
Sample Case Study
1
Relevant History
XX, a 78-year-old, right-handed female, was hospitalized in early February of 2014 due to a possible
ischemic stroke. Per review of the medical record, she awoke at 4 a.m. with left facial, perioral and left hand
numbness and tingling. She also reported weakness in her left upper and lower extremity, and decreased left-
sided peripheral vision in her left eye. She presented to a community hospital where the initial CT scan was
reportedly negative for acute processes. Symptoms reportedly progressed to include difficulty with ambulation,
and XX was transferred to a JCAHO-certified stroke center for continued care.
Magnetic resonance imaging completed upon admission to the stroke center revealed a right posterior
cerebral infarction greater than 8 hours of age. Areas of involvement included the right occipitotemporal gyrus,
the right occipital lobe, the posterior body and tail of the right hippocampus, and the right thalamus within the
distribution of the right posterior cerebral artery, resulting from thrombosis at the P1-P2 juncture. Images are
included for consideration in Appendix A. A computerized tomography angiogram (CTA) was completed,
confirming occlusion of the P1 segment of the posterior cerebral artery. Medical workup revealed left-sided
paresthesia and diminished strength, without “aphasia or facial droop”, and cranial nerve (CN) examination
revealed functions for CNs II – XII to be grossly intact. XX was reported to be oriented, with congruent mood
and affect. No acute cardiac, respiratory or gastrointestinal processes were identified. XX was placed on deep
vein thrombosis prophylaxis of aspirin and Lovenox® injections daily, along with the statin medication, Lipitor®
for management of hyperlipidemia, and Ambien® for insomnia. Referrals for physical, occupational and speech
therapy were initiated in the acute care setting, but service was limited to completion of evaluations only, as XX
met criteria for transfer to the comprehensive inpatient rehabilitation (IRF) setting. She was admitted to the IRF
only two days following hospitalization, and rehabilitation care continued in that setting for a period of 21 days.
XX was a high school graduate, with English as her only language. Her occupation was listed as
homemaker. Prior to hospitalization for this medical event, XX lived independently, drove and volunteered in
her church. She had two supportive daughters. Her prior medical history was limited to diagnoses of

Sample Case Study
2
hyperlipidemia and back pain, and family history was positive for cerebrovascular accident in both parents. The
only medication taken at home was Allegra-D®.
2) Assessment Methods/Tests & Results
The standardized assessment selected for use during XX’s evaluation in the inpatient rehabilitation
setting was the Burns Brief Inventory of Communication and Cognition: Right Hemisphere Inventory. This is a
criterion-referenced tool designed to provide a profile of strengths and challenges across a range of skills and
behaviors associated with injury to the right, cerebral hemisphere (Burns, 1997), which is generally considered
the non-dominant hemisphere with respect to speech and language functioning (Bhatnager, 2012). The tool had
the ability to efficiently provide a measure of non-linguistic attentional functioning and visual-perception, and
the extralinguistic skills of prosody and abstract language, all of which are frequently targets of intervention by
speech-language pathology for individuals who experience right hemisphere lesions (Myers and Blake, 2008).
The scoring summary for this assessment tool is designed to aid in the selection of relevant treatment activities,
as plotting of raw scores provides a way to quickly identify skills which are relatively intact and not in need of
intervention, as well as skills which are limited to a severe degree, such that focused intervention may be a less
efficient use of resources. Tasks on which performance falls in the range between these two extremes as
indicated by shading or diagonal lines are described as potentially relevant selections for impairment-based
therapy (Burns, 1997).
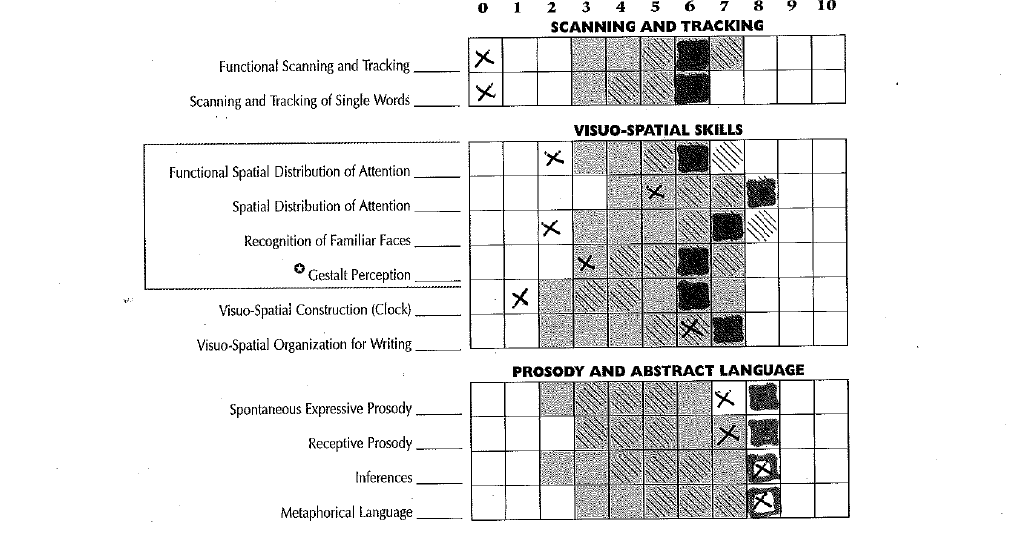
XX’s performance on the initial administration of this tool is shown in Appendix B. Examination of the
scores indicated the presence of moderate to severe difficulties with all activities which required leftward visual
scanning, sustained and/or alternating attention to the left side of table top activities, facial recognition, and
visual-spatial constructional and graphomotor abilities. When confronted with a picture of a mealtime place
setting, she stated that it appeared to her to be “a ball of yarn”. Of the 5 items included on this subtest, she was
only able to locate the one situated farthest to the right side of the scene. Another subtest presented a visual
Sample Case Study
3
closure activity in which XX was asked to name an item drawn in a degraded fashion with dashed lines, such that
pieces were missing. She was able to successfully name only 2 of the 5 items, and verbal responses reflected
significant perceptual difficulties such as referring to a pair of scissors as, “a wooden toy bear leaping in the air”,
and to a desk as “a hairdo”. XX’s initial clock drawing received 10% of available credit on this item as shown in
Appendix C. The drawing reflects multiple errors of omission for numbers typically found on the left side of a
clock, and the “11” and “12” are placed outside the circle. Vague and extraneous placement of hands is also
apparent.
XX’s scores on all items in the Prosody and Abstract Language cluster reveal performance in these areas
to be a relative strength. XX’s discourse reflected generally appropriate rhythm, and intonation, and she
exhibited only mild difficulty in recognizing emotional tone in the speech of others, as assessed by this tool.
The Burns Brief Inventory of Communication and Cognition: Complex Neuropathology Form (Burns,
1997) was also administered in efforts to further determine the quality of XX’s declarative and working memory
functioning. Results are shown below (Figure 1). While XX performed well on tasks which probed declarative
memory abilities, auditory attention and auditory memory, scores on subtests examining attention and memory
in a way that relies on visual processing confirm the deficits of perception and attention previously discussed.

Sample Case Study
4
Figure 1. Burns Brief Inventory of Communication and Cognition: Complex Neuropathology Form results
In conversation, XX did not demonstrate overt verbosity, tangential content or over-personalization
frequently associated with right hemisphere damage (Blake, 2006); however, moderately structured observation
of cognitive-communication functioning conducted during interview did reveal one of the more unusual aspects
of XX’s clinical presentation, this being significantly distorted interpretation of visually-based situations. XX
interpreted the hand-held medication scanner device used by nursing staff to be some type of camera which
was recording her activity. On another occasion, XX reported, “there was a duplicate of this (pointed to her left
thumb) that fell off. I left it on the table. I was afraid to throw it away.” Later, she was found to be sitting in her
wheelchair with a towel wrapped carefully on her lap. She explained that her hands kept falling off, and she had
them collected in the towel. She also reported that “a hand” was grabbing and pinching her, and at first
wondered if it was some kind of “voodoo”. XX’s perceptions regarding her affected left hand and arm may also
Sample Case Study
5
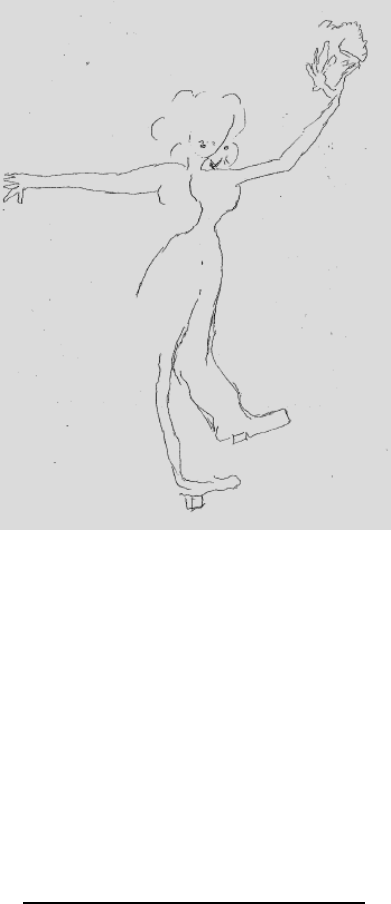
be revealed by the self-portrait drawn during evaluation by the occupational therapist, in which the person
depicted appears to have more than one left hand. (Figure 2).
Figure 2. Self portrait
Lastly, it was noted that oral mechanism examination was unremarkable. No dysphagia was identified
during clinical swallowing examination. XX had no prior history of hearing loss, and hearing acuity in
conversation was judged to be within functional limits.
3) Diagnostic and Prognostic Conclusions
Prognosis for improvement in cognitive-communication function was judged to be good in light of
several factors. XX had relatively limited health concerns prior to hospitalization, as well as with an active,
independent lifestyle, and XX’s family denied any concerns regarding cognitive functioning prior to the CVA.
Another factor in support of a positive prognosis was the fact that XX was still within the two-month window of
Sample Case Study
6
time often referred to as a period of spontaneous recovery (Estabrooks, Martin & Nicholas, 2014).
Furthermore, XX did not deny the presence of deficits once they were explained by the clinician, and she was
stimulable for improved performance on tasks requiring attention to the left hemispace, given visual and verbal
cues. Finally, despite significant changes in her functional ability, XX demonstrated a fairly upbeat, positive
outlook. At one point, when complimented on her sense of humor, she quoted a favorite verse, stating, “A
merry heart doeth good like a medicine.”
Potentially limiting factors were felt to be advanced age, along with the generous size and multilobar
distribution of the cerebrovascular accident. XX’s NIH Stroke Scale Score (NIHSS) upon admission to the hospital
was 9, reflecting the potential for moderately severe impairment (Adams, et al., 1999). Because XX awoke with
stroke symptoms, the time of onset for her CVA could not be determined. For this reason, she did not meet the
criteria to receive thrombolytic treatment (Lansberg, et al., 2012). Thrombolytic treatment has been shown to
improve long-term outcomes for individuals with ischemic stroke (González, et al., 2013; Lindsberg, et al., 2004),
so the fact that XX did not receive this medication may have contributed unfavorably to her outcome. In terms
of prognosis specific to cognitive-communication performance, Cherney and colleagues (2001) found that the
presence and severity of unilateral spatial neglect contributes negatively to outcomes for people recovering
from right hemisphere injury , so the fact that neglect behaviors were present in this case should be considered
in this light.
A differential diagnosis of moderate cognitive-communication deficit of the right hemisphere type was
given at the time of admission to the inpatient rehabilitation setting. The condition is also referred to as “right-
hemisphere syndrome” (Hegde, 2006), and “right hemisphere disorder (RHD)” (Blake, 2008). XX exhibited
greater limitation of non-linguistic than extralinguistic abilities at the time of her initial assessment. This
diagnosis is felt to be supported by site of lesion evidence as well as quantitative and qualitative results from
assessment by the speech-language pathologist. Based on behavioral examination, XX was also believed to

Sample Case Study
7
present with posterior-variant alien hand syndrome (AHS) ( Pack, Stewart, Diamond, & Gale, 2002) based on
diminished recognition of ownership of her left hand without the presence of visual cues, and a perception that
her hand acted in ways outside of her control (Ventura, Goldman & Hildebrand, 1995). Alien hand syndrome
differs from somatoparaphrenia, also common in people with right hemisphere damage, in that
somatoparaphrenia causes a person to deny ownership of the affected limb, even with visual cues. (Gandola, et
al., 2012) An interesting finding relevant to alien hand variants is the report that prognosis for recovery from
posterior variant AHS is believed by some to be better than the prognosis for other variants (Pack, Stewart,
Diamond & Gale, 2002).
4) Management Recommendations and Procedures
Following dynamic assessment of cognitive-communication skills completed within the first 3 days of
admission to the IRF setting, direct intervention by speech-language pathology services addressing cognitive-
communication abilities was recommended for a minimum of 1.0 hours daily on 5 of 7 days each week, for the
remainder of the inpatient rehabilitation stay. XX’s stated goal was to return to her home if at all possible. She
also expressed the desire to be able to read her Bible. Long and short-term goals were developed as follows,
with a focus on establishing skills XX would need in order to return to her home setting with intermittent
supervision from a family member. This level of functioning would allow XX to remain safely in her home alone
for periods of up to 4 hours, but preclude driving or staying in her home alone during nighttime hours.
Long-Term Goals: XX will manage cognitive-communication aspects of her daily routine with intermittent
supervision.
Short-Term Goals:
1) XX will utilize environmental cues and self-initiated strategies to be fully oriented on 3 consecutive
dates.
2) XX will demonstrate improved quality of left attention as demonstrated by comparison of work samples.
Sample Case Study
8
3) XX will punch-dial telephone numbers successfully in 5/5 trials on 3 consecutive dates.
4) XX will complete mock medication management tasks with at least 90% accuracy given extra time and
use of compensatory strategies.
5) XX will be able to read short paragraphs of enlarged print with at least 90% accuracy of comprehension.
6) XX will complete basic route finding activities successfully on at least 2 occasions, given extra time and
assistance upon request.
7) XX will verbalize increased confidence in her cognitive-communicative abilities by date of discharge, as
shown by comparison of responses on a basic visual analog scale.
8) XX’s family will verbalize and demonstrate understanding of XX’s cognitive status and related needs by
the date of discharge from the IRF setting.
The initial session following assessment was designed as an opportunity for XX to learn a bit about the
results of her assessment, and to provide her with a basic summary of brain functioning relative to her stroke.
XX was also told that she was free to question the rationale for any therapy activity, and to request occasional
rest breaks during therapy.
Environmental modifications are described by Barrett (2000) as beneficial in reducing sensory
deprivation in individuals with RHD; therefore, early management activities in this case also included
recommendations regarding XX’s room arrangement in order to facilitate safety and ease of access to
information. Her room was selected so that the doorway would be to her right side when she was in bed, in
order to prevent staff and visitors from surprising her when they entered her room. A clock and calendar were
also placed in a location visible to her right. In the experience of this clinician, mirrors have been observed to
contribute to visual misperception by individuals with RHD, so the full-length mirrored doors in XX’s room were
covered for the duration of her stay. Signs were posted to remind staff to place call light within reach to her left
side, and XX was engaged in practice of call light use until she gave successful and efficient return
demonstration. XX was instructed to treat her affected left arm and hand gently, and to keep her limb in a place
where she could see that it was not vulnerable to being pinched, twisted or otherwise injured.
Sample Case Study
9
Treatment interventions were typically provided in 30 minute sessions scheduled twice to three times daily.
Activities focused heavily on the development of improved visual scanning, with emphasis on the left
peripersonal and extrapersonal space (Warren, 2013; Ward, 2015), and included cancellation, tracing and
copying activities of increasing length and complexity (Warren, 1996). As a precursor, or warm up to these
activities, XX was encouraged to use her left hand to trace the left margin of each array prior to beginning each
graphomotor task. Blake (2007) suggests that such voluntary motor activity with the left hand may increase
right hemisphere activation, resulting in improved attention to the left peripersonal space, and Hillis (2006)
describes this strategy as a way to expand the “window of attention” around a particular stimulus or group of
stimuli. The level of difficulty for these activities was increased by decreasing font size, resulting in an increased
number of potential targets, and by increasing the relative similarity of the visual targets; for example, Ws and
Vs appear more visually similar than Ks and Ts. Computer-assisted activities, including use of the Visual
Attention Therapy app (Tactus Software Solutions, 2012) for iPad®, were incorporated into treatment sessions,
with difficulty level advanced once performance at the 80% accuracy level was achieved. Visual trails,
constructed by placing neon sticky notes with numbers and/or letters, were also used to promote improved
efficiency and accuracy of scanning in the extrapersonal space, similar to the scanning patterns needed for route
finding and driving (Warren, 2013).
Reduced success at the activity level, defined as specific skills or task performance, can result in participation
level limitations which prevent return to desired, age-appropriate roles (WHO, 2002). Because the ability to
obtain help in an emergency situation is one key to being able to live independently, the activity of punch-dialing
telephone numbers was included as a target of intervention, utilizing a phone on which brightly colored tape
was placed to the left side of the keypad. The tape served as a visual “anchor” to the left margin of the keypad
(Meyers, 1999). At baseline, XX performed this activity with less than 50% success, with skill improving to
greater than 80% accuracy level by date of discharge.

Sample Case Study
10
At the outset of treatment, XX was unable to read an analog clock successfully unless both hands indicated
numbers to the right side of the clock, such as “one fifteen”, or “four thirty”. When hands indicated numbers on
the left side of the clock face, XX appeared to interpret the very short extensions of the clock hands in the center
of the clock, and reading 10:10 as “ten after four”, etc. Rubens (1985) found that a medical treatment, referred
to as caloric stimulation, improved visual attention to the neglected side in a group of 18 individuals with
hemineglect. This intervention is conducted by irrigating the left ear canal with cold water, or, in some cases,
using warm water in a similar fashion in the right ear. The beneficial effects are described as being temporary;
however, in an effort to establish an initial successful response and perhaps provide a sensory frame of
reference for leftward scanning, this technique was modified by stroking XX’s left ear (helix, anthelix and
concha) with an iced applicator swab simultaneously with the request to decode clocks on which one or both
hands were pointing to numbers on the left side of the clock. In XX’s case, she was successfully able to read
clocks indicating 9:20 and 6:50 during the first session in which this technique was utilized. Verbal cues to “find
the nine, and then look for the hands” were then paired with all presentations. Once XX was reading the clocks
with 90% success, the iced swab use was discontinued, and XX was instructed to use verbal self-instruction to
direct leftward attention during this task.
It is interesting to note that, at the time this case study is being prepared, both the Practice Portal for the
American Speech-Language-Hearing Association, and the Evidence-Based Practice Guidelines of the Academy of
Neurologic Communication Disorders and Sciences lack specific information relative to the evaluation and
management of right hemisphere cognitive-communicative deficits.
5) Data Documenting Outcomes of Treatment
Within the inpatient rehabilitation setting, the tool known as the Inpatient Rehabilitation Facility-Patient
Assessment Instrument (IRF-PAI) is utilized as the comprehensive measure of functioning and reporting of
outcomes to third-party payers, including the Centers for Medicare and Medicaid Services (UB Foundation

Sample Case Study
11
Activities, 2012). Scoring is based on the set of 18 functional abilities often referred to as the FIM™ instrument
(UDSMR, 2015). The tool utilizes an 8-point descriptive scale rating system, ranging from 0 = “did not occur” to
7= complete independence. XX’s scores on admission to the IRF are shown in dark gray in Figure 3 below.
Scores for the discharge assessment are shown in light gray, and the case-based goal scores are reflected by the
black line.
Figure 3. Polar graph reflecting initial, discharge, and benchmark FIM scores
Key: ◼ = FIM ratings at admission; ◼ = FIM ratings at discharge; line = benchmark at 75
th
percentile
XX’s total FIM gain, calculated by subtracting the total admission FIM score from the total discharge FIM
score, was 16 points, and her length of stay efficiency (LSE), calculated by dividing FIM gain by length of stay was
0.76. In comparison, the average overall FIM gain attained by individuals with similar characteristics was 23.5
points, and the average LSE was 1.4. These lower than average scores may reflect the moderately severe
impairment predicted by the initial NIHSS administration. XX’s score on items in the Cognitive Skills cluster,
including receptive and expressive communication, memory, and problem solving, increased by 2 points. This
change was much smaller than expected based on observed performance of functional activities. It is the
opinion of this clinician that this finding could be related to mis-application of the FIM tool by the rehabilitation
Sample Case Study
12
nursing staff. Additional rational for this assertion, and a discussion of the use of the FIM as a measure of
cognitive-communication performance, will be included in the oral presentation for this case.
Outcomes and functional changes were also documented by comparison of results on the Burns Brief
Inventory of Communication and Cognition: Right Hemisphere Inventory (Burns, 1997) as shown in Appendix B.
Results obtained on the reassessment reflect significant improvement on all subtests involving performance of
visual attention, scanning, visual perception and visuo-spatial construction ability. Scores on tasks assessing
prosody and use of abstract language remained relatively static; however these were initially identified as
relative strengths in comparison to other skills, therefore this finding was not surprising.
Comparison of work samples was also conducted as a measure of improvement. Comparison of clock
drawings is shown in Appendix C, reflecting somewhat improved spatial construction and ability to attend to the
left side of an array during the post-treatment assessment, as shown by placement of the numbers. Although
quality of hand placement remained somewhat anomalous and vague, three of three naïve judges (students
completing clinical rotations in the rehabilitation department) selected the post-treatment drawing as
qualitatively better. It is the opinion of this clinician that the test instructions, “….set the hands at ten minutes
after 12”, may result in a product which is less sensitive in revealing right hemisphere deficits, since both the 12
and the 2 are situated at, or to the right of midline. Instructions for the clock drawing task on the Cognitive
Linguistic Quick Test (Estabrooks, 2001) specify hand placement at ten minutes after eleven, which may be a
position more likely to reveal neglect or inattention to the left hemispace.
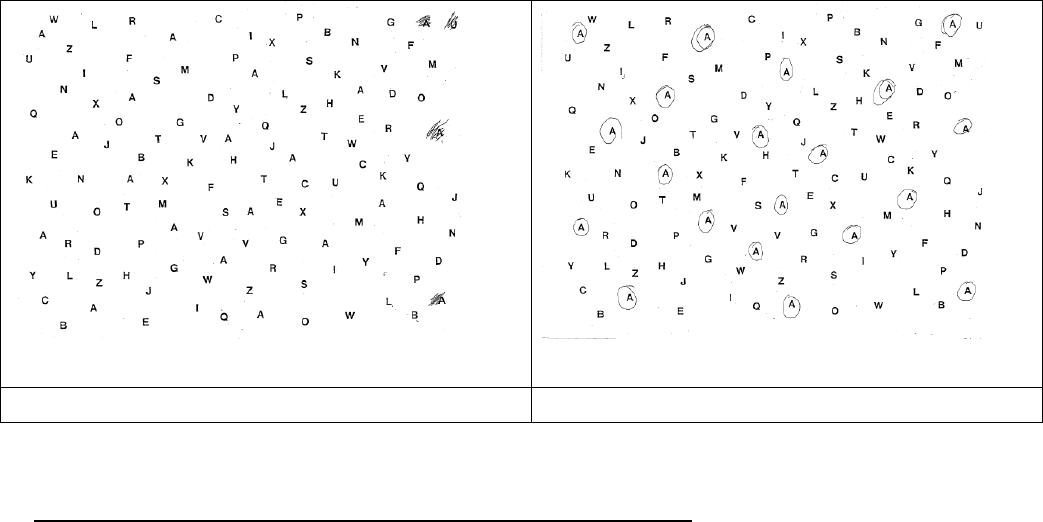
The scanning subtest from the Arizona Battery for Communication Disorders of Dementia (Bayles &
Tomoeda, 1993) was utilized as an additional qualitative measure of outcome. During the baseline attempt of
this task, XX located only three targets on the far right of the array, and then stated, “There. That’s all.” As
shown by Figure 4, performance in the post-treatment condition was significantly improved. XX identified all
the relevant targets, without any errors of commission; and, although her scanning behavior included a
Sample Case Study
13
combination of left to right, and right to left, search patterns, she did initiate self-checking behaviors and the
final product does not reflect inattention to the left side of the array.
Pre-treatment
Post-treatment
Figure 4: Comparison of pre- and post-treatment cancellation task response
6) Rationale for Termination of Treatment and Follow-up Recommendations
Continued direct intervention by speech-language pathology was recommended upon transfer to the
skilled nursing (SNF) setting. Handoff of care took place via an exchange of medical records including the report
of evaluation, weekly progress notes and a discharge summary. Due to HIPAA guidelines which limit ongoing
direct communication with subsequent treating clinicians, it is unknown as to the length of time XX remained in
the SNF setting, and whether or not treatment continues on a home care or outpatient basis at the present
time. Given the current nature of the healthcare environment, including the capitated payment system in place
for outpatient rehabilitation care, and the length of time post-onset, it is believed likely that formal intervention
is not continuing at this time. Had XX received ongoing care from this clinician, discharge from direct treatment
would have been recommended in any of several circumstances: 1) upon request from XX and/or her caregivers;
2) upon successful completion of the course of care, such that goals were attained; or, 3) evidence that direct
treatment was no longer beneficial in supporting progress toward improved function. Use of the ASHA National

Sample Case Study
14
Outcome System (NOMS) which is based on performance on up to 15 Functional Communication Measures
(FCMs) (ASHA, n.d.) is suggested as an appropriate choice for a tool to track and document progress in a SNF,
home care or outpatient setting as it has the ability to track performance across multiple skills targeted in
rehabilitation of RHD, including attention, reading, writing and pragmatic skills.
7) Neurologic Considerations
The left cerebral hemisphere is generally considered to be the dominant hemisphere, with respect to
language functioning, in the majority of individuals (Bhatnager, 2012). Given that XX was right-handed, and that
her conversational language was free of word-finding difficulty and other signs of aphasia, the assessment that
the stroke affected her non-language-dominant hemisphere appears to be supported.
The thalamus, a structure involved in XX’s stroke, is a large midline subcortical gray matter structure
containing various sensory nuclei, including the lateral geniculate nucleus (LGN) which carries visual information,
and the ventral posterolateral nucleus, which is associated with somatosensation (Bhatnager, 2012). The
thalamus receives its blood supply from the P1 branch of the posterior cerebral artery which was occluded in
this individual’s stroke. In the absence of damage to the primary somatosensory cortex in the parietal lobe, the
involvement of the thalamus within the cerebral territory affected by her stroke would account, at least in part,
for XX’s identified deficits in somatosensation. Right-sided thalamic lesions have also been associated with the
phenomenon of alien hand syndrome (Ventura, Goldman & Hildebrand, 1995; Sarva, Deik & Severt, 2014),
providing a physiologic basis for this finding as well. XX presented with left hand movements she perceived
were not under her control, sustained grasping of objects, and hyper-extended posturing of her fingers. These
behaviors are associated with a posterior variant of alien hand syndrome. (Sarva, Deik, & Severt, 2014; Pack,
Stewart, Diamond, & Gale, 2002).
Damage to the LGN, which is also supplied by the posterior cerebral artery, has been associated with the
findings of visual field deficit and neglect (Luco, Hope, Schweitzer, Vicuña & Fantin, 1992; Schmahmann, 2003).

Sample Case Study
15
The behaviors resulting from field cuts and neglect are similar, often co-exist, and can be challenging to
distinguish. (Parton, Malhotra & Husein, 2004) It is the opinion of this clinician that both were likely present to
some degree in this case, based on lesion size and locations, along with observed behaviors on tasks of drawing
and cancellation, along with failures of leftward attention in basic route finding and basic reading.
The temporal lobes are home to the fusiform face area (FFA), an area also supplied by the P1 branch of
the posterior cerebral artery. This region is located on the ventromedial aspect of the temporal lobes,
bilaterally. Facial recognition is a skill for which there has been shown to be a functional unilateral difference in
cerebral physiology, with heightened activity in the right FFA during tasks of facial recognition (Kanwisher &
Yovel, 2006). Disordered facial recognition, referred to as prosopagnosia, is often associated with right-
hemisphere damage, and XX’s performance on the facial recognition subtest of the Burns Inventory reflected
some degree of difficulty with facial recognition skills.
Myers (1999), states that anosognosia is consistently associated with frontal and/or parietal sites of
lesion. The fact that XX’s stroke spared right frontal and right parietal regions is felt to account for the fact that
anosognosia, or denial of deficit, was not an observed behavior. Dysarthria was also an unlikely finding, since
XX’s lesion did not involve the right frontal lobe, basal ganglia or brainstem.
8) Quality Assessment Statement
A query of the database for the inpatient rehabilitation unit where XX received care showed that 45% of
individuals with unilateral CVA on the speech-language pathology caseload presented with right hemisphere
CVA, so with regards to the underlying etiologic diagnosis, this case is typical of the caseload seen by this writer.
Analysis of the database also shows that this case is fairly typical from the standpoint of the length of stay and
discharge disposition. An atypical aspect of this case is the unusual and infrequently encountered finding of
alien hand symptoms which raised the curiosity of this writer and invited closer inspection.

Sample Case Study
16
In retrospect, and after additional reading related to this particular case, deep testing of various abilities
would be informative, and the results could contribute to future treatment decisions. Further testing would
include detailed assessment of facial matching and facial identification/naming skills, and comparison of object
naming with facial naming. Deeper testing of discourse comprehension (Blake, 2015; Tompkins, 2008), and
production (Blake, 2015) would also be appropriate, especially as some of the visual attention challenges with
potential to limit safe independence resolved. Blake (2015) suggested several tasks useful for expanded testing,
including elicitation of expository speech sample via a response to the Cookie Theft task on the Boston
Diagnostic Aphasia Examination (Goodglass, Kaplan & Barresi, 2001) or similar picture, with analysis specific to
organization, efficiency, gist, and quantity; and use of the Functional Assessment of Verbal Reasoning and
Executive Strategies (FAVRES) (MacDonald, 2005). Assessment using a measure of functional communication
such as the Communication Abilities of Daily Living (CADL-2) (Holland, Frattali and Fromm, 1999) could also be
informative, especially in determining readiness for return to home or transition to an assisted- living setting.
A fair evaluation of this case would recognize that XX was receiving care in the early stages of recovery
from her CVA, and some might say that improvement in function could be attributed to the natural course of
recovery. In the experience of this clinician, families, and even some healthcare providers overlook the
cognitive-communicative deficits of people with RHD, due a focus on recovery of mobility skills. Early,
individualized and evidence-based intervention can identify deficits and help people move more quickly and
safely down the road of recovery, perhaps preventing development of counterproductive behaviors along the
way.
It is the opinion of this writer that treatment contributed to favorable improvement in activities relevant
to safe independence such as survival skill reading and way-finding in living surroundings. Qualitative and
quantitative measures support this claim. Additionally, XX verbalized increased confidence related to her
performance over the course of her care. The visual analog tool used to document this finding will be shared

Sample Case Study
17
during the oral presentation of this case. Although interventions by this discipline should not be considered as
treatment for alien hand syndrome, XX reported gradual reduction in the frequency and intensity of these
uncomfortable perceptions over the course of her stay in the IRF setting. While XX was not immediately able to
return home following her IRF stay due to family circumstances which prevented supervision at least during
nighttime hours, improvements in mobility and visual perceptual functioning lessened her burden of care and
increased the likelihood of an eventual return to her home.

Sample Case Study
18
References
Adams, H., Davis, P., Leira, E., Chang, K., Bendixen, B., Clark, W., . . .Hansen, M. (1999). Baseline NIH Stroke Scale score
strongly predicts outcome after stroke: A report of the Trial of Org 10172 in Acute Stroke Treatment (TOAST).
Neurology, 53(1): 126-131.
American Speech-Language-Hearing Association. (n.d.) National Outcomes Measurement System (NOMS).
Retrieved 07/02/15 from http://www.asha.org/NOMS/.
Barrett, A. (2000). Treatment of unilateral neglect in patients with right hemisphere brain damage. Perspectives on
Neurophysiology & Neurogenic Speech & Language Disorders, 10(4), 18-26. doi:10.1044/nnsld10.4.18. Bhatnagar, S.
(2012). Neuroscience for the study of communicative disorders, 4
th
ed. Philadelphia, PA: Lippincott
Williams & Wilkins.
Bayles, K., and Tomoeda, C. (1993). Arizona battery of communication disorders of dementia. Austin, TX: Pro-Ed, Inc.
Blake, M. (2007, November). Treatment for cognitive-communication deficits after right brain damage in the absence
of evidence. Presented at the American Speech-Language-Hearing Association Convention, Boston, MA.
Blake, M. (2015, November). Right hemisphere communication disorders: Current knowledge and best practices.
Presented at the American Speech-Language-Hearing Association Convention, Denver, CO.
Blake, M. (2008). CE Introduction, Perspectives on Neurophysiology & Neurogenic Speech & Language Disorders, 18
(2): 42-42.
Blake, M.L., (2006). Clinical relevance of discourse characteristics after right hemisphere brain damage. America
Journal of Speech-Language Pathology, 15, 255-267.
Burns, M. (1997). Burns brief inventory of communication and cognition: Right hemisphere inventory. San Antonio,
TX: The Psychological Corporation.
Cherney, L., Halper, A., Kwasnica, C., Harvey, R., and Zhang, M. (2001). Recovery of functional status after right
hemisphere stroke: relationship with unilateral neglect. Archives of Physical Medicine and Rehabilitation.
82(3):322-8.
Gandola, M., Invernizzi, P., Sedda, A., Ferrè, E., Sterzi, R., Sberna, M., Paulesu, E., Bottini, G. (2012). An
anatomical account of somatoparaphrenia. Cortex 48(9):1165–1178.
Goodglass, H., Kaplan, E., and Barresi, B. (2001). Boston Diagnostic Aphasia Examination (3
rd
ed.). Austin, TX:
Pro-Ed, Inc.
González, R., Furie, K., Goldmacher, G., Smith, W., Kamalian, S., Payabvash, S., . . . Lev, M. (2013). Good outcome rate of
35% in IV-tPA–treated patients with computed tomography angiography confirmed severe anterior circulation
occlusive stroke. Stroke 44: 3109-3113.
Hegde, M. (2006). A coursebook on aphasia and other neurogenic language disorders (3
rd
ed.). Clifton Park, NY:
Delmar Cengage Learning.

Sample Case Study
19
Helm-Estabrooks, N. (2001). Cognitive linguistic quick test. San Antonio, TX: Psychological Corporation.
Helm-Estabrooks, N., Martin, L., and Nicholas, M. (2014). Manual of aphasia and aphasia therapy. Austin, TX: Pro-
Ed, Inc.
Hillis, A. (2006). Rehabilitation of unilateral spatial neglect: New insights from magnetic resonance perfusion imaging.
Archives of Physical Medicine and Rehabilitation, 87(12 Suppl 2), S43-49.
Holland, A., Frattali, C., and Fromm, D. (1999) Communication activities of daily living (CADL-2) (2
nd
ed.). Austin, TX:
Pro- Ed, Inc.
Kanwisher, N., and Yovel, G. (2006). The fusiform face area: A cortical region specialized for the perception of faces.
Philosophical Transactions of the Royal Society of London, Series B, 361(1476), 2109-2128.
Lindsberg, P., Soinne, L., Tatlisumak, T., Roine, R., Kallela, M., Häppölä, O., Kaste, M. (2004). Long-term outcome after
intravenous thrombolysis of basilar artery occlusion. JAMA 292(15):1862-1866. doi:10.1001/jama.292.15.1862
Luco, C., Hopee, A., Schweitzer, V., Vicuña, X., and Fantin, A. (1992). Visual field defects in vascular lesions of the
lateral geniculate body. Journal of Neurology, Neurosurgery and Psychiatry, 55: 12-15.
MacDonald, S. (2005). Functional assessment of verbal reasoning and executive functions. Guelph, Ontario, Canada:
CCD Publications.
Myers, P. (1999). Right hemisphere damage: Disorders of communication and cognition. San Diego, CA: Singular
Publishing Group, Inc.
Myers, P., and Blake, M. (2008). “Communication disorders associated with right-hemisphere damage.” In Chapey, R.
(Ed.), Language Intervention Strategies for Adults With Aphasia and Related Neurogenic Communication Disorders
(pp. 279-298). Baltimore, MD: Lippincott, Williams & Wilkins.
Lansberg, M., O'Donnell, M., Khatri, P., Lang, E., Nguyen-Huynh, M., Schwartz, N., . . . Akl, E. (2012). Antithrombotic and
thrombolytic therapy for ischemic stroke: antithrombotic therapy and prevention of thrombosis, 9th ed: American
College of Chest Physicians evidence-based clinical practice guidelines. Chest, 141(2 Suppl):e601S-36S. Retrieved
from http://www.guideline.gov/content.aspx?id=35272.

Sample Case Study
20
Pack, B., Stewart, K., Diamond, P., & Gale, S. (2002). Posterior-variant alien hand
syndrome: Clinical features and
response to rehabilitation. Disability and Rehabilitation, 24(15): 817-
818.Parton, A., Malhotra, P., and Husein, M. (2004). Hemispatial neglect. Journal of Neurology Neurosurgery
and
Psychiatry, 75:13–21.
Sarva, H., Deik, A., & Severt, W. L. (2014). Pathophysiology and treatment of alien hand syndrome. Tremor and
Other Hyperkinetic Movements, 4, 241. http://doi.org/10.7916/D8VX0F48.
Rubens, A. (1985). Caloric stimulation and unilateral visual neglect. Neurology, 35(7):1019-24.
Schmahmann, J. (2003). Vascular syndromes of the thalamus. Stroke, 34(7): 2264-2278. doi:
10.1161/01.STR.0000087786.38997.9E
Tactus Therapy Solutions. (2012). Visual Attention Therapy. Vancouver, Canada: Tactus Therapy Solutions, Ltd.
Tompkins, C. (2008). Theoretical considerations for understanding “understanding” by adults with right hemisphere
brain damage. Perspectives on Neurophysiology & Neurogenic Speech & Language Disorders, 18 (2): 45-54.
UB Foundation Activities. (2012). Inpatient Rehabilitation Facility – Patient Assessment Instrument (IRF-PAI) Training
Manual. Available at http://www.cms.gov/Medicare/Medicare-Fee-for-Service-
Payment/InpatientRehabFacPPS/Downloads/IRFPAI-manual-2012.pdf .
Uniform Data System for Medical Rehabilitation (UDSMR). (2015). Retrieved from:
http://www.udsmr.org/WebModules/FIM/Fim_About.aspx.
Ventura, M., Goldman, S., Hildebrand, J. (1995). Alien hand syndrome without a corpus callosum lesion. Journal of
Neurology, Neurosurgery, and Psychiatry, 58:735-737.
Ward, J. (2015). The student’s guide to cognitive neuroscience, 3
rd
Ed. New York, NY: Psychology Press.
Warren, M. (2013). “Evaluation and treatment of visual deficits following brain injury.” In Pendelton, H., and Schultz-
Krohn, W. (Eds.), Pedretti’s Occupational Therapy: Practice Skills for Physical Dysfunction (7
th
ed.). (pp 590-630). St.
Louis: MO: Elsevier.
Warren, M. (1996). Pre-reading and writing exercises for persons with macular scotomas. Birmingham, AL:
visABILITIES Rehab Services, Inc.
World Health Organization. (2002). Towards a common language for functioning, disability, and health. Geneva,
Switzerland: World Health Organization.

Sample Case Study
21
Appendix A: Radiographic images
Axial 14 DWI
Coronal 5 DWI
15 Sagittal T1 FLAIR
Axial 15 DWI
Coronal 11 DWI
16 Sagittal T1 FLAIR
Axial 17 DWI
Coronal 18 DWI
18 Sagittal T1 FLAIR
Sample Case Study
22
Appendix B: Comparison of pre- and post-treatment scores on the Burns Brief Inventory of Communication and
Cognition: Right Hemisphere Inventory
Key: X = score on initial IRF assessment; ◼ = score at discharge from IRF setting

Sample Case Study
23
Appendix C: Comparison of pre- and post-treatment clock drawings on the Burns Brief Inventory of
Communication and Cognition: Right Hemisphere Inventory
Clock drawing during initial assessment:
Clock drawing during discharge assessment:
