incentive Grants for Eligible Providers (Line 3a)
CMS provides incentives to Eligible Providers (as defined by CMS) for the adoption, implementation, upgrading,
and improvement of interoperability of certified EHRs.
• Report grants funded through CMS from the Medicare and Medicaid EHR Incentive Program (now known as
“Promoting Interoperability Programs”).
• In rare cases, these payments go directly to the health center’s providers, but they are usually paid to the
providers’ designee (generally, the health center). It is presumed that if the payment goes to the providers
these funds will be turned over to the health center. Report them on this line even though the payment may
come from the provider and not directly from CMS. This is an exception to the “last party” rule. In the event
the provider retains some or all of these incentives as part of their compensation, report the total amount on
this line and the amount retained by the provider on Table 8A, Line 1, as personnel compensation.
Provider Relief Fund (Line 3b)
• Report funds from the CARES Act Provider Relief Fund through HHS. These funds provide relief to eligible
providers for health care–related expenses or lost revenues that are attributable to the novel coronavirus.
Total Other Federal Grants (Line 5)
Sum of Lines 2 + 3 + 3a + 3b.
NON-FEDERAL GRANTS OR CONTRACTS
State Government Grants and Contracts (Line 6)
• Report cash received during the calendar year for any state government grants or contracts that are within the
health center scope of project and for which the health center receives the funds with no specific tie to
services provided. Use the “specify” field to detail the names and amounts of state government grants and
contracts.
• Most include line-item budgets that support specific personnel positions or other costs.
• DO NOT report receipts from state governments that pay based on the amount of health care services
provided or on a negotiated fee-for-service or fee-per-visit. Report charges, collections, and adjustments on
Table 9D on the Other Public revenue lines.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
173 2023 UDS MANUAL | Instructions for Table 9E
State/Local Indigent Care Programs (Line 6a)
• Report the amount of funds received from state/local indigent care programs that are earmarked to subsidize
services rendered to patients who are uninsured. Use the “specify” field to detail the names and amounts of
state/local indigent care programs.
• Include amounts allocated to the health center by tribes from their IHS PL 93-638 Compact funds.
• DO NOT include revenue received under a contract with a tribal government for services provided to its
members. Report as Other Public with charges, collections, and adjustments on Table 9D.
• Further guidance is available in Appendix B
.
Local Government Grants and Contracts (Line 7)
• Report cash received during the calendar year for any local government grants or contracts that are within the
scope of project and for which there is no specific tie to patient services provided. Use the “specify” field to
detail the names and amounts of local government grants and contracts.
• Most include line-item budgets that support specific personnel positions or other costs.
• DO NOT include revenue received from local governments that pay based on amount of health care services
provided or on a negotiated fee-for-service or fee-per-visit basis. Report charges, collections, and adjustments
on Table 9D on the Other Public revenue lines.
• DO NOT include funds from local indigent care programs here. Report these on Line 6a.
Foundation/Private Grants and Contracts (Line 8)
• Report the amount received from foundations or private organizations during the calendar year that covers
costs included within the scope of project. Use the “specify” field to detail the names and amounts of
foundation/private grants and contracts.
• Include funds (including subaward funds) received directly from a primary care association (PCA), another
health center, or another community service provider on this line, even when funds originate elsewhere.
Total Non-Federal Grants and Contracts (Line 9)
Sum of Lines 6 + 6a + 7 + 8.
Other Revenue (Line 10)
• Report other revenue receipts included in the federally approved scope of project that are unrelated to charge-
based services or to grants and contracts described above. Use the “specify” field to detail the names and
amounts of other revenue.
• Include fundraising, interest revenue, rent from tenants, patient health records fees, individual monetary
donations, receipts from vending machines, retail pharmacy sales to the public (i.e., non–health center
patients), etc.
• Include receipts related to the gain on the sale of an asset.
• DO NOT report:
o the value of in-kind or other non-monetary donations made to the health center. Report these only on
Table 8A, Line 18.
o the proceeds of any loan received for operations, a mortgage, or other purposes.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
174 2023 UDS MANUAL | Instructions for Table 9E
o the value of loans forgiven by the lender.
o insurance proceeds related to a loss, unless the loss was recognized as an expense rather than a reduction
in the value of an asset.
o the receipt or recognition of in-kind “community benefit” from a third party here or anywhere else on the
UDS unless it is received as a cash donation.
o under any circumstances, payments or net payments from a pharmacy contracted to dispense 340B
pharmaceuticals on this line (or anywhere on Table 9E). Report all revenue from pharmacy services
provided to health center patients on Table 9D and record all expenses on Table 8A.
Total Other Revenue (Line 11)
Sum of Lines 1 + 5 + 9 + 10.
FAQ FOR TABLE 9E
1. We received maternal and child health services funds from the state that originated from the federal
government. On which line do we report these funds?
Use the “last party rule” to report on this table. In this instance, report these funds as state grants on Line 6,
since the funds were awarded to the health center by the state for maternal and child health services, even
though these may include a mixture of federal funds (such as Title V) and state funds.
2. We receive various Ryan White–related funds. How do we report these?
This depends on which entity you received Ryan White funds from. Use the following to guide your
reporting:
• Report Ryan White Part A, Impacted Area grants, from county or city governments on Line 7. If they are
first sent to a third party, report the funds on Line 8. Report on Line 3 when the reporting entity is a
county or city government, and the funds were received directly from the Ryan White Part A federal
program.
• Report Part B grants from the state on Line 6, unless they are first sent to a county or city government (in
which case, report on Line 7) or to a third party (in which case, report the funds on Line 8).
• Report drawdowns received during the calendar year for Ryan White Part C on Line 2.
• Report Part D funds from the HIV/AIDS Bureau on Line 3.
• Report Part F funds, Special Projects of National Significance (SPNS) grants, received from the
HIV/AIDS Bureau on Line 3.
3. Are there any important issues to keep in mind for this table?
This table collects information on cash receipts for the calendar year that supported activities described in the
scope of project covered by any of the Health Center Program awards, the look-alike designation, or the BHW
primary care clinics program.
In the case of a grant:
• Report the cash amount received during the calendar year.
• DO NOT report the award amount (unless the full award was paid/drawn down during the year).

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
175 2023 UDS MANUAL | Instructions for Table 9E
4. How should we report indigent care funds?
• Report payments received from state or local indigent care programs subsidizing services rendered to
patients who are uninsured (including patients covered by a tribe’s 638 funds) on Line 6a of Table 9E,
whether the actual payment to the health center is made on a per-visit basis or as a lump sum for services
rendered.
• Report patients who received care during the year covered by these programs as Uninsured on Table 4.
• Report all charges, self-pay patient collections, sliding fee discounts, and bad debt write-offs on the Self-
Pay line (Line 13) on Table 9D.
• Report amounts collected from the patients covered by indigent programs on Table 9D, Line 13, Column
B. However, DO NOT report funds reported on Line 6a of Table 9E on Table 9D as collections, sliding
discounts, or bad debt.
UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
176 2023 UDS MANUAL | Instructions for Table 9E
TABLE 9E: OTHER REVENUES
Calendar Year: January 1, 2023, through December 31, 2023
Line Source
Amount
(a)
[blank]
BPHC Grants (Enter Amount Drawn Down—Consistent with PMS 272)
[blank]
1a
Migrant Health Center
[blank]
1b
Community Health Center
[blank]
1c
Health Care for the Homeless
[blank]
1e
Public Housing Primary Care
[blank]
1g
Total Health Center (Sum of Lines 1a through 1e)
[blank]
1k
Capital Development Grants, including School-Based Service Site Capital Grants
[blank]
1l
Coronavirus Preparedness and Response Supplemental Appropriations Act (H8C)
[blank]
1m
Coronavirus Aid, Relief, and Economic Security Act (CARES) (H8D)
[blank]
1n
Expanding Capacity for Coronavirus Testing (ECT) (H8E and LAL ECT)
[blank]
1o
American Rescue Plan (ARP) (H8F, L2C, C8E)
[blank]
1p
Expanding COVID-19 Vaccination (ECV)
[blank]
1p2
Other COVID-19-Related Funding from BPHC (specify _______)
1q
Total COVID-19 Supplemental (Sum of Lines 1l through 1p2)
[blank]
1
Total BPHC Grants
(Sum of Lines 1g + 1k + 1q)
[blank]
[blank]
Other Federal Grants
[blank]
2
Ryan White Part C HIV Early Intervention
[blank]
3
Other Federal Grants (specify _______)
[blank]
3a
Medicare and Medicaid EHR Incentive Payments for Eligible Providers
[blank]
3b
Provider Relief Fund (specify _______)
[{blank]
5
Total Other Federal Grants
(Sum of Lines 2 through 3b)
[blank]
[blank]
Non-Federal Grants or Contracts
[blank]
6
State Government Grants and Contracts (specify_______)
[blank]
6a
State/Local Indigent Care Programs (specify_______)
[blank]
7
Local Government Grants and Contracts (specify_______)
[blank]
8
Foundation/Private Grants and Contracts (specify_______)
[blank]
9
Total Non-Federal Grants and Contracts
(Sum of Lines 6 + 6a + 7 + 8)
[blank]
10
Other Revenue (non–patient service revenue not reported elsewhere) (specify ______)
[blank]
11
Total Revenue (Sum of Lines 1 + 5 + 9 + 10)
[blank]
Table 9E Cross-Table Considerations:
• Pharmacy: Only retail, public pharmacy revenue for non–health center patients is reported on Table 9E, Line
10, and the related cost is reported on Table 8A, Line 12. Follow the guidance for other pharmacy reporting
situations as described in Appendix B
.
• The revenue received from indigent care programs that subsidize services rendered to patients who are
uninsured are reported on Table 9E, while the charges for these services are reported on Table 9D. Follow the
detailed reporting requirements included in Appendix B
to address the cross-table reporting.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
177 2023 UDS MANUAL | Appendix A
Appendix A: Listing of Personnel
All line numbers in the following table refer to Table 5. NOT all services delivered by a “provider” count as
visits. DO NOT count encounters with “non-providers” as countable visits. Use the Provider
definitions to
classify personnel as a “provider” or “non-provider.”
Personnel by Major Service Category
Provider
Non-Provider
Physicians
<blank>
<blank>
Family practitioners (Line 1)
X
<blank>
General practitioners (Line 2)
X
<blank>
Internists (Line 3)
X
<blank>
Obstetricians/Gynecologists (Line 4)
X
<blank>
Pediatricians (Line 5)
X
<blank>
Licensed medical residents—line determined by specialty
X
<blank>
Other Specialist Physicians (Line 7)
<blank>
<blank>
Allergists
X
<blank>
Cardiologists
X
<blank>
Dermatologists
X
<blank>
Endocrinologists
X
<blank>
Orthopedists
X
<blank>
Surgeons
X
<blank>
Urologists
X
<blank>
Other specialists and sub-specialists
X
<blank>
Nurse Practitioners, Physician Assistants, and Certified Nurse Midwives
<blank>
<blank>
Nurse practitioners (Line 9a)
X
<blank>
Physician assistants (Line 9b)
X
<blank>
Certified nurse midwives (Line 10)
X
<blank>
Nurses (Line 11)
<blank>
<blank>
Clinical nurse specialists
X
<blank>
Public health nurses
X
<blank>
Home health nurses
X
<blank>
Visiting nurses
X
<blank>
Registered nurses (RNs)
X
<blank>
Licensed practical nurses/Licensed vocational nurses
<blank>
X
Nurse emergency medical services (EMS)/Nurse emergency medical technicians
(EMT)
X blank
Other Medical Personnel (Line 12)
<blank>
<blank>
Nurse aides/assistants (certified and uncertified)
<blank>
X
Clinic aides/medical assistants (certified and uncertified medical technologists)
<blank>
X
Unlicensed interns and residents
<blank>
X
EMS/EMT personnel (not credentialed as a nurse)
<blank>
X
Laboratory Personnel (Line 13)
<blank>
<blank>
Pathologists
<blank>
X
Medical technologists
<blank>
X
Laboratory technicians
<blank>
X
Laboratory assistants
<blank>
X
Phlebotomists
<blank>
X
X-Ray Personnel (Line 14)
<blank>
<blank>
Radiologists
<blank>
X
X-ray technologists
<blank>
X
X-ray technicians
<blank>
X
Radiology assistants
<blank>
X
Ultrasound technicians
<blank>
X

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
178 2023 UDS MANUAL | Appendix A
Personnel by Major Service Category
Provider
Non-Provider
Dentists (Line 16)
<blank>
<blank>
General practitioners
X
<blank>
Oral surgeons
X
<blank>
Periodontists
X
<blank>
Endodontists
X
<blank>
Dental Hygienists (Line 17)
<blank>
<blank>
Dental hygienists
X
<blank>
Dental Therapists (Line 17a)
<blank>
<blank>
Dental therapists
X
<blank>
Other Dental Personnel (Line 18)
<blank>
<blank>
Dental assistants, advanced practice dental assistants
<blank>
X
Dental technicians
<blank>
X
Dental aides
<blank>
X
Dental students (including hygienist students)
<blank>
X
Mental Health (Line 20) and Substance Use (Line 21)
<blank>
<blank>
Psychiatrists (Line 20a)
X
<blank>
Psychologists (Line 20a1)
X
<blank>
Social workers—clinical (Line 20a2 or 21)
X
<blank>
Social workers—psychiatric (Line 20b or 21)
X
<blank>
Family therapists (Line 20b or 21)
X
<blank>
Psychiatric nurse practitioners (Line 20b)
X
<blank>
Nurses—psychiatric and mental health (Line 20b)
X
<blank>
Unlicensed mental health providers, including trainees (interns or residents) and
“certified” personnel (Line 20c)
X <blank>
Unlicensed substance use disorder providers, including trainees (interns or
residents) and “certified” personnel (Line 21)
X <blank>
Alcohol and drug abuse counselors (Line 21)
X
<blank>
RN counselors (Line 20b or 21)
X
<blank>
Peer recovery coaches and workers (Line 21)
X
<blank>
Other Professional Health Services Personnel (Line 22)
<blank>
Audiologists
X
<blank>
Acupuncturists
X
<blank>
Chiropractors
X
<blank>
Community and behavioral health aides and practitioners
X
<blank>
Herbalists
X
<blank>
Massage therapists
X
<blank>
Naturopaths
X
<blank>
Registered dietitians, including nutritionists/dietitians
X
<blank>
Occupational therapists
X
<blank>
Podiatrists
X
<blank>
Physical therapists
X
<blank>
Respiratory therapists
X
<blank>
Speech therapists/pathologists
X
<blank>
Traditional healers
X
<blank>
Vision Services Personnel
<blank>
<blank>
Ophthalmologists (Line 22a)
X
<blank>
Optometrists (Line 22b)
X
<blank>
Ophthalmologist/optometric assistants (Line 22c)
<blank>
X
Ophthalmologist/optometric aides (Line 22c)
<blank>
X
Ophthalmologist/optometric technicians (Line 22c)
<blank>
X

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
179 2023 UDS MANUAL | Appendix A
Personnel by Major Service Category
Provider
Non-Provider
Pharmacy Personnel
<blank>
<blank>
Pharmacists (Line 23a)
<blank>
X
Clinical pharmacists (Line 23b)
X
Pharmacy technicians (Line 23c)
<blank>
X
Pharmacist assistants (Line 23d)
<blank>
X
Pharmacy clerks (Line 23d)
<blank>
X
Case Managers (Line 24)
<blank>
<blank>
Case managers
X
<blank>
Care/referral coordinators
X
<blank>
Patient advocates
X
<blank>
Social workers
X
<blank>
Public health nurses
X
<blank>
Home health nurses
X
<blank>
Visiting nurses
X
<blank>
Registered nurses
X
<blank>
Licensed practical nurses/licensed vocational nurses
X
<blank>
Health Education Specialists (Line 25)
<blank>
<blank>
Family planning counselors
X
<blank>
Patient health educators/specialists
X
<blank>
Social workers
X
<blank>
Public health nurses
X
<blank>
Home health nurses
X
<blank>
Visiting nurses
X
<blank>
Registered nurses
X
<blank>
Licensed practical nurses/licensed vocational nurses
X
<blank>
Community and group educators/specialists
<blank>
X
Outreach Workers (Line 26)
<blank>
<blank>
Outreach workers
<blank>
X
Transportation Workers (Line 27)
<blank>
<blank>
Patient transportation coordinators
<blank>
X
Drivers, including mobile van drivers
<blank>
X
Eligibility Assistance Workers (Line 27a)
<blank>
<blank>
Benefits assistance workers
<blank>
X
Pharmacy assistance program (PAP) eligibility workers
<blank>
X
Eligibility workers
<blank>
X
Patient navigators
<blank>
X
Patient advocates
<blank>
X
Registration clerks
<blank>
X
Certified assisters
<blank>
X
Interpretation Personnel (Line 27b)
<blank>
<blank>
Interpreters
<blank>
X
Translators
<blank>
X
Community Health Workers (Line 27c)
<blank>
<blank>
Community health workers
<blank>
X
Community health advisors or representatives
<blank>
X
Lay health advocates
<blank>
X
Peer health promoters/educators
<blank>
X
Promotoras
<blank>
X
Personnel Performing Other Enabling Services Activities (Line 28)
<blank>
<blank>
Other enabling services personnel
<blank>
X
UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
180 2023 UDS MANUAL | Appendix A
Personnel by Major Service Category
Provider
Non-Provider
Other Programs and Related Services Personnel (Line 29a)
<blank>
<blank>
WIC workers
<blank>
X
Head Start workers
<blank>
X
Housing assistance workers
<blank>
X
Child care workers
<blank>
X
Food bank/meal delivery workers
<blank>
X
Employment/educational counselors
<blank>
X
Exercise trainers/fitness center personnel
<blank>
X
Adult day health care, frail elderly support personnel
<blank>
X
Quality Improvement Personnel (QI) (Line 29b)
<blank>
<blank>
QI nurses
<blank>
X
QI technicians
<blank>
X
QI data specialists
<blank>
X
Statisticians, analysts
<blank>
X
Quality assurance/quality improvement and HIT/EHR design and operation
personnel
<blank> X
Management and Support Personnel (Line 30a)
<blank>
<blank>
Project directors
<blank>
X
Chief executive officers/executive directors
<blank>
X
Chief financial officers/fiscal officers
<blank>
X
Chief information officers
<blank>
X
Chief medical officers
<blank>
X
Secretaries/administrative assistants
<blank>
X
Administrators
<blank>
X
Directors of planning and evaluation
<blank>
X
Clerk typists
<blank>
X
Personnel directors
<blank>
X
Receptionists
<blank>
X
Directors of marketing
<blank>
X
Marketing representatives
<blank>
X
Enrollment/service representatives
<blank>
X
Fiscal and Billing Personnel (Line 30b)
<blank>
<blank>
Finance directors
<blank>
X
Accountants
<blank>
X
Bookkeepers
<blank>
X
Billing clerks
<blank>
X
Cashiers
<blank>
X
Data entry clerks
<blank>
X
IT Personnel (Line 30c)
<blank>
<blank>
Directors of data processing
<blank>
X
Programmers
<blank>
X
IT help desk technicians
<blank>
X
Data entry clerks
<blank>
X
Facility Personnel (Line 31)
<blank>
<blank>
Janitors/custodians
<blank>
X
Security guards
<blank>
X
Groundskeepers
<blank>
X
Equipment maintenance personnel
<blank>
X
Housekeeping personnel
<blank>
X

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
181 2023 UDS MANUAL | Appendix A
Personnel by Major Service Category
Provider
Non-Provider
Patient Services Support Personnel (Line 32)
<blank>
<blank>
Medical and dental team clerks
<blank>
X
Medical and dental team secretaries
<blank>
X
Medical and dental appointment clerks
<blank>
X
Medical and dental patient health records clerks
<blank>
X
Patient health records supervisors
<blank>
X
Patient health records technicians
<blank>
X
Patient health records clerks
<blank>
X
Patient health records transcriptionists
<blank>
X
Registration clerks
<blank>
X
Appointments clerks
<blank>
X

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
182 2023 UDS MANUAL | Appendix B
Appendix B: Special Multi-Table Situations
Several conditions require special consideration in the UDS because they affect multiple tables that must then be
reconciled. This appendix presents some situations along with instructions on how to deal with them, including:
• Contracted care (specialty, dental, mental health, etc.) that is paid for by the reporting health center
• Services provided by a volunteer provider
• Interns and residents
• WIC
• In-house pharmacy or dispensary services for health center patients
• In-house pharmacy for community (i.e., for non-patients)
• Contract pharmacies
• Donated drugs
• Clinical dispensing of drugs
• ADHC/PACE
• Medi-Medi crossovers
• Certain grant-supported clinical care programs (BCCEDP, Title X, etc.)
• State or local indigent care programs
• Workers’ compensation
• Tricare, Trigon, Public Employees Insurance, etc.
• Contract sites
• CHIP
• Carved-out services
• Incarcerated patients
• HIT/EHR personnel and costs
• Migrant voucher programs and other voucher programs
• New start or New Access Point
• Relationship between personnel on Table 5 and costs on Table 8A
• Relationship between insurance on Table 4 and revenue on Table 9D
• Relationship between prenatal care on Table 6B and deliveries on Table 7
• Relationship between race and ethnicity on Table 3B and Table 7

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
183 2023 UDS MANUAL | Appendix B
CONTRACTED CARE (SPECIALTY, DENTAL, MENTAL HEALTH, ETC.)
Contracted care is services paid for by the health center.
Tables
Affected
Treatment
5
Report providers (Column A) if the contract is for a portion of an FTE (e.g., one-day-a-week OB/GYN =
0.20 FTE).
Always report visits (Column B or B2), regardless of method of provider payment or location of service
(health center’s service delivery site or contract provider’s office). Services provided by contractors and paid
for by or billed through the health center must meet the UDS countable visit definition in order to be counted
on Table 5.
DO NOT report FTE if the contract is for a service (e.g., $X per visit or $55 per resource-based relative value
unit [RBRVU]), rather than provider time.
DO NOT report FTE or visits if the contracted provider directly bills a third-party payer for the service.
6A
Report diagnoses and/or services provided, as applicable, from the encounter form or equivalent form
received from the contract provider. Include contracted tests or procedures on Table 6A only if the listed
services provided to patients are paid for by the health center or if their results are returned to the health
center provider to evaluate and provide results to the patient.
6B, 7
If a contract provider provides any services that are subject to clinical quality measures, collect and report all
data from the contractor (e.g., last HbA1c from an endocrinologist, sealants placed from a dentist).
8A
Column A, Accrued Cost: Report the cost of a provider/service on the applicable line.
DO NOT report a “co-payment” or a “nominal fee” received by the provider from the patient. Report only
the sum of what the health center pays.
Column B, Facility and Non-Clinical Support Services: The health center will generally use a lower facility
and non-clinical support services allocation rate for off-site services. Include all facility and non-clinical
support costs in the direct charge (Column A) if the provider is off-site.
9D
Column A, Charge: The health center’s UCR charge if on-site; use the contractor’s UCR charge if off-site.
Column B, Collection: The amount received by the health center and contractor from first and third parties.
Column D, Adjustment: The amount disallowed by a third party for the charge (if on Lines 1–12).
Column E, Sliding Fee Discount: The amount written off for eligible patients per the health center’s fiscal
policies (Line 13), if applicable. Calculate as UCR charge, minus amount collected from patients, minus
amount owed by patients as their share of payment. DO NOT include payment by the health center here.
UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
SERVICES PROVIDED BY A VOLUNTEER PROVIDER
Vol
unteers are not paid by the health center (although they may be paid by a third party) for services, which they
provide on-site. This includes volunteer personnel (including AmeriCorps/HealthCorps, but not NHSC) who
provide services on- or off-site on behalf of the health center. FTE can be included in the UDS Report when there
is a basis for determining their hours.
Tables
Affected
Treatment
5
Column A, FTE: Report FTE for services provided by volunteers on-site at the health center’s service
delivery site. FTE must be calculated. Use hours volunteered as the numerator. Because volunteers DO NOT
receive paid leave benefits, the denominator is the number of hours that comparable personnel spend
performing their job. Reduce a full-time schedule of 2,080 hours (for example) by vacation, sick leave,
holidays, and continuing education normally provided to personnel. As a rule of thumb, use hours worked
divided by a number somewhere around 1,800.
DO NOT report providers who provide services at their own offices.
Column B, Clinic Visits, and Column B2, Virtual Visits: Count visits for services provided at a service
delivery site in the health center’s scope of project and under its control. Include virtual visits when the
volunteer provider is assigned to an approved service delivery location, providing services to health center
patients, and documenting services in the health center’s HIT/EHR.
6A
Report diagnoses and/or services provided on-site or virtually.
8A
Column C, Line 18: Report the value of the time donated by volunteers on this line only.
9D
The charges for their services are treated the same as for paid personnel.
DO NOT include charges for volunteer providers who are off-site when those services are outside the scope
of project and/or the control of the health center.
INTERNS AND RESIDENTS
Healt
h centers often use individuals who are in training, referred to variously as interns or residents depending on
their field and their licensing. Medical residents are generally licensed practitioners, while medical interns are
generally NOT licensed. Some mental health interns, as well as other providers, may be licensed practitioners
who are training for a higher level of certification or licensing.
Tables
Affected
Treatment
5
Column A: Report licensed interns and residents in the credentialing category they are pursuing. For
example, count a family practice resident on Line 1 as a Family Physician. Depending on the arrangement,
FTEs may be calculated like any other personnel (if they are being paid by the health center) or like a
volunteer (if they are not being paid). See volunteer providers above.
Columns B and B2: Report visits between a medical resident or intern and a patient as visits to that resident
or intern. DO NOT credit the visits to the supervisor of the resident or intern, unless an intern is unlicensed
and the supervisor is legally responsible for the visit.
8A
If the intern or resident is paid by the health center or their cost is being paid through a contract that pays a
third party for the interns or residents, report the cost in Column A on the appropriate line (Line 1 for
medical, Line 5 for dental, etc.).
If the health center is not paying an intern, resident, or third party, report the value of the donated time on
Line 18. Be sure to describe the nature of the donation on the table.
184 2023 UDS MANUAL | Appendix B
UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
185 2023 UDS MANUAL | Appendix B
WOMEN, INFANTS, AND CHILDREN (WIC)
Tables
Affected
Treatment
ZIP Code,
3A, 3B, 4
DO NOT report individuals whose only encounter with the health center is for WIC services (e.g., nutrition,
health education, enabling services) and who receive no other services listed on Table 5 from providers
outside of WIC.
5
Report FTE of personnel (Column A) on Line 29a.
DO NOT report visits and patients (Columns B, B2, and C).
8A
Column A, Accrued Cost: Report the total net accrued cost of the program on Line 12 in Column A.
Column B, Allocation of Facility and Non-Clinical Support Services: Since much of the non-clinical support
services cost of the program will be included in the direct costs, it is presumed that overhead will be at a
significantly lower rate.
9D
DO NOT report anything associated with the WIC program.
9E
Revenue for WIC programs, though originally federal, generally comes to health centers from the state,
though some receive it from a lower-level intermediary. If the health center is receiving WIC funds from a
state government, the grant/contract funds received go on Line 6. If the health center is receiving WIC funds
from an intermediary, report the funds on Line 8. Specify the source of funds.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
186 2023 UDS MANUAL | Appendix B
IN-HOUSE PHARMACY OR DISPENSARY SERVICES FOR HEALTH CENTER PATIENTS
Include only that part of the pharmacy that is paid by the health center and dispensed by in-house personnel (see
below for other situations).
Tables
Affected
Treatment
5
Column A, FTE: Report pharmacy personnel according to their role on Lines 23a–23d. If they have only an
incidental responsibility to provide assistance in enrolling patients in PAPs, include them on the
corresponding pharmacy Line 23a–23d. Include clinical pharmacists on Line 23b even if they spend time
outside of the pharmacy. Report personnel other than pharmacists who spend time with PAPs on Line 27a,
Eligibility Assistance.
Columns B and B2, Visits: The UDS does NOT count encounters with pharmacy personnel as visits, whether
it is for filling prescriptions or associated education or other patient/provider support. This is true for clinical
pharmacists with expanded clinical privileges, as well. DO NOT count the administration or dispensing of
medications as visits.
8A
Line 8a, Column A, Other Pharmacy Direct (Accrued) Costs: Report all operating costs of the pharmacy,
other than the cost of drugs, on Line 8a. Include salaries, benefits, pharmacy computers, supplies, etc.
Line 8b, Column A, Pharmaceutical Direct (Accrued) Costs: Place the actual cost of drugs the health center
pharmacy bought on Line 8b. Include the cost of vaccines, contraceptives, injectable antibiotics, and other
drugs dispensed in the health center but NOT in a pharmacy on Line 8b. The value of donated drugs is not
reported here. That amount is reported on Line 18 in Column C.
Line 11e, Column A, Eligibility Assistance Direct (Accrued) Costs: Report on Line 11e the cost of personnel
(full-time, part-time, or allocated time) helping patients become eligible for PAPs and of all related supplies,
equipment depreciation, etc.
Column B, Facility and Non-Clinical Support Services: Report all facility and non-clinical support services
costs associated with pharmacy and pharmaceuticals (Lines 8a and 8b) on Line 8a. Although there may be
some facility and non-clinical support services costs associated with the actual purchase of the drugs, these
costs are generally minimal when compared to the total cost of the drugs.
Column C, Line 18: Report the value of donated drugs, including vaccines (generally calculated at 340B
rates) and test kits, on this line only.
9D
Column A: Charge is the health center’s full retail charge for dispensed drugs.
Column B: Collection is the amount received from patients and/or other third parties/insurance companies.
Column D: Adjustment is the amount a third party disallows for the charge (if on Lines 1–12).
Column E: Sliding fee discount is the amount written off for eligible patients per health center policies (on
Line 13). Calculate as retail charge, minus amount collected (if any) from patients or third-party payers,
minus amount owed by patients (if any), as their share of payment.
9E
DO NOT report the value of donated drugs on this table; report on Table 8A, Line 18 (see next page,
Donated Drugs, Including Vaccines). The charges for drugs dispensed to patients go on Table 9D, NOT on
this table.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
187 2023 UDS MANUAL | Appendix B
IN-HOUSE PHARMACY FOR COMMUNITY (I.E., FOR NON-PATIENTS)
Many health centers that own licensed pharmacies also provide services to members of the community at large
who are not health center patients. Careful records must be maintained at these pharmacies to ensure that non-
patients DO NOT receive drugs purchased under section 340B provisions. Some of these pharmacies are totally in
scope, while others have their “public” portion out of scope. If the public aspect is out of scope, DO NOT report
its activities on the UDS. If it is in scope, treat the public portion as an “other activity,” as follows:
Tables
Affected
Treatment
ZIP Code,
3A, 3B, 4
DO NOT include in the patient profile tables community members (non-patients) provided pharmaceuticals.
5
Column A, FTE: Allocate and report a portion of personnel who serve the public on Line 29a: Other
Programs and Services.
8A
Line 12: Other Program-Related Services: Report all related personnel and pharmacy costs, including cost of
pharmaceuticals.
9E
Line 10, Other Revenue: Report all revenue from public pharmacy and specify from “Public access
pharmacy.”
CONTRACT PHARMACY DISPENSING TO HEALTH CENTER PATIENTS, GENERALLY USING
340B PURCHASED DRUGS
Tables
Affected
Treatment
5 DO NOT report personnel, visits, or patients for pharmacy dispensing.
8A
Report the amount the pharmacy charges for managing dispensing of drugs on Line 8a.
Report the full amount paid for pharmaceuticals, either directly by the clinic or indirectly by the pharmacy,
on Line 8b.
If the pharmacy buys prepackaged drugs and there is no reasonable way to separate the pharmaceutical costs
from the dispensing/administrative costs, report all costs on Line 8b. Associated non-clinical support services
(overhead) costs will go on Line 8a in Column B, even if Line 8a Column A is blank.
Report payments to pharmacy benefit managers on Line 8a.
Share of profits and other fees: Some pharmacies engage in fee splitting and keep a share of profit. Report
this as a payment to the pharmacy on Line 8a.
9D
Column A, Charge: Report the health center/contract pharmacy’s full retail charge for the drugs dispensed. If
retail is unknown, ask the pharmacy for retail prices for the drugs dispensed.
Column B, Collection: Report the amount received by the contract pharmacy from patients or insurance
companies. Health centers must collect this information from the contract pharmacy. (Note: Most health
centers DO NOT have this sort of arrangement for Medicaid patients, unless explicitly stated.)
Column D, Adjustment: Report the amount disallowed by a third party for the charge (if on Lines 1–12).
Column E, Sliding Fee Discount: Report the amount written off for eligible patients per health center policies
(Line 13). Calculate as retail charge (or pharmacy charge), minus amount collected (by pharmacy or health
center) from patients, minus amount owed by patients as their share of payment.
9E
DO NOT report pharmacy revenue on Table 9E, and DO NOT use Table 9E to report net revenue from the
pharmacy. Report actual gross revenue on Table 9D.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
188 2023 UDS MANUAL | Appendix B
DONATED DRUGS, INCLUDING VACCINES
Tables
Affected
Treatment
8A
If the drugs are donated to the health center and then dispensed to patients, report their value (generally
calculated at 340B rates) on Line 18, Column C.
If the drugs are donated directly to the patient, the health center is not required to report the value of the
drugs; however, it is preferred that the value be included for a better understanding of the program.
9D
If the health center charges patients a dispensing fee, report only this amount and its collection and/or write-
off.
9E
DO NOT report any amount, even though generally accepted accounting principles (GAAP) might suggest
another treatment for the value.
CLINICAL DISPENSING OF DRUGS
Clinic areas of health centers dispense many pharmaceuticals, including vaccines, allergy shots, contraceptives,
and MOUD. This may be a service associated with the visit or, in the case of vaccinations, a community service.
These services DO NOT count as a visit, but charging patients for them is appropriate unless the clinic received
the drugs for free.
Tables
Affected
Treatment
3A, 3B, 4
DO NOT report these individuals as patients if this is the only service they received during the year.
5
DO NOT report these services as visits.
6A
DO NOT report these on Table 6A; they are not visits.
8A
Report drug costs on Line 8b, Pharmaceuticals (not on Line 3, Other Medical Costs). In the case of vaccines
obtained at no cost through Vaccines for Children, HRSA (for COVID-19 vaccines, test kits, and supplies),
or other state or local programs, report the value on Line 18, Donated Services and Supplies.
9D
Report full charges, collections, adjustments, and discounts, as appropriate. It is not appropriate to charge for
a pharmaceutical that has been donated. However, an administration and/or dispensing fee is appropriate.
Note that Medicare has separate flu vaccine rules.
9E
DO NOT report any amount.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
189 2023 UDS MANUAL | Appendix B
ADHC AND PACE
Medicare, Medicaid, and certain other third-party payers often recognize ADHC programs. They involve caring
for an infirm, frail, or elderly patient during the day to permit family members to work and to avoid
institutionalization and preserve the health of the patient. They are quite expensive and may involve extraordinary
per member per month (PMPM) capitation payments, but are cost effective compared to institutionalization.
Patients who have both Medicare and Medicaid coverage are treated as Medi-Medi, as described below. PACE is
even more expansive and may include ADHC services, as well as services to maintain independence for the
elderly.
Tables
Affected
Treatment
3A, 3B, 4
Report the individuals seen during the year in ADHC and PACE programs as patients if one or more of their
encounters are countable visits.
5
When a medical or mental health provider does a formal, separately billable examination of a patient at the
ADHC/PACE facility, treat it as any other medical visit.
DO NOT count the nursing, observation, monitoring, and dispensing of medication services that are bundled
together to form an ADHC service as a visit for the purposes of reporting. Personnel are included on Line
29a, Other Programs and Services.
6A, 6B, 7
Report the clinical activity provided to patients at ADHC and PACE facilities, as appropriate, on the clinical
tables.
8A
If the health center provides and bills medical services separately from the ADHC charge, report the
associated costs on Lines 1–3. Report all other costs on Line 12. Similarly, include PACE costs for medical
on Lines 1–3, pharmacy costs on Lines 8a–8b, and all other costs on Line 12.
9D
Report ADHC charges and collections on this table, generally as Medicaid and/or Medicare. Because of
FQHC procedures, it is possible that there will also be significant positive or negative adjustments. In
addition, see Medi-Medi, below.
MEDI-MEDI/DUALLY ELIGIBLE
Some individuals are eligible for and enrolled in both Medicare and Medicaid (commonly referred to as Medi-
Medi or dually eligible). In this case, Medicare is primary and billed first. After Medicare pays its (usually
FQHC-associated Z code or geographic-rate-adjusted) fee, the remainder is billed to Medicaid, which pays an
amount based on policy that varies from state to state.
Tables
Affected
Treatment
4
Report patients on Line 9, Medicare.
DO NOT report as Medicaid. In addition, report these patients on Line 9a, Dually Eligible (Medicare and
Medicaid); this line is a subset of the total reported on Line 9, Medicare.
9D
While the entire charge initially shows as a Medicare charge, after Medicare makes its payment, the remaining
allowable amount is reclassified to Medicaid. Report the payment received from Medicaid on Line 1 in
Column B. Report the difference between the charge and the collection as a positive or negative adjustment,
depending on the amount. The health center must ensure that the charge is reclassified from Medicare to
Medicaid. If your system does not reallocate the charge automatically, it should be done manually.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
190 2023 UDS MANUAL | Appendix B
CERTAIN GRANT-SUPPORTED CLINICAL CARE PROGRAMS: BCCEDP, TITLE X, ETC.
Some programs pay providers on a fee-for-service or fee-per-visit basis under a contract, which may or may not
also have a cap on total payments per grant period (usually the state fiscal year). They cover a very narrow range
of services. Breast and cervical cancer early detection and family planning programs are the most common, but
there are others.
These are fee-for-service or fee-per-visit programs only.
Tables
Affected
Treatment
4
These programs are NOT insurance. They pay for a service, but health centers must classify patients
according to their primary health insurance carrier. Most of these programs DO NOT serve insured patients,
so most of the patients would be reported on Line 7 as uninsured.
9D
Although the patient is likely uninsured, there is an “other public” payer for the service. Report the health
center’s usual and customary charge for the service (NOT the negotiated fee paid by the public entity) on
Line 7 in Column A and the payment in Column B. Because the payment will almost always be different
from the charge, report the difference as an adjustment in Column D.
9E
DO NOT report the grant or contract covering the fee-for-service or fee-per-visit amount on Table 9E. Fully
account for this on Table 9D.
STATE OR LOCAL INDIGENT CARE PROGRAMS
These pay for a wide range of clinical services through a state or local government grant earmarked for uninsured
patients, generally those under an income limit. Most of these programs set payment caps and often make
payments in a different fiscal year than that in which the patient received the service. IHS PL 93-638 Compact
funds are included.
Tables
Affected
Treatment
4
While patients may need to meet eligibility criteria, these programs are NOT public insurance. Count patients
receiving care through these programs on Line 7 as uninsured, unless they have insurance.
9D
The health center’s usual charges for each service are charged directly to patients (reported on Line 13,
Column A). If patients pay any co-payment, report it in Column B. If they are responsible for a co-payment
but DO NOT pay it, it remains a receivable until it is collected or is written off as bad debt in Column F.
Report the portion of the charge not covered by the indigent program or the patient’s responsibility as a
sliding fee discount in Column E.
9E
Report the total amount received during the calendar year from the state or local indigent care program or
IHS PL 93-638 Compact fund on Line 6a and specify the source.
WORKERS’ COMPENSATION
Workers’ compensation is a form of liability insurance for employers and NOT health insurance for employees.
Tables
Affected
Treatment
4
If workers’ compensation covers a patient’s bills, the patient usually has related insurance. Report that on
Table 4 (even if the health center is not billing the insurance). Patients with work-related insurance go on
Line 11 (Private). Those without any health insurance go on Line 7 (Uninsured).
9D
Report charges, collections, and adjustments for workers’ compensation-covered services on Line 10 (Private
Non-Managed Care).

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
191 2023 UDS MANUAL | Appendix B
TRICARE, TRIGON, PUBLIC EMPLOYEES’ INSURANCE, ETC.
Many government employees have insurance.
Tables
Affected
Treatment
4
Report them on Line 11 (Private), NOT on Line 10a.
Note: Coverage directly through the Department of Veterans Affairs is a form of “other public” payment,
NOT a form of medical insurance. Identify if the patient has primary medical insurance.
9D
Report charges, collections, and adjustments on Lines 10–12 (Private), NOT on Lines 7–9.
CONTRACT SITES
Some health centers have included in their scope of project a service delivery site (such as a school, workplace, or
jail
) where they provide services to patients at a contracted flat rate per session or other similar rate that is not
based on the volume of work performed. The agreement generally stipulates whether and under what
circumstances the health center may bill third parties.
Tables
Affected
Treatment
4
Lines 1–6, Income: Obtain information on income from patients. In prisons, assume that all are at 100% and
below FPG (Line 1). In schools, income should be that of the parent(s) or caregiver(s), or report as
“Unknown.” In the limited case of minor consent services, patients should be reported as below poverty. In
the workplace, income is the patient’s family/household income or, if not known, “Unknown” (Line 5).
Lines 7–12, Insurance: Record the form of medical insurance the patient has, regardless of the health center’s
ability to bill that source. (Medicaid often covers children in school-based service sites even though they
have another provider. Report these children as Medicaid patients.) The health center’s contracting agency is
not an insurer. Except for confidential minor consent services, it is not acceptable to assume that a student is
uninsured.
5
Report all visits as appropriate.
DO NOT reduce or reclassify FTEs for travel time to and from contract sites.
8A
Costs will generally be considered medical (Lines 1–3) unless other services (mental health, case
management, etc.) are being provided.
DO NOT report on Line 12: Other Related Services.
9D
Unless the health center charges a visit to a third party such as Medicaid, report the health center’s usual and
customary charges on Line 9 (Other Public) if a government entity or Line 10, Column A (Private) if
privately run. Report the amount paid by the contractor in Column B. Report the difference (positive or
negative) in Column D (Adjustments).
9E
DO NOT report contract revenue on Table 9E.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
192 2023 UDS MANUAL | Appendix B
THE CHILDREN’S HEALTH INSURANCE PROGRAM (CHIP)
CHIP provides health coverage to eligible children through Medicaid and/or separate CHIP programs. CHIP is
administered by states, according to federal requirements. The program is funded jointly by states and the federal
government.
Tables
Affected
Treatment
4
Medicaid: If Medicaid handles CHIP and the enrolled patients are identifiable, report them on Line 8b. If it is
not possible to differentiate CHIP administered through Medicaid from regular Medicaid, report the enrolled
patients on Line 8a with other Medicaid patients.
Non-Medicaid: Report CHIP-enrolled patients in states that DO NOT use Medicaid as “Other Public CHIP”
on Line 10b. DO NOT report the enrollees on Line 11 (Private) even if a private insurance plan administers
the program.
9D
Medicaid: Report on Lines 1–3, as appropriate.
Non-Medicaid: Report on Lines 7–9 (Other Public), as appropriate. DO NOT report on Lines 10–12
(Private), even if a private insurance company administers the plan.
CARVE-OUTS
Relevant to capitated managed care only: The health center has a capitated contract with an HMO that
stipulates one set of CPT codes will be covered by the capitation fee, regardless of service frequency, and another
set of codes (or all other codes) will be paid for by the HMO on a fee-for-service basis (the carve-outs) when
appropriate. Most common carve-outs involve mental health, lab, radiology, and pharmacy, but may include
specific specialty care or diagnoses (e.g., perinatal care or HIV).
Tables
Affected
Treatment
4
Patient Member Months: Member months are reported on Line 13a in the appropriate column, regardless of
whether the patient made use of services in any or all of those months. DO NOT report on Line 13b (fee-for-
service managed care member months) for the carved-out services, regardless of payments received.
9D
Lines 2a/b, 5a/b, 8a/b, 11a/b: Report covered charges and related capitation payments on the “a” lines and
carve-out charges and payments on the “b” lines. Report wraparound payments on both lines using the health
center’s allocation process.
INCARCERATED PATIENTS
Some health centers contract with jails or prisons to provide health services to inmates. These arrangements can
vary in terms of the contractual arrangement and location for providing health services to patients.
Tables
Affected
Treatment
4
Assume prisoners’ individual income is at or below 100% FPG (Line 1).
Unless the institution has arranged for inmate Medicaid enrollment, assume that inmates are uninsured.
9D
Report the health center’s usual and customary charges for the service in Column A and the payments in
Column B. Because the payment will almost always be different from the charge, report the difference as an
adjustment in Column D.
Assuming the jail or prison is billed for the patient’s services, report on the following lines:
• Line 7 (Other Public) if a government entity
• Line 10 (Private) if privately run
9E
DO NOT report the grant or contract on Table 9E. Report revenue fully on Table 9D.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
193 2023 UDS MANUAL | Appendix B
HIT/EHR PERSONNEL AND COSTS
HIT, including EHR systems (some of which have integrated PMS), record clinical activities and help providers
manage and integrate patient services. As such, they are part of a QI program, though some aspects count in other
service categories.
Tables
Affected
Treatment
5
Include personnel who document services in the HIT/EHR, perform data entry, training, and technical
assistance functions in the appropriate service category for which they perform these functions (e.g., scribes).
DO NOT report as IT personnel or QI personnel.
Report personnel members dedicating some or all of their time to design, operation, and oversight of QI
systems; data specialists; statisticians; and HIT/EHR or medical form designers as QI personnel on Line 29b.
Report personnel managing the hardware and software of a practice management billing and collection
system as non-clinical support personnel under IT, Line 30c.
8A
Report costs for personnel who document services in the HIT/EHR or perform data entry, training, and
technical assistance functions in the appropriate service category for which they perform these functions,
NOT as IT personnel or QI personnel.
Report costs associated with licenses, depreciation of the hardware and software, software support services,
and annual fees for other aspects of the HIT/EHR on Line 3 (Other Medical). If the HIT/EHR covers dental
and/or mental health, then appropriately allocate some of the costs to those lines as well.
Report costs for personnel noted above as being included in QI on Line 12a.
Report costs for personnel managing the hardware and software of a practice management billing and
collection system as non-clinical support on Line 15.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
194 2023 UDS MANUAL | Appendix B
ISSUANCE OF VOUCHERS FOR PAYMENT OF SERVICES
Voucher programs have traditionally delivered primary and specialty care services to agricultural workers in
geographically dispersed areas. Some homeless and other health center programs also use vouchers to outsource
care they cannot provide in-house. This involves contracting with providers outside of the health center. Vouchers
authorize a third-party provider to deliver the services and then submit the voucher to the health center for
payment. Payment is generally less than the provider’s full fee but consistent with other payers, such as Medicaid.
Tables
Affected
Treatment
ZIP Code,
3A, 3B, 4
Report patients even if the only service they received was a paid vouchered service if these services would
make the patient eligible for inclusion if the health center provided them. For example, a vouchered taxi ride
or prescription would not make the individual “countable” because health centers DO NOT count
transportation or pharmacy services on Table 5, but a vouchered eye exam would make the patient countable.
5
Column A: There is no way to account for the time of the voucher providers. As a result, report 0 FTEs for
these services. If there is a provider who works at the health center, count the FTE of that provider. For
example, count the one-day-a-week family practitioner who works on voucher at the health center as 0.20
FTEs on Line 1.
Columns B and B2: Report all visits covered by voucher. DO NOT report visits where the referral is to a
provider who is not paid for the service (e.g., a “voucher” to a doctor who donates five visits per week or one
that pays a portion of the provider’s fee with the rest being the patient’s responsibility does not generate a
visit on Table 5).
6A, 6B, 7
Diagnoses and Services: The voucher program should receive a bill from the provider, similar to a Health
Care Financing Administration (HCFA)-1500, that lists the services and diagnoses. Health centers should
track these and report them on Tables 6A, 6B, and 7.
8A
Cost of Vouchered Services: Report the costs on the appropriate service line(s). Report medical vouchers on
Line 1 (NOT Line 3), dental vouchers on Line 5, etc. Report only those costs paid directly by the health
center.
Discounts: Virtually all clinical providers receive less than their full fee. Some health centers report the
amount of these discounts as “donated services.” While this is not required, health centers may report the
difference between the voucher provider’s full fee and the contracted voucher payment as a donated service
on Line 18, Column C.
9D
Column A, Charges: Report the full charge that providers show on their HCFA-1500 on Line 13 (Self-Pay).
DO NOT use the voucher amount as the full charge.
Column B, Collections: If the patient paid the voucher program or provider a nominal or other fee, report this
in Column B.
Column E, Sliding Fee Discounts: Report the difference between the full charge and the amount that the
patient was supposed to pay in Column E. DO NOT report the full amount in Column E if the patient should
have paid the health center or voucher provider but did not complete payment.
Column F, Bad Debt: Report any amount (such as a nominal fee) that the patient was supposed to pay to the
health center but did not. Report bad debts according to the health center’s financial policies. DO NOT report
amounts that were due but not paid to the referral provider by the health center or a third-party payer.
UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
195 2023 UDS MANUAL | Appendix B
NEW START OR NEW ACCESS POINT (NAP)
Health center grants or designations awarded for the first time (new start) may be added prior to October 1 during
the calendar year. New starts must submit data for the full calendar year (covering January 1 to December 31).
Health center service delivery sites may be added in scope of project at any point during the calendar year through
a change in scope (CIS) request or a NAP award. Active, existing health centers are required to submit data for in-
scope activities based on the CIS approval date and/or NAP site implementation date.
Tables
Affected
Treatment
Patients
by ZIP
Code, 3A,
3B, 4
It is understood that a health center may have never collected some of the data required to be reported in the
UDS prior to the start of Notice of Award, such as veteran status, gender identity, member months in
managed care, etc. Provide the best data available, but for the first year only, you may have some unusual
numbers. Work with your UDS Reviewer to explain apparent data inconsistencies.
6B, 7
If the added service delivery site or health center will transition to a new HIT/EHR during the calendar year,
gather the information for the year across the two systems and analyze them in a separate database to remove
any duplication in the data.
RELATIONSHIP BETWEEN PERSONNEL ON TABLE 5 AND COSTS ON TABLE 8A
Personnel classifications should be consistent with cost classifications. The chart below illustrates the relationship
between the two tables. The personnel on Table 5 are routinely compared to the costs on Table 8A during the
review and analysis process. If there is a reason why such a comparison would look unusual (e.g., volunteers on
Table 5 result in no cost on Table 8A or contractor costs on Table 8A with no corresponding FTEs on Table 5),
include an explanation on Table 8A. Note that the cost categories on Table 8A are not in the same sequential
order as the personnel categories on Table 5.
FTEs Reported on Table 5, Line: Have Costs Reported on Table 8A, Line:
1–12: Medical Personnel
1: Medical Personnel
13–14: Medical Lab and X-ray
2: Medical Lab and X-ray
16–18: Dental
5: Dental
20a–20c: Mental Health
6: Mental Health
21: Substance Use Disorder
7: Substance Use Disorder
22: Other Professional
9: Other Professional
22a–22c: Vision
9a: Vision
23a–23d: Pharmacy
8a: Pharmacy
24–28: Enabling
11a–11h: Enabling
24: Case Managers
11a: Case Management
25: Health Education Specialists
11d: Health Education
26: Outreach Workers
11c: Outreach
27: Transportation Personnel
11b: Transportation
27a: Eligibility Assistance Workers
11e: Eligibility Assistance
27b: Interpretation Personnel
11f: Interpretation Services
27c: Community Health Workers
11h: Community Health Workers
28: Other Enabling Services
11g: Other Enabling Services
29a: Other Programs and Services
12: Other Program-Related Services
29b: Quality Improvement Personnel
12a: Quality Improvement
30a–30c and 32: Non-Clinical Support Services
15: Non-Clinical Support Services
31: Facility Personnel
14: Facility
UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
196 2023 UDS MANUAL | Appendix B
RELATIONSHIP BETWEEN INSURANCE ON TABLE 4 AND REVENUE ON TABLE 9D
Revenue sources are generally aligned with patient insurance. The chart below illustrates the relationship between
the two tables. The insurance on Table 4 (primary medical insurance as of the last visit) is routinely compared to
the revenue on Table 9D (insurance payer at the time of each visit) during the review and analysis process. If
there is a reason why such a comparison would look unusual (e.g., a large change in insurance coverage), include
an explanation on Table 9D.
Primary Third-Party Medical Insurance on Table 4, Line: Have Revenue Reported on Table 9D, Line:
7: Uninsured—No medical insurance at last visit (includes patients
whose service is reimbursed through grant, contract, or indigent
care funds)
13: Self-Pay—Include co-pays and deductibles,
state and local indigent care programs (DO NOT
include revenues from programs with limited
benefits; See Other Public, Lines 7–9)
8a and 8b: Medicaid and Medicaid CHIP (includes Medicaid
managed care programs and all forms of state-expanded Medicaid)
1–3: Medicaid (includes Medicaid expansion)
9: Medicare (includes Medicare Advantage)
4–6: Medicare
9a: Dually eligible (Medicare and Medicaid)
4–6: Medicare, initially, with balance reallocated to
Medicaid
10a: Other Public non-CHIP—State and local government insurance
that covers primary care
7–9: Other Public—Include patient service revenue
from programs with limited benefits, such as family
planning (Title X), EPSDT, BCCEDP, etc.
10b: Other Public CHIP (private carrier outside Medicaid)
7–9: Other Public
11: Private—Commercial insurance, including insurance purchased
from state or federal exchanges (DO NOT include workers’
compensation coverage as health insurance—it is a liability
insurance)
10–12: Private—Charges and collections from
contracts with private (commercial) carriers,
private schools, private jails, Head Start, workers’
compensation, and state and federal exchanges
13a: Capitated managed care enrollees
“a” lines
13b: Fee-for-service managed care enrollees
“b” lines
RELATIONSHIP BETWEEN PRENATAL CARE ON TABLE 6B AND DELIVERIES ON TABLE 7
The chart below illustrates the relationship and accounting of prenatal care patients and the birth outcomes to be
reported on Tables 6B and 7. A “Yes” indicates that the information is to be reported in the specified table and
section; “No” indicates the information is NOT to be reported. As a result, it would be unusual for the count of
prenatal care patients to equal the birth outcomes. The prenatal care patients on Table 6B are routinely compared
to the deliveries and birth outcomes on Table 7 during the review and analysis process. If there is a reason why
such a comparison would look unusual, include an explanation on the appropriate table.
Prenatal Care Patient and Birth
Outcome Scenarios
Table 6B, Lines 1–9
(Age and Trimester of
Entry)
Table 7, Column 1a
(Patients who Delivered)
Table 7, Columns 1b–1d
(Birth Outcomes—
report each baby
separately)
Patients still in prenatal care
Yes
No
No
Patients known to have delivered,
with known birth outcomes
Yes
Yes
Yes
Patients known to have delivered,
but birth outcomes unknown
Yes
Yes
No
Patients who miscarried
Yes
No
No
Patients with a stillbirth outcome
Yes
Yes
No
Patients lost to follow-up, birth
outcomes unknown
Yes
No
No

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
197 2023 UDS MANUAL | Appendix B
RELATIONSHIP BETWEEN RACE AND ETHNICITY ON TABLES 3B AND 7
The patient population for each clinical quality measure on Table 7 is defined in terms of race and ethnicity, and
comparisons are made to the race and ethnicity numbers reported on Table 3B. The following table illustrates the
crosswalk between the comparable fields across the two tables.
Race
Ethnicity
Table 3B Reference
Table 7 Reference
Asian Hispanic, Latino/a, or Spanish Origin Line 1, Column A1–A5 Line 1a
Asian
Not Hispanic, Latino/a, or Spanish Origin
Line 1, Column B
Line 2a
Asian Indian Hispanic, Latino/a, or Spanish Origin Line 1a, Column A1–A5
Line 1a1m, 1a1p,
1a1c, 1a1a, or 1a1o
Asian Indian
Not Hispanic, Latino/a, or Spanish Origin
Line 1a, Column B
Line 2a1
Chinese Hispanic, Latino/a, or Spanish Origin Line 1b, Column A1–A5
Line 1a2m, 1a2p,
1a2c, 1a2a, or 1a2o
Chinese
Not Hispanic, Latino/a, or Spanish Origin
Line 1b, Column B
Line 2a2
Filipino Hispanic, Latino/a, or Spanish Origin Line 1c, Column A1–A5
Line 1a3m, 1a3p,
1a3c, 1a3a, or 1a3o
Filipino
Not Hispanic, Latino/a, or Spanish Origin
Line 1c, Column B
Line 2a3
Japanese Hispanic, Latino/a, or Spanish Origin Line 1d, Column A1–A5
Line 1a4m, 1a4p,
1a4c, 1a4a, or 1a4o
Japanese
Not Hispanic, Latino/a, or Spanish Origin
Line 1d, Column B
Line 2a4
Korean Hispanic, Latino/a, or Spanish Origin Line 1e, Column A1–A5
Line 1a5m, 1a5p,
1a5c, 1a5a, or 1a5o
Korean
Not Hispanic, Latino/a, or Spanish Origin
Line 1e, Column B
Line 2a5
Vietnamese Hispanic, Latino/a, or Spanish Origin Line 1f, Column A1–A5
Line 1a6m, 1a6p,
1a6c, 1a6a, or 1a6o
Vietnamese
Not Hispanic, Latino/a, or Spanish Origin
Line 1f, Column B
Line 2a6
Other Asian Hispanic, Latino/a, or Spanish Origin Line 1g, Column A1–A5
Line 1a7m, 1a7p,
1a7c, 1a7a, or 1a7o
Other Asian
Not Hispanic, Latino/a, or Spanish Origin
Line 1g, Column B
Line 2a7
Native Hawaiian Hispanic, Latino/a, or Spanish Origin Line 2a, Column A1–A5
Line 1b1m, 1b1p,
1b1c, 1b1a, or 1b1o
Native Hawaiian
Not Hispanic, Latino/a, or Spanish Origin
Line 2a, Column B
Line 2b1
Other Pacific Islander Hispanic, Latino/a, or Spanish Origin Line 2b, Column A1–A5
Line 1b2m, 1b2p,
1b2c, 1b2a, or 1b2o
Other Pacific Islander
Not Hispanic, Latino/a, or Spanish Origin
Line 2b, Column B
Line 2b2
Guamanian or
Chamorro
Hispanic, Latino/a, or Spanish Origin Line 2c, Column A1–A5
Line 1b3m, 1b3p,
1b3c, 1b3a, or 1b3o
Guamanian or
Chamorro
Not Hispanic, Latino/a, or Spanish Origin Line 2c, Column B Line 2b3
Samoan Hispanic, Latino/a, or Spanish Origin Line 2d, Column A1–A5
Line 1b4m, 1b4p,
1b4c, 1b4a, 1b4o
Samoan
Not Hispanic, Latino/a, or Spanish Origin
Line 2d, Column B
Line 2b4
Black/African
American
Hispanic, Latino/a, or Spanish Origin Line 3, Column A1–A5
Line 1cm, 1cp, 1cc,
1ca, or 1co
Black/African
American
Not Hispanic, Latino/a, or Spanish Origin Line 3, Column B Line 2c
American
Indian/Alaska Native
Hispanic, Latino/a, or Spanish Origin Line 4, Column A1–A5
Line 1dm, 1dp, 1dc,
1da, or 1do
American
Indian/Alaska Native
Not Hispanic, Latino/a, or Spanish Origin Line 4, Column B Line 2d
White Hispanic, Latino/a, or Spanish Origin Line 5, Column A1–A5
Line 1em, 1ep, 1ec,
1ea, or 1eo
White
Not Hispanic, Latino/a, or Spanish
Line 5, Column B
Line 2e

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
198 2023 UDS MANUAL | Appendix B
Race
Ethnicity
Table 3B Reference
Table 7 Reference
More than One Race Hispanic, Latino/a, or Spanish Origin Line 6, Column A1–A5
Line 1fm, 1fp, 1fc,
1fa, or 1fo
More than One Race
Not Hispanic, Latino/a, or Spanish Origin
Line 6, Column B
Line 2f
Unreported/Chose
Not to Disclose Race
Hispanic, Latino/a, or Spanish Origin Line 7, Column A1–A5
Line 1gm, 1gp, 1gc,
1ga, or 1go
Unreported/Chose
Not to Disclose Race
Not Hispanic, Latino/a, or Spanish Origin Line 7, Column B Line 2g
Unreported/Chose
Not to Disclose Race
Unreported/Chose Not to Disclose Ethnicity
Line 7, Column C Line h

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
199 2023 UDS MANUAL | Appendix C
Appendix C: Reduced Number of Records Reviewed for
Clinical Quality Measure Reporting
Data from health centers’ electronic health record (EHR) systems are increasingly being used to report on the full
denominator of patients whose characteristics fulfill UDS clinical quality measure (CQM) specifications. The
option of using a chart sampling method (i.e., a scientifically drawn random sample of 70 patient charts) for
reporting CQMs on Tables 6B and 7 is no longer available for UDS reporting. Using EHR data to report UDS
clinical quality measures among all patients for which each CQM applies allows for a more complete
understanding of health centers’ clinical quality performance and patient health status.
For each measure discussed on Tables 6B and 7 (except the perinatal measures), health centers have the option of
reporting on their entire patient population as the Number of Records Reviewed (Column B) or a reduced
denominator consisting of a minimum of 80% of all medical (or dental for the dental sealants measure) patients
from all service delivery sites and grant-funded programs. While a reduced number of records reviewed is
permitted, a full EHR or health information technology (HIT) system reporting is preferred. Although a reduced
denominator is permitted for the Number of Records Reviewed, health centers must be able to report on the total
patients to be assessed for the measure (denominator, Column A) using their EHR or HIT system.
Note: Data source must cover the measurement period (e.g., 5 years for Pap tests, 2 years for immunizations) and
include information to assess meeting the numerator criteria with the clinical quality measure, as well as to
evaluate exclusions.
A reduced denominator generally provides the ability to facilitate accurate reporting if all conditions of individual
CQM requirements are met. You may only report a reduced denominator (Number of Records Reviewed, Table
6B, Column B; and Table 7, Columns 2b, and 3b) if the factors that required its use are unrelated to the measure
variables outlined in measure-specific reporting requirements on Tables 6B and 7.
If you DO NOT have an EHR or HIT system in place, or are unable to report a minimum of 80% of all medical
(or dental for the dental sealants measure) patients from all service delivery sites, please contact the UDS Support
Center to discuss reporting options.
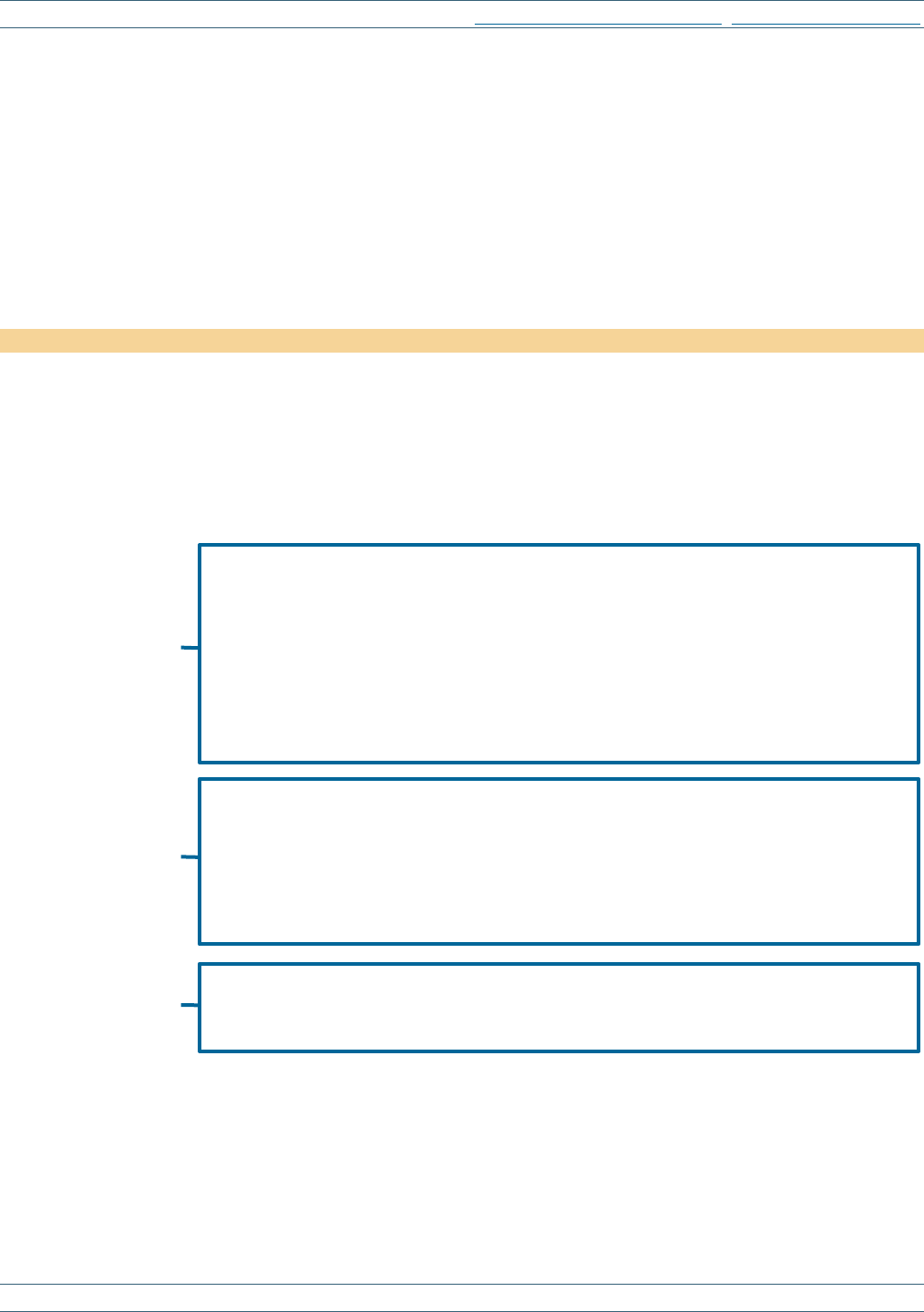
UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
200 2023 UDS MANUAL | Appendix D
Appendix D: Health Center Health Information Technology
(HIT) Capabilities
INTRODUCTION
The HIT Capabilities Form collects information through a series of questions on the health center’s HIT
capabilities, including EHR interoperability and eligibility for CMS Promoting Interoperability programs. The
HIT Form must be completed and submitted as part of the UDS submission. The form includes questions about
the health center’s implementation of an EHR, certification of systems, and how widely adopted the system is
throughout the health center and its providers.
There are no major changes to this form.
QUESTIONS
The following questions appear in the EHBs. Complete them before you file the UDS Report. Reporting
requirements for the HIT questions are on-screen in the EHBs as you complete the form. Respond to each
question based on your health center status as of December 31, 2023.
1. Does your health center currently have an electronic health record (EHR) system installed and in use, at a
minimum, for medical care, by December 31?
a. Yes,
installed at
all service delivery
sites and used by
all providers
• For the purposes of this response, “providers” mean all medical providers, including
physicians, nurse practitioners, physician assistants, and certified nurse midwives.
• Although some or all of the dental, mental health, or other providers may also be using the
system, as may medical support personnel, this is not required to choose response (a).
• For the purposes of this response, “all service delivery sites” means all permanent service
delivery sites where medical providers serve health center medical patients.
• It DOES NOT include administrative-only locations, hospitals or nursing homes, mobile vans,
or sites used on a seasonal or temporary basis.
• You may check this option if a few newly hired, untrained personnel are the only ones not
using the system.
b. Yes, but only
installed at
some service
delivery sites or
used by
some providers
• Select option (b) if one or more permanent service delivery sites did NOT have the EHR
installed or in use (even if this is planned), or if one or more medical providers (as defined on
this page under [a]) do not yet use the system.
• When determining if all providers have access to the system, the health center should also
consider part-time and locum providers who serve clinic patients.
• DO NOT select this option if the only medical providers who did not have access were those
who were newly hired and still being trained on the system.
c. No
• Select “no” if no EHR was in use on December 31, even if you had the system installed and
training had started.
• If the health center purchased an EHR but has not yet put it into use, answer “no.”

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
201 2023 UDS MANUAL | Appendix D
If response is “c. No,” skip to Question 11. If response is “a” or “b”, continue to next question.
If more than one medical EHR is used, answer “Yes,” to Question 1 and select “a” if they are used at all service
delivery sites and used by all providers or select “b” if they are used at some service delivery sites or used by
some providers.
If “Yes, but only installed at some service delivery sites or used by some providers” is selected, a box expands for
health centers to identify how many service delivery sites have the EHR in use and how many (medical) providers
are using it. Please enter the number of service delivery sites (as defined under question 1) where the EHR is in
use and the number of providers who use the system (at all service delivery sites). Include part-time and locum
medical providers who serve clinic patients. Count a provider who has separate login identities at more than one
service delivery site as just one provider.
This next set of questions seeks to determine whether the health center installed an EHR by December 31 and, if
so, which product was in use, how broad system access was, and what features were available and in use. DO
NOT include PMS or other billing systems, even though they can often produce much of the UDS data.
If a system is in use (i.e., if [a] or [b] has been selected), indicate whether it has been certified by the Office of the
National Coordinator—Authorized Testing and Certification Bodies
.
1a. Is your system certified by the Office of the National Coordinator for Health IT (ONC) Health IT
Certification Program?
a. Yes
b. No
Health centers are to indicate the vendor, product name, version number, and ONC-certified health IT
product list number. This information is available on the Certified Health IT Product List
. Select the most
current version number being used. If you have more than one EHR (if, for example, you acquired another
practice with its own EHR), report the EHR that will be the successor system or the EHR used for
capturing primary medical care.
1a1. Vendor
1a2. Product Name
1a3. Version Number
1a4. ONC-certified Health IT Product List Number
Note: The Certified Health IT Product List (CHPL) Number is a standardized number that reflects your
certified product and version. Step-by-step instructions for using the CHPL to find your system are
available in the CHPL Public User Guide
.
1b. Did you switch to your current EHR from a previous system this year?
a. Yes
b. No

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
202 2023 UDS MANUAL | Appendix D
1c. Do you use more than one EHR, data collection, and/or data analytics system across your organization?
Select “Yes” if the health center has more than one EHR that flows into one central HIT/EHR or practice
management system.
a. Yes
b. No
1c1. If yes, what is the reason?
a. Additional EHR/data system(s) are used during transition from one primary EHR to another
b. Additional EHR/data system(s) are specific to one service type (e.g., dental, behavioral health, care
coordination)
c. Additional EHR/data system(s) are used at specific service delivery sites with no plan to transition
d. Additional EHR/data system(s) are used for analysis and reporting (such as for clinical quality
measures or custom reporting)
e. Other (please describe ______)
1d. Question removed.
1e. Question removed.
2. Question removed.
3. Question removed.
4. Which of the following key providers/health care settings does your health center electronically exchange
clinical or patient information with? (Select all that apply.)
a. Hospitals/Emergency rooms
b. Specialty providers
c. Other primary care providers
d. Labs or imaging
e. Health information exchange (HIE)
23
f. Community-based organizations/social service partners
g. None of the above
h. Other (please describe ______)
5. Does your health center engage patients through health IT in any of the following ways? (Select all that
apply.)
a. Patient portals
b. Kiosks
c. Secure messaging between patient and provider
d. Online or virtual scheduling
e. Automated electronic outreach for care gap closure or preventive care reminders
23
HIEs are typically state or regional data exchanges that support information sharing between different organizations, provider types, and technology
vendors. More information on HIEs can be found on the Health Information Exchange webpage
.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
203 2023 UDS MANUAL | Appendix D
f. Application programming interface (API) patient access to their health record through mHealth apps
24
g. Other (please describe _______)
h. No, we DO NOT engage patients using HIT
6. Question removed.
7. Question removed.
8. Question removed.
9. Question removed.
10. How does your health center utilize HIT and EHR data beyond direct patient care? (Select all that apply.)
a. Quality improvement
b. Population health management
c. Program evaluation
d. Research
e. Other (please describe ______)
f. We DO NOT utilize HIT or EHR data beyond direct patient care
11. Does your health center collect data on individual patients’ social risk factors, outside of the data countable in
the UDS?
Note: Health centers should respond “a. Yes” below only if they are screening for social risks, meaning they
have a consistent set of questions that are asked of individual patients uniformly for the purposes of collecting
information on the non-medical, health-related social needs of patients, such as housing instability and/or
food insecurity, beyond those demographic patient characteristics captured elsewhere on the UDS Report.
Collecting race, ethnicity, sexual orientation, gender identity, and/or income level would not be considered
here as collecting data on individual patients’ social risk factors, as this information is already counted in the
UDS Report, on Tables 3B and 4. Similarly, collecting data on intimate partner violence, domestic violence,
and/or human trafficking would not be considered, as this information is already counted in the UDS Report,
on Table 6A.
a. Yes
b. No, but we are in planning stages to collect this information
c. No, we are not planning to collect this information
If response to Question 11 is “a,” then continue to the next question. If response is “b” or “c,” skip to
Question 12b.
11a. How many health center patients were screened for social risk factors using a standardized screener during
the calendar year? (Only respond to this if the response to Question 11 is “a. Yes.”) _____________
12. Which standardized screener(s) for social risk factors, if any, did you use during the calendar year? (Select all
that apply. Only respond to this if your response to Question 11a is greater than 0.)
a. Accountable Health Communities Screening Tools
b. Upstream Risks Screening Tool and Guide
24
More information on How APIs in Health Care can Support Access to Health Information: Learning Module

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
204 2023 UDS MANUAL | Appendix D
c. IHELLP
d. Recommend Social and Behavioral Domains for EHRs
e. Protocol for Responding to and Assessing Patients’ Assets, Risks, and Experiences (PRAPARE)
f. Well Child Care, Evaluation, Community Resources, Advocacy, Referral, Education (WE CARE)
g. WellRx
h. Health Leads Screening Toolkit
i. Other (please describe: __________)
Note: Health centers that are screening for social risks, using the definition noted in Question 11, but are
NOT using one of the standardized screening tools listed should respond “i. Other.” Specify that you are
using standardized questions from various screening tools.
j. We DO NOT use a standardized screener (response to Question 12b is required when selected)
Note: Only select “j. We DO NOT use a standardized screener” if you DO NOT use a consistent set of
questions/approach to screen patients for social risks. If Question 11a is greater than 0 and the health center
responds to Question 12, continue to the next question. If Question 11a is 0 and Question 12 is any option
other than “j,” skip to Question 13.
12a. Of the total patients screened for social risk factors (Question 11a), please provide the total number of
patients that screened positive for any of the following at any point during the calendar year. (A patient may
experience multiple social risks and should be counted once for each risk factor they screened positive for,
regardless of the number of times screened during the year.)
a. Food insecurity ___________
b. Housing insecurity ___________
c. Financial strain ___________
d. Lack of transportation/access to public transportation ___________
12b. If you DO NOT use a standardized screener to collect this information, please indicate why. (Select all that
apply.) (Only respond to this question if your response to Question 11a is “zero” or if Question 12, option j is
selected.)
a. Have not considered/unfamiliar with standardized screeners
b. Lack of funding for addressing these unmet social needs of patients
c. Lack of training for personnel to discuss these issues with patients
d. Inability to include with patient intake and clinical workflow
e. Not needed
f. Other (please describe ___________)
13. Does your health center integrate a statewide Prescription Drug Monitoring Program (PDMP) database into
the health information systems, such as health information exchanges, EHRs, and/or pharmacy dispensing
software (PDS) to streamline provider access to controlled substance prescriptions?
a. Yes
b. No
c. Not sure

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
205 2023 UDS MANUAL | Appendix D
FAQ FOR APPENDIX D: HEALTH CENTER HIT CAPABILITIES FORM
1. What do we do if our health center acquired a new EHR system and we need to use two different
systems in order to report a full calendar year UDS Report?
Health centers are required to submit one UDS Report that includes unduplicated data for the entire scope of
services included in the grant or designation for the calendar year. It is expected that health centers that
transition from one EHR to another during the reporting year are able to report unduplicated counts of
patients, visits, and other activity, as appropriate. To complete the UDS Report as accurately as possible, your
health center will need to have access to both systems and merge results. Health centers should work to
establish a process to pull and transfer data from the previous EHR system during the merger process. This
may require pulling data from the two systems into a separate database to remove any duplication in the data.
This can be a time-consuming process and it is recommended that health centers begin this process as soon as
the year ends or once the transition has been completed to ensure sufficient time for completion prior to the
submission due date.
2. We use multiple EHRs across our health center that are then aggregated into a single analytics
platform or data warehouse for UDS reporting. How should we be responding to the questions on this
form?
Respond to Question 1 and its sub-questions 1a through 1c1 based on the primary EHR used by your medical
providers. For example, provide the vendor, product, product number, and CHPL number for the primary
EHR used by your medical providers.
Respond to Questions 4 through 10 based on your entire EHR and health IT ecosystem. Your responses
should state where data are exchanged from any of the systems in use at your health center and for what
purposes the data from those systems are used.
3. We combined a few different social risk screeners to do social risk screening of patients (such as to meet
various grant or payer requirements or address unique needs of the community). How do we report
this on Questions 11 through 12b?
Respond “a. Yes” to Question 11 and select “i. Other” on Question 12. Describe the screening tool that you
use in the specify field of Question 12 (for example, describe the screeners that have been combined or note
that a screener was provided by your MCO). Also, report the total number of health center patients screened
using the particular tool(s) you use in Question 11a, and, of those screened, how many screened positive in
each of the four areas specified in Question 12a. If your screener does NOT have a question related to any of
the four areas specified in Question 12a, enter “0” for that area.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
206 2023 UDS MANUAL | Appendix E
Appendix E: Other Data Elements
INTRODUCTION
The questions on the Other Data Elements Form collect information on the changing landscape of health centers
to include expanded services and delivery systems.
Several notable changes have been made to the Other Data Elements Form, as outlined below:
• Medication assisted treatment (MAT) is now referred to as medications for opioid use disorder (MOUD).
• The Drug Addiction Treatment Act of 2000 (DATA) waiver is no longer required to treat opioid use disorder
with medications specifically approved by the U.S. Food and Drug Administration (FDA) (i.e.,
buprenorphine).
QUESTIONS
Report on these data elements as part of your UDS submission. Topics include medications for opioid use
disorder (MOUD), telehealth, and outreach and enrollment assistance. Respond to each question based on your
health center status as of December 31, 2023.
1. Medications for Opioid Use Disorder (MOUD)
a. How many providers, on-site or with whom the health center has contracts, treat opioid use disorder with
medications specifically approved by the U.S. Food and Drug Administration (FDA) (i.e., buprenorphine)
for that indication during the calendar year?
b. During the calendar year, how many patients received MOUD for opioid use disorder from a provider
accounted for in Question 1a?
2. Did your organization use telemedicine to provide remote (virtual) clinical care services?
Note: Telemedicine services refers to remote clinical services with patients.
a. Yes
If “Yes” is selected, proceed to questions 2a1–2a3.
2a1. Who did you use telemedicine to communicate with? (Select all that apply.)
a. Patients at remote locations from your organization (e.g., home telehealth, satellite locations)
b. Specialists outside your organization (e.g., specialists at referral centers)
2a2. What telehealth technologies did you use? (Select all that apply.)
a. Real-time telehealth (e.g., live videoconferencing)
b. Store-and-forward telehealth (e.g., secure e-mail with photos or videos of patient examinations)
c. Remote patient monitoring
d. Mobile Health (mHealth)
2a3. What primary telemedicine services were used at your organization? (Select all that apply.)
a. Primary care
b. Oral health
c. Behavioral health: Mental health
d. Behavioral health: Substance use disorder

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
207 2023 UDS MANUAL | Appendix E
e. Dermatology
f. Chronic conditions
g. Disaster management
h. Consumer health education
i. Provider-to-provider consultation
j. Radiology
k. Nutrition and dietary counseling
l. Other (Please describe ________________)
b. No.
If you did not have telemedicine services, please comment on why. (Select all that apply.)
a. Have not considered/unfamiliar with telehealth service options
b. Policy barriers (Select all that apply.)
i. Lack of or limited reimbursement
ii. Credentialing, licensing, or privileging
iii. Privacy and security
iv. Other (Please describe __________________)
c. Inadequate broadband/telecommunication service (Select all that apply.)
i. Cost of service
ii. Lack of infrastructure
iii. Other (Please describe __________________)
d. Lack of funding for telehealth equipment
e. Lack of training for telehealth services
f. Not needed
g. Other (Please describe __________________)
3. Provide the number of all assists provided during the past year by all trained assisters (e.g., certified
application counselor or equivalent) working on behalf of the health center (personnel, contracted personnel,
or volunteers), regardless of the funding source that is supporting the assisters’ activities. Outreach and
enrollment assists are defined as customizable education sessions about third-party primary care health
insurance coverage options (one-on-one or small group) and any other assistance provided by a health center
assister to facilitate enrollment.
Enter number of assists _______________
Note: Assists DO NOT count as visits on the UDS tables.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
208 2023 UDS MANUAL | Appendix F
Appendix F: Workforce
INTRODUCTION
The Workforce Form collects information through a series of questions on health center workforce. It is important
to understand the current state of health center workforce training and different staffing models to better support
recruitment and retention of health center professionals.
There are no major changes to this form.
QUESTIONS
Report on these data elements as part of your UDS submission. Topics include health professional
education/training (DO NOT include continuing education units) and satisfaction surveys. Respond to each
question based on your health center status as of December 31, 2023.
1. Does your health center provide any health professional education/training that is a hands-on, practical, or
clinical experience?
a. Yes
b. No
1a. If yes, which category best describes your health center’s role in the health professional education/training
process? (Select all that apply.)
a. Sponsor
25
b. Training site partner
26
c. Other (please describe ________________)
2. Please indicate the range of health professional education/training offered at your health center and how many
individuals you have trained in each category
27
within the calendar year.
[blank] a. Pre-Graduate/Certificate b. Post-Graduate Training
Medical [blank] [blank]
1. Physicians
[blank for demonstration]
[blank for demonstration]
a. Family Physicians
[blank for demonstration]
[blank for demonstration]
b. General Practitioners
[blank for demonstration]
[blank for demonstration]
c. Internists
[blank for demonstration]
[blank for demonstration]
d. Obstetrician/Gynecologists
[blank for demonstration]
[blank for demonstration]
e. Pediatricians
[blank for demonstration]
[blank for demonstration]
f. Other Specialty Physicians
[blank for demonstration]
[blank for demonstration]
2. Nurse Practitioners
[blank for demonstration]
[blank for demonstration]
3. Physician Assistants
[blank for demonstration]
[blank for demonstration]
4. Certified Nurse Midwives
[blank for demonstration]
[blank for demonstration]
5. Registered Nurses
[blank for demonstration]
[blank for demonstration]
6. Licensed Practical Nurses/ Vocational
Nurses
[blank for demonstration]
[blank for demonstration]
25
A sponsor hosts a comprehensive health profession education and/or training program, the implementation of which may require partnerships with other
entities that deliver focused, time-limited education and/or training (e.g., a teaching health center with a family medicine residency program).
26
A training site partner delivers focused, time-limited education and/or training to learners in support of a comprehensive curriculum hosted by another
health profession education provider (e.g., month-long primary care dentistry experience for dental students).
27
Examples of pre-graduate/certificate training include student clinical rotations or externships. A residency, fellowship, or practicum would be examples of
post-graduate training. Include non-health-center individuals trained by your health center.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
209 2023 UDS MANUAL | Appendix F
[blank] a. Pre-Graduate/Certificate b. Post-Graduate Training
7. Medical Assistants
[blank for demonstration]
[blank for demonstration]
Dental [blank] [blank]
8. Dentists
[blank for demonstration]
[blank for demonstration]
9. Dental Hygienists
[blank for demonstration]
[blank for demonstration]
10. Dental Therapists
[blank for demonstration]
[blank for demonstration]
10a. Dental Assistants
[blank for demonstration]
[blank for demonstration]
Mental Health and Substance Use
Disorder
[blank] [blank]
11. Psychiatrists
[blank for demonstration]
[blank for demonstration]
12. Clinical Psychologists
[blank for demonstration]
[blank for demonstration]
13. Clinical Social Workers
[blank for demonstration]
[blank for demonstration]
14. Professional Counselors
[blank for demonstration]
[blank for demonstration]
15. Marriage and Family Therapists
[blank for demonstration]
[blank for demonstration]
16. Psychiatric Nurse Specialists
[blank for demonstration]
[blank for demonstration]
17. Mental Health Nurse Practitioners
[blank for demonstration]
[blank for demonstration]
18. Mental Health Physician Assistants
[blank for demonstration]
[blank for demonstration]
19. Substance Use Disorder Personnel
[blank for demonstration]
[blank for demonstration]
Vision [blank] [blank]
20. Ophthalmologists
[blank for demonstration]
[blank for demonstration]
21. Optometrists
[blank for demonstration]
[blank for demonstration]
Other Professionals [blank] [blank]
22. Chiropractors
[blank for demonstration]
[blank for demonstration]
23. Dieticians/Nutritionists
[blank for demonstration]
[blank for demonstration]
24. Pharmacists
[blank for demonstration]
[blank for demonstration]
25. Other (please describe ________)
[blank for demonstration]
[blank for demonstration]
3. Provide the number of health center personnel serving as preceptors at your health center: ____
4. Provide the number of health center personnel (non-preceptors) supporting ongoing health center training
programs: ____
5. How often does your health center conduct satisfaction surveys to providers (as identified in Appendix A
,
Listing of Personnel) working for the health center? Report provider surveys only here. (Select one.)
a. Monthly
b. Quarterly
c. Annually
d. We DO NOT currently conduct provider satisfaction surveys
e. Other (please describe _________)

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
210 2023 UDS MANUAL | Appendix F
6. How often does your health center conduct satisfaction surveys for general personnel (as identified in
Appendix A
, Listing of Personnel) working for the health center (report provider surveys in question 5 only)?
(Select one.)
a. Monthly
b. Quarterly
c. Annually
d. We DO NOT currently conduct personnel satisfaction surveys
e. Other (please describe _________)

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
211 2023 UDS MANUAL | Appendix G
Appendix G: De-Identified Patient-Level Reporting
INTRODUCTION
High-quality accessible data are critical to strategically meeting the needs of patients and identifying opportunities
for clinical process improvement. The growth in health information technology, coupled with the increased
adoption of EHRs, has transformed patient care delivery and underscored the need for secure and rapid exchange
of health data between disparate systems.
Health Level Seven International (HL7®) developed Fast Healthcare Interoperability Resources (FHIR®) version
release 4 (R4) to standardize the electronic exchange of patient data across systems. FHIR R4 has the flexibility to
support a variety of use cases and enhances interoperability by transmitting health data rapidly and more securely
than ever before. It is important for the collection of UDS data to align with interoperability standards and
reporting requirements across HHS and the health care industry. Leveraging FHIR R4 to collect UDS de-
identified patient-level data will improve data granularity, allow for the development of robust patient
management programs, and improve equitable access to high-quality, cost-effective primary care services. The
transition to de-identified patient-level data reporting using FHIR R4 interoperability standards is part of the
natural evolution of HIT.
In addition to aggregate UDS reporting within EHBs, health centers may voluntarily submit de-identified patient-
level reporting (UDS+) using FHIR R4. The aggregate report submitted in EHBs will be the submission of record
for calendar year 2023 UDS reporting.
SCOPE OF UDS+
All health centers are to submit a full UDS Report within EHBs by February 15, 2024.
Beginning with the 2023 UDS reporting, in addition to an aggregate UDS Report submission within EHBs, health
centers may voluntarily submit de-identified patient-level data (UDS+) submitted using HL7 FHIR R4 standards
for UDS, for the data elements on the following tables:
• Patients by ZIP Code Table
• Table 3A: Patients by Age and by Sex Assigned at Birth
• Table 3B: Demographic Characteristics
• Table 4: Selected Patient Characteristics
• Table 6A: Selected Diagnoses and Services Rendered
• Table 6B: Quality of Care Measures
• Table 7: Health Outcomes and Disparities
Health centers choosing to participate in this voluntary reporting will submit through (bulk) FHIR R4 APIs, using
the UDS+ FHIR R4 Implementation Guide (IG) as described in Appendix G
. To learn more about UDS+, please
refer to the Health Center Program Community website.
REPORTING UDS+ DATA
The UDS+ will utilize FHIR R4 to increase the utility of UDS Report data and to reduce the annual reporting
burden by aligning with interoperability standards and reporting requirements used across the U.S. Department of
Health and Human Services and within the health care industry. The UDS+ FHIR R4 Implementation Guide (IG)
defines the set of rules by which health centers can report UDS+ de-identified patient data to HRSA through
FHIR R4 APIs. The UDS+ FHIR R4 IG provides well-defined capability statements, FHIR R4 operations, FHIR
R4 profiles, FHIR R4 extensions, and terminology needed to successfully implement UDS+.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
212 2023 UDS MANUAL | Appendix G
The UDS+ FHIR R4 IG will align HRSA reporting requirements with the Office of the National Coordinator for
Health Information Technology (ONC) and Centers for Medicare & Medicaid Services (CMS) regulations to the
extent possible.
Note: Data submitted through UDS+ will NOT include protected health information (PHI) or identifiable patient
data for successful submission.
RESOURCES AND SUPPORT FOR UDS+ REPORTING
Several resources are available to assist health centers with the use of FHIR R4 standards for UDS reporting:
ONC Resources
Topic and Link Description
21
st
Century Cures Act Final Rule:
Interoperability, Information Blocking, and the
ONC Health IT Certification Program
Federal administrative regulation published in the Federal Register,
which implements certain provisions of the Cures Act related to
advancing EHR interoperability and is designed to give patients and
their health care providers secure access to health information.
Certification of Health IT
Webpages describing elements of ONC’s Health IT Certification
Program, including the program requirements, certification process,
and certified health IT product list.
FHIR® API
Interface that allows a computer program or system to access and
exchange data across systems. APIs define the data structure, format of
the data, and accepted system interactions.
FHIR® Fact Sheets
Four fact sheets developed by ONC and Health Level Seven
International (HL7®) to demystify FHIR® for health care providers
and administrators.
United States Core Data for Interoperability
(USCDI)
A standardized set of health data classes and constituent data elements
for nationwide, interoperable health information exchange.
HL7® Resources
Topic and Link Description
Bulk Data Access Implementation Guide (IG)
Overview of the purpose and use cases for a Bulk Data FHIR® IG.
HL7® FHIR® Implementation Guidance
Checklist
Assists in navigating available resources for the adoption of HL7®
FHIR® standards and API-based approaches to interoperability.
HL7® FHIR® Resource Index
A page for finding FHIR® specification resources by category and
alphabetically.
HL7® Standards
Homepage for HL7®, a not-for-profit, American National Standards
Institute (ANSI)-accredited standards developing organization, which
provides a comprehensive framework and related standards for the
exchange, integration, sharing, and retrieval of electronic health
information.
US Core Implementation Guide
Homepage for the US Core Implementation Guide, which defines the
minimum set of constraints on the FHIR R4 resources to create the US
Core Profiles.
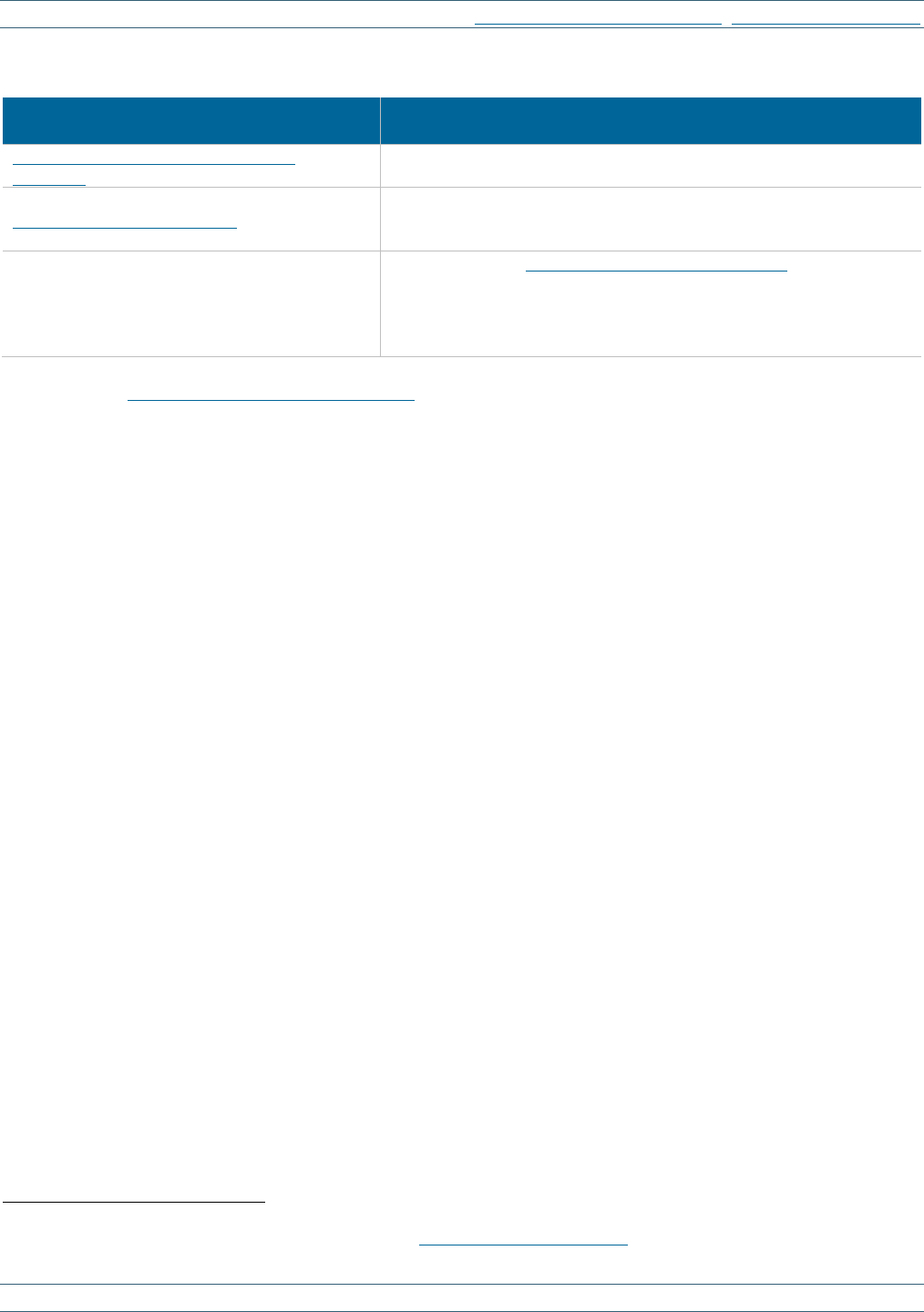
UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
213 2023 UDS MANUAL | Appendix G
BPHC Webpages
Topic and Link Description
UDS Modernization Frequently Asked
Questions
Webpage that provides answers to health center personnel and
stakeholder FAQ about the overall initiative, including UDS+.
UDS Modernization Overview
A webpage that provides the purpose, goals, objectives, and activities
of the UDS Modernization Initiative, including UDS Patient-Level
Submission (UDS+).
UDS+ FHIR R4 Implementation Guide (IG)
Homepage for the Health Center Program Community, which includes
UDS+-related resources, including the UDS+ FHIR R4 IG, which
defines the health IT architectural details and technical specifications
by which health centers can report the UDS+ de-identified patient data
to HRSA using APIs.
Please visit the Health Center Program Community
28
website to access more information about UDS+, including
the UDS+ FHIR R4 IG, resources, and FAQ.
28
Login credentials are required. Users may request access through the Health Center Program Community.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
214 2023 UDS MANUAL | Appendix H
Appendix H: Health Center Resources
Several resources are available to assist health centers with UDS reporting criteria, UDS+, or EHBs system
questions:
Description Contact E-mail or Web Form Phone
UDS reporting questions UDS Support Center
udshelp330@bphcdata.net
or
BPHC Contact Form
Select: UDS Reporting and most applicable
subcategory
866
‐
837
‐
4357
(866
‐
UDS
‐
HELP)
EHBs account and user
access questions
Health Center
Program Support
BPHC Contact Form
Select: Technical Support, EHBs
Tasks/Technical Issues, EHBs Privileges
877
‐
464
‐
4772
EHBs technical issues
with UDS Reports
Health Center
Program Support
BPHC Contact Form
Select: Technical Support, EHBs
Tasks/Technical Issues, Other EHBs
Submission Types
877
‐
464
‐
4772
UDS+ FHIR R4 IG and
API (UDS Modernization)
technical support
Health Center
Program Support
BPHC Contact Form
Select: UDS Modernization
877
‐
464
‐
4772
Other data and resource links, including this manual, a complete set of the UDS tables and forms (note that the
table view within EHBs may look different but contains the same fields), notifications of changes to reporting
criteria, training opportunities, and other reporting materials and guidance, can be found on the
BPHC UDS
training and technical assistance website, the Primary Health Care Digest, or the UDS Modernization Initiative
page.
Strategic partnerships, including health center-controlled networks, national cooperative agreements, primary care
associations, and primary care offices, can be found on the BPHC Strategic Partnerships webpage
.
Resources are available to assist health centers serving special populations and other vulnerable populations with
meeting performance requirements and training needs:
Organization
Website
Contact and Email
Phone
National Association of
Community Health Centers
(NACHC)
http://www.nachc.org
Margaret Davis
mdavis@nachc.com
301-347-0445
PHPC Program
Organization
Website
Contact and Email
Phone
National Nurse-Led Care
Consortium (NNCC)
https://nurseledcare.phmc.org/
Kristine Gonnella
kgonnella@phmc.org
267-350-7632
National Center for Health in
Public Housing (NCHPH)
http://www.nchph.org
Dr. Jose Leon
jose.leon@namgt.com
703-812-8822, ext.
250

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
215 2023 UDS MANUAL | Appendix H
MHC Program
Organization
Website
Contact and Email
Phone
Farmworker Justice (FJ) https://www.farmworkerjustice.org/
Alexis Guild
aguild@farmworkerjustice.
org
202-372-7422
Health Outreach Partners
(HOP)
http://outreach-partners.org/
Cynthia Selmi
cynthia@outreach-
partners.org
925-788-9723
MHP Salud http://mhpsalud.org/
Shannon Patrick
spatrick@mhpsalud.org
956-968-3600, ext.
2033
Migrant Clinicians Network
(MCN)
http://www.migrantclinician.org
Theressa Lyons-Clampitt
tlyons@migrantclinician.
org
512-579-4511
National Center for
Farmworker Health (NCFH)
http://www.ncfh.org
Sylvia Partida
partida@ncfh.org
512-312-5457
HCH Program
Organization
Website
Contact and Email
Phone
Corporation for Supportive
Housing (CSH)
http://www.csh.org
Jamie Blackburn
978-457-1443
National Health Care for the
Homeless Council (NHCHC)
http://www.nhchc.org
Dr. Alaina Boyer
aboyer@nhchc.org
615-226-2292
Other Vulnerable Populations and Supports
Organization
Website
Contact and Email
Phone
Association of Asian Pacific
Community Health
Organizations (AAPCHO)
http://www.aapcho.org
John Nguyen-Yap
jnguyenyap@aapcho.org
510-545-9372
Association of Clinicians for
the Underserved (ACU)’s
STAR² Center (Recruitment
and Retention)
http://www.clinicians.org/
Suzanne Speer
sspeer@clinicians.org
703-577-1206
Capital Link (Capital
Development and Growth)
http://www.caplink.org/
Meredith Tzouros
mtzouros@caplink.org
617-422-0350, ext.
2213
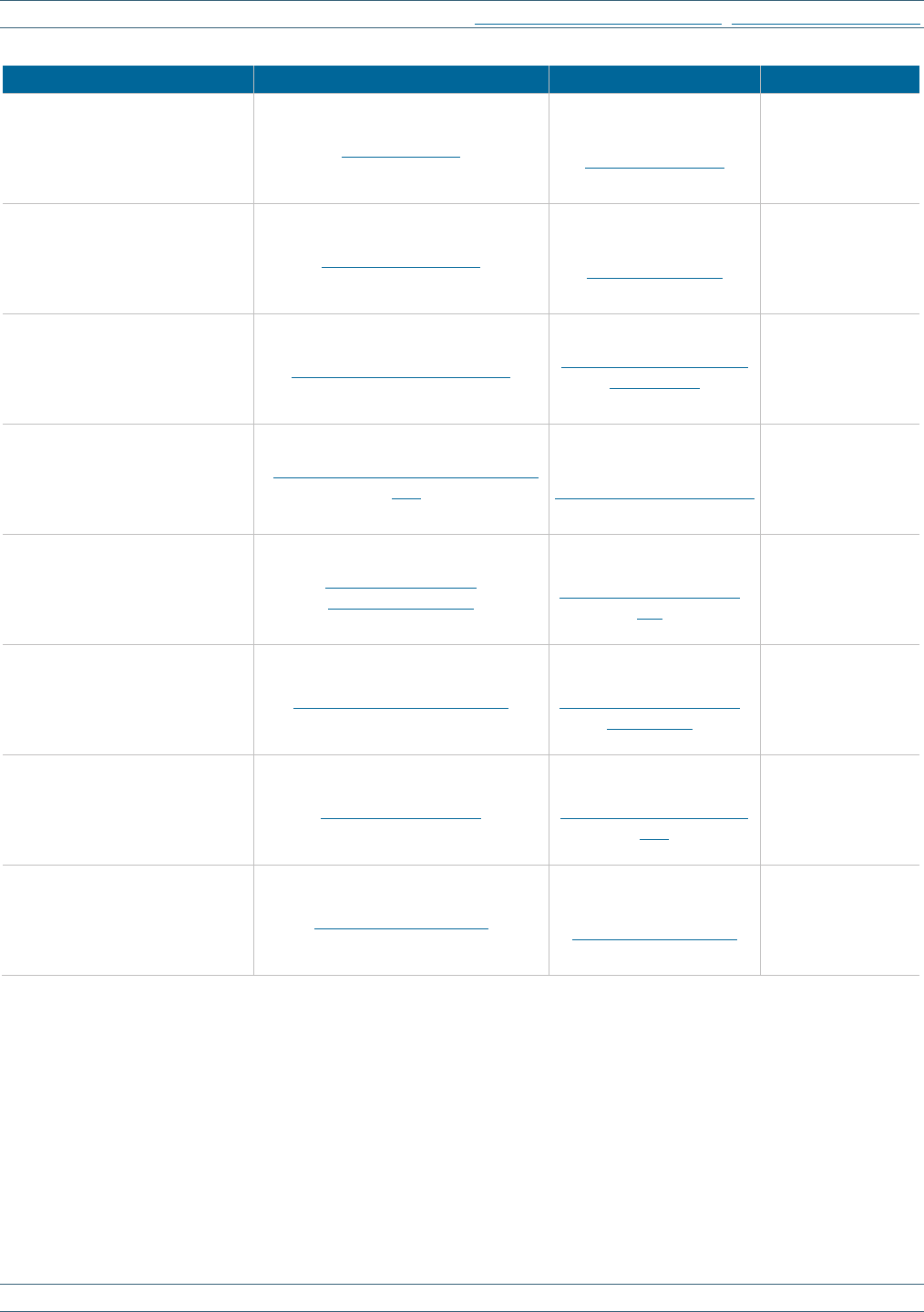
UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
216 2023 UDS MANUAL | Appendix H
Organization
Website
Contact and Email
Phone
Community Health Center, Inc.
(CHC)/Weitzman Institute
(Workforce Development)
http://chc1.com/
Amanda Schiessl
860-266-8665
Health Information and
Technology, Evaluation and
Quality (HITEQ) Center
http://hiteqcenter.org/
Jillian Maccini
844-305-7440
Health Partners on IPV +
Exploitation
https://healthpartnersipve.org/
Anna Marjavi
amarjavi@futureswithout
violence.org
415-678-5502
National LGBTQIA+ Health
Education Center
https://www.lgbtqiahealtheducation.
org/
Dr. Alex Keuroghlian
617-927-6064
National Center for Medical-
Legal Partnership (NCMLP)
http://www.medical-
legalpartnership.org
Bethany Hamilton, JD
bhamilton1@email.gwu.
edu
202-994-0905
National Center for Equitable
Care for Elders (NCECE)
https://ece.hsdm.harvard.edu/
Christine Riedy-Murphy
Christine_Riedy@hsdm.
harvard.edu
617-432-5251
National Network for Oral
Health Access (NNOHA)
http://www.nnoha.org
Phillip Thompson
executivedirector@nnoha
.org
303-957-0635, ext.
6
School-Based Health Alliance
(SBHA)
http://www.sbh4all.org/
Dannielle Dobbins
ddobbins@sbh4all.org
202-370-4391

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
217 2023 UDS MANUAL | Appendix H
UDS PRODUCTION TIMELINE AND REPORT AVAILABILITY
Health centers can access their current-year and prior-year UDS Reports, as well as several standard reports,
through the EHBs web link
.
• UDS Preliminary Reporting Environment (PRE): October–December 2023
• UDS annual data collection and reporting: January 1–February 15, 2024
• Deadline for submitting a complete UDS Report: February 15, 2024
• UDS reporting freeze: March 31, 2024
• Standard UDS Reports are available in EHBs, as shown below.
o Release of UDS Rollup Reports, Awardee and Look-Alike Profiles, and Awardee Comparison Data
Views will be available on the HRSA Data Warehouse
in August 2024.
o Service area data will be available on the HRSA Data and Reporting website in August 2024.
UDS Report
Level
Timing Description Awardee
Look-
Alike
Finalized Health
Center Tables and
XML Data File
June
Provides health center with data for each of the 11
UDS tables, the HIT, Other Data Elements, and
Workforce forms
HC HC
Health Center
Trend Report
July/August
Compares the health center’s performance for key
measures (in three categories: Access, Quality of
Care/Health Outcomes, and Financial Cost/Viability)
with national and state averages over a 3-year period
HC, S, N HC, N
UDS Summary
Report
July/August
Summarizes and analyzes the health center’s current
UDS data using measures across various tables of the
UDS Report
HC, S, N HC, N
UDS Rollup
Report
July/August
Compiles annual data reported by health centers and
provides summary data for patient characteristics,
socioeconomic characteristics, staffing, patient
diagnoses and services rendered, quality of care,
health outcomes and disparities, financial costs, and
revenue
S, N N
Performance
Comparison
Report
September
Summarizes and analyzes the health center’s latest
UDS data, giving details at awardee, state, national,
urban, and rural levels with trend comparisons and
percentiles
HC, S, N HC, N
Abbreviations indicate geographies and detail level for which each report is available.
HC=Health Center, S=State, N=National

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
218 2023 UDS MANUAL | Appendix H
UDS CQMS AND NATIONAL PROGRAMS CROSSWALK
The following table crosswalks the UDS CQMs and other national programs using these measures. Specification
details and eCQM flowsheets are available at the eCQI Resource Center. Use the
Office of National Coordinator
Issue Tracking System to report issues or ask questions about eCQM specifications.
ID Measure Title
Measure
Steward
CMS
eCQM
NQF
#
CMS
Medicaid
Core Set
Healthy People
2030
MIPS/
QPP
Table
6B,
Line 7
Early Entry to
Prenatal Care
n/a n/a n/a n/a MICH-08 No
Table
6B,
Line 10
Childhood
Immunization
Status
National
Committee for
Quality
Assurance
CMS117v
11
38 Child Core n/a Yes
Table
6B,
Line 11
Cervical Cancer
Screening
National
Committee for
Quality
Assurance
CMS124v
11
32 Adult Core C-09 Yes
Table
6B,
Line
11a
Breast Cancer
Screening
National
Committee for
Quality
Assurance
CMS125v
11
2372 Adult Core C-05 Yes
Table
6B,
Line 12
Weight
Assessment and
Counseling for
Nutrition and
Physical Activity
for Children/
Adolescents
National
Committee for
Quality
Assurance
CMS155v
11
24 Child Core n/a Yes
Table
6B,
Line 13
Preventive Care
and Screening:
Body Mass Index
(BMI) Screening
and Follow-Up
Plan
Centers for
Medicare &
Medicaid
Services
CMS69v11
421e n/a n/a Yes
Table
6B,
Line
14a
Preventive Care
and Screening:
Tobacco Use:
Screening and
Cessation
Intervention
Physician
Consortium for
Performance
Improvement
CMS138v
11
28e Adult Core n/a Yes
Table
6B,
Line
17a
Statin Therapy
for the Prevention
and Treatment of
Cardiovascular
Disease
Centers for
Medicare &
Medicaid
Services
CMS347v
6
n/a n/a n/a Yes
Table
6B,
Line 18
Ischemic Vascular
Disease (IVD):
Use of Aspirin or
Another
Antiplatelet
National
Committee for
Quality
Assurance
CMS164v
7 (no
updated
eCQM)
68 n/a n/a No
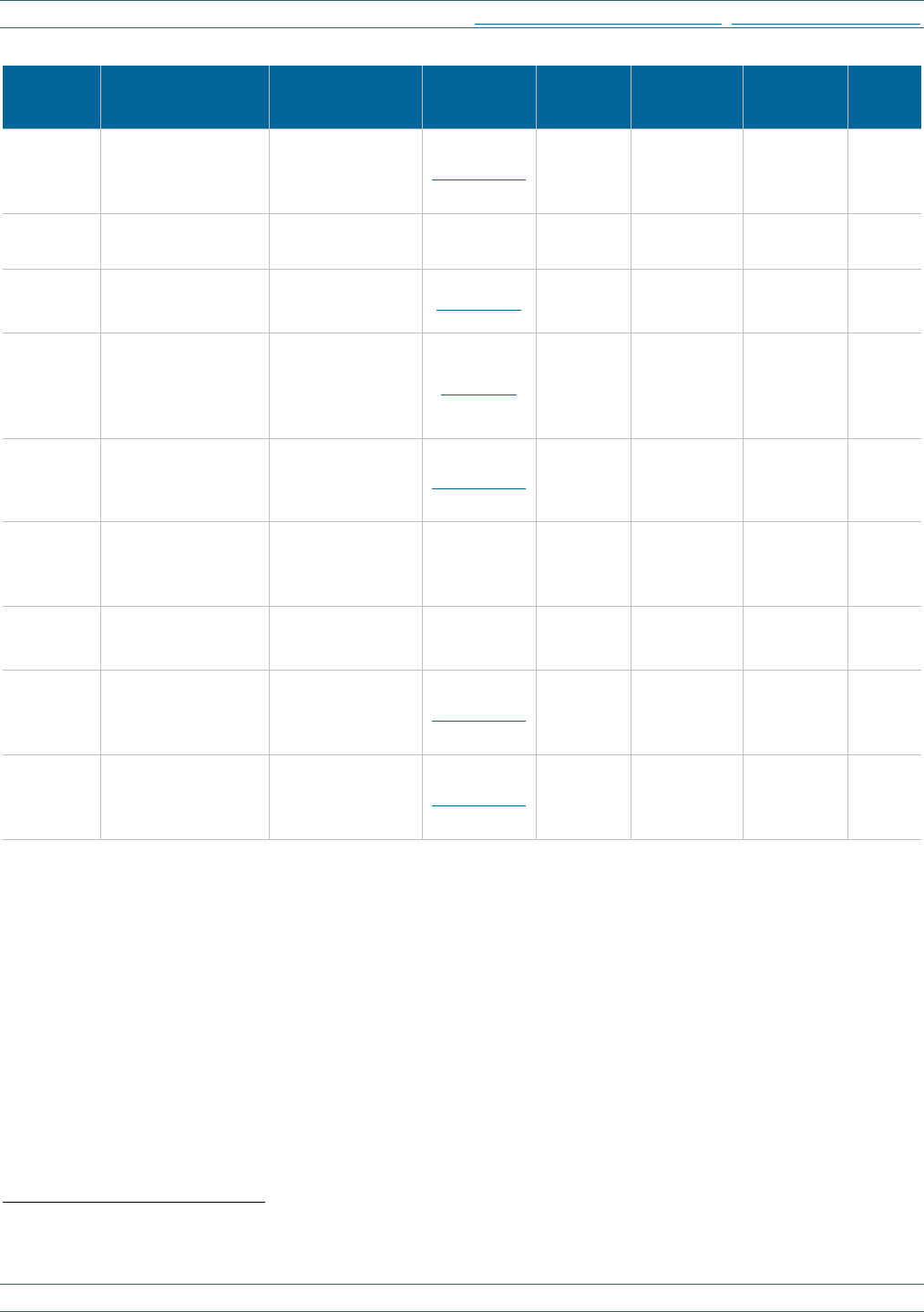
UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
219 2023 UDS MANUAL | Appendix H
ID Measure Title
Measure
Steward
CMS
eCQM
NQF #
CMS
Medicaid
Core Set
Healthy
People
2030
MIPS/
QPP
Table 6B,
Line 19
Colorectal Cancer
Screening
National
Committee for
Quality
Assurance
CMS130v11 34 n/a C-07 Yes
Table 6B,
Line 20
HIV Linkage to
Care
n/a n/a n/a n/a HIV-04 No
Table 6B,
Line 20a
HIV Screening
Centers for
Disease Control
and Prevention
CMS349v5 n/a n/a n/a Yes
Table 6B,
Line 21
Preventive Care
and Screening:
Screening for
Depression and
Follow-Up Plan
Centers for
Medicare &
Medicaid
Services
CMS2v12
418e Adult Core MHMD-08 Yes
Table 6B,
Line 21a
Depression
Remission at
Twelve Months
Minnesota
Community
Measurement
CMS159v1
1 710e n/a n/a Yes
Table 6B,
Line 22
Dental Sealants for
Children between
6–9 Years
Dental Quality
Alliance -
American Dental
Association
CMS277
(no updated
eCQM)
29
2508
(claims-
based
measure)
Child Core OH-10 No
Table 7,
Section A
Low Birth Weight
Centers for
Disease Control
and Prevention
n/a 1382 n/a n/a No
Table 7,
Section B
Controlling High
Blood Pressure
National
Committee for
Quality
Assurance
CMS165v11 18 Adult Core HDS-05 Yes
Table 7,
Section C
Diabetes:
Hemoglobin A1c
(HbA1c) Poor
Control (>9%)
National
Committee for
Quality
Assurance
CMS122v11 59 Adult Core D-03 Yes
n/a = Not applicable, NQF = National Quality Forum, MIPS = Merit-based Incentive Payment System, QPP = Quality Payment Program
29
Contact the UDS Support Center to access measure details.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET, BPHC CONTACT FORM
220 2023 UDS MANUAL | Appendix I
Appendix I: Glossary
Accrual basis: Method of accounting that recognizes income when it is earned and expenses when they are
incurred.
Adjustment: The difference between the health center fee schedule charge and the amount to be reimbursed by a
payer for any given patient service transaction. There may be multiple adjustments on a single transaction.
Aged and disabled former migratory agricultural workers: As defined in section 330 (g)(1)(B), individuals
who have previously been migratory agricultural workers but who no longer work in agriculture because of their
age or disability.
Bad debt (self-pay): Amounts owed by a patient that the health center has determined to be uncollectable and
written off.
Capitation: An agreed-upon amount that a managed care payer pays to the provider (health center) for providing
all of the services in an agreed-upon list. The payer/HMO pays the health center a set amount monthly, regardless
of the number of services or if any services were rendered during the month.
Cash basis: Method of accounting that recognizes income when the payment is received and expense when cash
is disbursed.
Change in accounts receivable: Charges minus collections minus adjustments, or the amount by which what is
owed to the health center increases or decreases during the calendar year.
CHIP: The Children’s Health Insurance Program (CHIP) is a federally funded program that provides primary
health care coverage for children and, on a state-by-state basis, others, especially pregnant patients, mothers, or
parents of these children. CHIP coverage can be provided through the state’s Medicaid program, contracts with
private insurance plans, or both.
Clinical quality language (CQL): A Health Level Seven International (HL7) authoring language standard
intended to be human readable.
Clinical quality measure (CQM): A quantified indicator used to evaluate how well the health center is achieving
standards.
Contracted personnel: People who work under contract for the health center, as opposed to being a salaried
employee. They DO NOT have withholding taxes deducted from their paychecks, and they have their income
reported to the Internal Revenue Service (IRS) on a 1099 form.
Cost center: Unit of the health center’s business where costs associated with that unit are charged and
accumulated for accounting purposes.
Countable visit: A documented encounter in the patient health record between a patient and a licensed or
credentialed provider who exercises their independent professional judgment in the provision of services to the
patient. (Virtual visits are allowable for each of the service categories.)
Denominator: The number below the line in a fraction, or the divisor. As used in clinical quality measure
reporting, patients who fit the detailed criteria described for inclusion in the specific measure to be evaluated.
Draw down: The amount of grant dollars in cash transferred by HHS to the health center in response to a formal
request for awarded grant funds.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET
221 2023 UDS MANUAL | Appendix I
Dually eligible: A patient enrolled in both Medicare and Medicaid, with Medicare being the primary insurance.
Electronic health record (EHR)/Electronic medical record (EMR)/Patient health record: A digital record of
a patient’s registration profile, the history of services provided, diagnostic results, and other patient information. It
often includes a web-based communications portal for patients and providers. The record information is made
available securely to authorized users.
Ethnicity: The ethnic ancestry or origin of a person or group of people.
Exclusions or exceptions: As used in clinical quality measure reporting, patients NOT to be considered or
included in the denominator (exclusions) or removed if a specific condition is identified (exceptions).
Federal poverty guidelines: An annual notice issued by HHS of the annual income thresholds, defined by the
number of persons in the family/household, at or under which individuals are defined as being in poverty. Three
separate schedules are issued for people residing in the 48 contiguous states and the District of Columbia, in
Alaska, and in Hawaii. Health centers in U.S. territories may use the 48 contiguous state schedule.
Fee-for-service: A method of charging for services and paying reimbursements to providers based upon the
charge for procedures, visits, or other services rendered.
Fee schedule: A listing of the health center’s uniform charges for its goods and services.
First trimester (prenatal care): Patients who are estimated to be pregnant up through the end of the 13
th
week
after the first day of their last menstrual period.
Full-time equivalent (FTE): The fraction of time an individual is paid during the calendar year. Full-time (as
defined by the health center) is equal to 1.00 FTE (and half-time is equal to 0.50 FTE, and so on).
Full-time personnel: People generally employed 40 hours per week, but subject to organizational definitions.
Full-time personnel generally receive benefits, have withholding taxes deducted from their paychecks, and have
their income reported to the IRS on a W-2 form. Personnel may or may not have a contract. Personnel are full-
time when they are so defined in their contract and/or when their benefits reflect this status.
Gender identity: An individual’s internal sense of their gender as a male, female, a combination of male and
female, or another gender. This may or may not align with one’s assigned sex at birth.
Gross charges: The sum of the full, undiscounted health center fees for a product or a service rendered.
Hispanic, Latino/a, or Spanish origin: Describes individuals of specific Spanish or Latino/a heritage, lineage,
descent, or country of birth.
Homeless: An individual experiencing homelessness is a person who lacks housing (without regard to whether
the individual is a member of a family), including individuals whose primary residence during the night is at a
location classified as unfit for human habitation (e.g., street, field, abandoned building), a supervised public or
private facility that provides temporary living accommodations, a day-to-day temporary and unstable living
arrangement in someone else’s home (doubled up), in transitional housing, or in permanent supportive housing.
May include children and youth at risk of homelessness, homeless veterans, and veterans at risk of homelessness.
Income: Money received through earnings from work and other sources.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET
222 2023 UDS MANUAL | Appendix I
Indigent care programs: State or local programs that earmark dollars to pay in whole or in part for services
rendered to people who are uninsured and experiencing poverty. Indigent care programs include 638 compact
programs for tribal groups.
Last party rule: Reporting of grant and contract cash receipts based on the entity from which the health center
received them, rather than the source from which they originated.
Locum tenens: People who work at the health center on an as-needed basis during a part-time absence of another
individual, when the health center is unable to hire full- or part-time personnel until the position is filled, or to
serve during a period of increased demand. Locums are uniquely identifiable because they work for an agency and
the health center pays the agency rather than the individual. They DO NOT receive benefits from the health center
(although they may from the agency they work for) and generally are not covered by the health center’s
professional liability insurance.
Look-alike: A designation by HRSA of a health center that meets the requirements of a Federally Qualified
Health Center but does not receive Health Center Program section 330 funding.
Managed care: A system in which a premium is paid under contract to a health center by a private or public
organization to provide a defined range of services to patients assigned to the health center.
Measurement period: The time period (defined by start and end dates) for which a clinical quality measure
applies.
Medicaid: Joint federal/state-run programs operating under the guidelines of Titles XIX (Medicaid) and XXI
(CHIP, as appropriate) of the Social Security Act.
Medicaid expansion: A program created by the Affordable Care Act that makes Medicaid available to more
patients in each state and that requires the state to opt in to participate.
Medicare: Federal health insurance program for people 65 years of age or older, people with blindness, people
with a disability, and people with end-stage renal disease (Title XVIII of the Social Security Act).
Member month: One individual enrolled in a managed care plan for one month.
Migratory agricultural workers: For the purposes of health centers receiving a Health Center Program award or
designation under section 330(g) of the Public Health Service Act, individuals whose principal employment is in
agriculture, who have been so employed within 24 months of their first visit of the calendar year being reported,
and who establish for the purposes of such employment a temporary abode. This includes the family members
(who themselves may or may not migrate) of the individuals described above and individuals who are no longer
employed in migratory agriculture because of age or disability.
National Health Service Corps (NHSC) assignees: Clinicians who either received an NHSC scholarship or are
receiving NHSC loan repayment who are obligated to repay that support by serving at an approved facility in a
designated health professional shortage area.
New Access Point: A health center’s newly approved service delivery site.
Numerator: The number that is above the line in a fraction and is divided by the denominator. As used in clinical
quality measure reporting, patient health records (a subset of the denominator) that meet the criteria for the
specified measure.
Off-site contract providers: Providers who are contracted to provide services to referred health center patients at
locations other than the health center’s approved service delivery sites.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET
223 2023 UDS MANUAL | Appendix I
Part-time personnel: People employed for a period less than what the health center defines as full-time. They
receive benefits as specified by the health center’s policy, have withholding taxes deducted from their paychecks,
and have their income reported to the IRS on a W-2 form. Part-time personnel may or may not have a contract.
Patient: An individual who has at least one countable visit during the calendar year in one or more categories of
services: medical, dental, mental health, substance use disorder, vision, other professional, or enabling.
Patient service revenue: The revenue attributable to the provision of patient services within the scope of federal
project.
Penalty/paybacks: Payments made by health centers to refund overpayments, or payments due to failure to meet
utilization or other performance goals required by the payer.
Prenatal care (first visit): The first date a patient has a visit with a physician, NP, PA, or CNM who conducts a
comprehensive prenatal exam to initiate pregnancy-related health care.
Public housing: Public housing agency-developed, owned, or assisted low-income housing, including mixed-
finance projects but excluding housing units with no public housing agency support other than Section 8 housing
vouchers.
Race: A physical or social categorization of an individual, presumably based on inheritance or genetics.
Reclassify: Transfer of amounts due from one payer to another payer, including the patient.
Reconciliations: Lump-sum retroactive adjustments based on the filing of a settlement report.
Residents/trainees: Individuals in training for a license or certification who provide services at the health center
under the supervision of a more senior individual. Many of these trainees (especially medical and dental residents)
already have licenses.
School-based service site: A health center located on school grounds (including pre-school, kindergarten, and
primary through secondary schools) that provides health services.
Screening: A test to check for a disease or health condition in the absence of signs and symptoms. Screening tests
DO NOT diagnose illness, and those who test positive typically require additional evaluation with diagnostic tests
or procedures.
Seasonal agricultural workers: For the purposes of health centers receiving a Health Center Program award or
designation under section 330(g) of the Public Health Service Act, individuals whose principal employment is in
agriculture on a seasonal basis and who DO NOT meet the definition of a migratory agricultural worker.
Second trimester (prenatal care): Patients who were pregnant and estimated to be between the start of the 14th
week and the end of the 27th week after the first day of their last menstrual period.
Self-pay: A type of payment (in whole or in part) that is NOT directly paid by a third-party payer to the health
center for services provided to a patient.
Sex: The anatomical and physiological biology of an individual assigned at birth.
Sexual orientation: How an individual describes their emotional and sexual attraction to others, such as straight,
lesbian, gay, bisexual, or another sexual orientation.
Sliding fee discount: A discount applied to the fee schedule that adjusts fees based on the patients’ ability to pay
based on their income and family/household size.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET
224 2023 UDS MANUAL | Appendix I
Standing order: Written protocol that authorizes designated members of the health care team (e.g., nurses) to
complete certain clinical tasks without having to first obtain a physician or advanced practice provider order.
Third trimester (prenatal care): Patients who were estimated to be pregnant for 28 weeks or longer after the
first day of their last menstrual period.
Third-party payer: An insurer or other entity that reimburses the health center for services rendered to patients.
Veteran: Discharged individuals who served in the active military, naval, or air service, which includes the Air
Force, Army, Coast Guard, Marines, Navy, and Space Force, or as a commissioned officer of the Public Health
Service or National Oceanic and Atmospheric Administration. This also includes individuals who served in the
National Guard or Reserves on active duty status.
Volunteers: Individuals who work at the health center but are NOT paid for their work.
Wraparound payments: Periodic payments to FQHCs to reimburse the shortfall between the amounts paid by
the payer and the health center’s established FQHC or PPS visit rate.

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET
225 2023 UDS MANUAL | Appendix J
Appendix J: Acronyms
• AAPCHO: Association of Asian Pacific
Community Health Organizations
• ACO: accountable care organization
• ADA: American Dental Association
• ADHC: adult day health care
• AMA: American Medical Association
• AMI: acute myocardial infarction
• API: application programming interface
• APN: advanced practice nurse
• ASCVD: atherosclerotic cardiovascular
disease
• AWP: average wholesale price
• BCCEDP: Breast and Cervical Cancer Early
Detection Program
• BDI, BDI-II: Beck Depression Inventory
• BDI-PC: Beck Depression Inventory-Primary
Care
• BHW: Bureau of Health Workforce
• BMI: body mass index
• BP: blood pressure
• BPHC: Bureau of Primary Health Care
• CABG: coronary artery bypass graft
• CAD-MDD: Computerized Adaptive
Diagnostic Test for Major Depressive
Disorder
• CADRE: Capital Assistance for Disaster
Response and Recovery Efforts
• CARE: Capital Assistance for Hurricane
Response and Recovery Efforts
• CASA: Clinic Assessment Software
Application
• CAT-DI: Computerized Adaptive Testing
Depression Inventory
• CCO: coordinated care organizations
• CDC: Centers for Disease Control and
Prevention
• CEO: chief executive officer
• CES-D: Center for Epidemiologic Studies
Depression Scale
• CFO: chief financial officer
• CHC: Community Health Center (program)
• CHIP: Children’s Health Insurance Program
• CIO: chief information officer
• CIS: change in scope
• CME: continuing medical education
• CMO: chief medical officer
• CMS: Centers for Medicare & Medicaid
Services
• CNM: certified nurse midwife
• COO: chief operations officer
• COVID-19: coronavirus disease 2019
• CPT: Current Procedural Terminology
• CQL: Clinical Quality Language
• CQM: clinical quality measure
• CSDD: Cornell Scale for Depression in
Dementia
• CSH: Corporation for Supportive Housing
• CT: computerized tomography
• DADS: Duke Anxiety-Depression Scale
• DATA: Drug Addiction Treatment Act of
2000
• DEPS: Depression Scale
• DGMO: Division of Grants Management
Operations
• DNA: deoxyribonucleic acid
• DO: Doctor of Osteopathic Medicine
• DRE: digital rectal exam
• DT, DTaP, DTP: diphtheria, tetanus, pertussis
• eCQI: Electronic Clinical Quality
Improvement

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET
226 2023 UDS MANUAL | Appendix J
• eCQMs: electronic-specified clinical quality
measures
• EHBs: Electronic Handbooks
• EHR: electronic health record
• EKG: electrocardiogram
• EMR: electronic medical records
• EMS: emergency medical service
• EMT: emergency medical technician
• ENDS: electronic nicotine delivery systems
• EPSDT: Early and Periodic Screening,
Diagnostic, and Treatment
• ESRD: end-stage renal disease
• FAQ: frequently asked question
• FDA: U.S. Food and Drug Administration
• FHIR R4: Fast Healthcare Interoperability
Resources forth digital standards release
• FIT: fecal immunochemical test
• FOBT: fecal occult blood test
• FPG: federal poverty guidelines
• FQHC: Federally Qualified Health Center
• FTC/TAF: emtricitabine/tenofovir
alafenamide
• FTC/TDF: emtricitabine/tenofovir disoproxil
fumarate
• FTE: full-time equivalent
• GAAP: generally accepted accounting
principles
• GDS: Geriatric Depression Scale
• gFOBT: guaiac fecal occult blood test
• HAM-D: Hamilton Rating Scale for
Depression
• HbA1c: Hemoglobin A1c
• HCFA: Health Care Financing Administration
• HCH: Health Care for the Homeless
(program)
• HCPCS: Healthcare Common Procedure
Coding System
• HEDIS: Healthcare Effectiveness Data and
Information Set
• HHS: U.S. Department of Health and Human
Services
• Hib: haemophilus influenza B
• HIT: health information technology
• HITEQ: Health Information Technology,
Evaluation, and Quality Center
• HIV: human immunodeficiency virus
• HL7: Health Level Seven
• HMO: health maintenance organization
• HPV: human papillomavirus
• HR: human resources
• HRSA: Health Resources and Services
Administration
• HUD: U.S. Department of Housing and Urban
Development
• ICD: International Classification of Diseases
• iFOBT: immunochemical-based fecal occult
blood test
• IG: Implementation Guide
• IHS: Indian Health Service
• IPV: inactivated polio vaccine
• IRS: Internal Revenue Service
• IT: information technology
• IVD: ischemic vascular disease
• LAL: look-alike
• LBW: low birth weight
• LCSW: licensed clinical social worker
• LDL-C: low-density lipoprotein cholesterol
• LGBTQIA+: lesbian, gay, bisexual,
transgender, queer, intersex, asexual, and all
sexual and gender identities
• MCN: Migrant Clinicians Network

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET
227 2023 UDS MANUAL | Appendix J
• MCO: managed care organization
• MD: medical doctor
• MFQ: Mood Feeling Questionnaire
• MHC: Migrant Health Center (program)
• MIPS: Merit-based Incentive Payment System
• MMR: measles, mumps, and rubella
• MOUD: Medications for opioid use disorder
• NACHC: National Association of Community
Health Centers
• NAICS: North American Industry
Classification System
• NAP: New Access Point
• NCFH: National Center for Farmworker
Health
• NCHPH: National Center for Health in Public
Housing
• NCHS: National Center for Health Statistics
• NHCHC: National Health Care for the
Homeless Council
• NHSC: National Health Service Corps
• NNCC: National Nurse-Led Care Consortium
• NP: nurse practitioner
• NQF: National Quality Forum
• OB/GYN: obstetrician/gynecologist
• OMB: Office of Management and Budget
• OMH: Office of Minority Health
• ONC: Office of the National Coordinator for
Health IT
• P4P: pay for performance
• PA: physician assistant
• PACE: Program of All-Inclusive Care for the
Elderly
• PAL: Program Assistance Letter
• PAP: pharmacy assistance program
• PCCM: primary care case management
• PC-DMIS: personal computer dimensional
measurement inspection software
• PCI: percutaneous coronary intervention
• PCMH: patient-centered medical home
• PCV: pneumococcal conjugate
• PDMP: Prescription Drug Monitoring
Program
• PDS: pharmacy dispensing software
• PDSA: plan, do, study, act
• PECS: patient electronic care system
• PHPC: Public Housing Primary Care
(program)
• PHQ: Patient Health Questionnaire
o PHQ-9M: PHQ modified for teens
o PHQ-A: PHQ for adolescents
• PHS: Public Health Service (Act)
• PMPM: per member per month
• PMS: Payment Management System (PMS-
272)
• PPD: purified protein derivatives
• PPS: prospective payment system
• PRAPARE: Protocol for Responding to and
Assessing Patients’ Assets, Risks, and
Experiences
• PRE: Preliminary Reporting Environment
• PrEP: pre-exposure prophylaxis
• PRIME MD: Primary Care Evaluation of
Mental Disorders
• PSC-17: Pediatric Symptom Checklist
• PTSD: post-traumatic stress disorder
• QI: quality improvement
• QID-SR: Quick Inventory of Depressive
Symptomology Self-Report
• RBRVU: resource-based relative value unit
• RN: registered nurse
• RV: rotavirus

UDS SUPPORT CENTER, 866-UDS-HELP, UDSHELP330@BPHCDATA.NET
228 2023 UDS MANUAL | Appendix J
• SAMHSA: Substance Abuse and Mental
Health Services Administration
• SARS-CoV-2: strain of severe acute
respiratory syndrome-related coronavirus
• SBIRT: Screening, Brief Intervention, and
Referral to Treatment
• SNAP: Supplemental Nutrition Assistance
Program
• SRO: single-room occupancy
• SSI: Supplemental Security Income
• TAF/FTC: tenofovir
alafenamide/emtricitabine
• TANF: Temporary Assistance for Needy
Families
• TDF/FTC: tenofovir disoproxil
fumarate/emtricitabine
• UCR: usual, customary, and reasonable
• UDS: Uniform Data System
• UDS+: Uniform Data System De-Identified
Patient-Level Submission
• USHIK: United States Health Information
Knowledgebase
• VFC: Vaccines for Children (program)
• VSAC: Value Set Authority Center
• VZV: varicella zoster virus
• WE CARE: Well Child Care, Evaluation,
Community Resources, Advocacy Referral,
Education
• WIC: Women, Infants, and Children
(program)

2023 UDS Manual—May 8, 2023
OMB Number: 0915-0193
Expiration Date: 04/30/2026
